There are many different ways of explaining mental health issues, and of explaining the factors that influence our health. Different models emphasise different aspects of mental health, such as the impact society and culture have on a person’s mental health.
It is important to note that there is more to mental health than whether or not a person has a diagnosis of an illness.
For the purposes of this website, I have selected the mental health continuum as a useful model to show that mental health changes over time and that mental health issues are about everyone (I learnt about the mental health continuum as part of the Scotland’s Mental Health First Aid course).
Other models of health and mental health are briefly described below.
Trauma Model of Mental Disorders
You can read about the Trauma Model of Mental Disorder here.
Dahlgren and Whitehead Model
After the mental health continuum, another popular model to give an overview of one alternative way of considering health is the model by Dahlgren and Whitehead (1991).
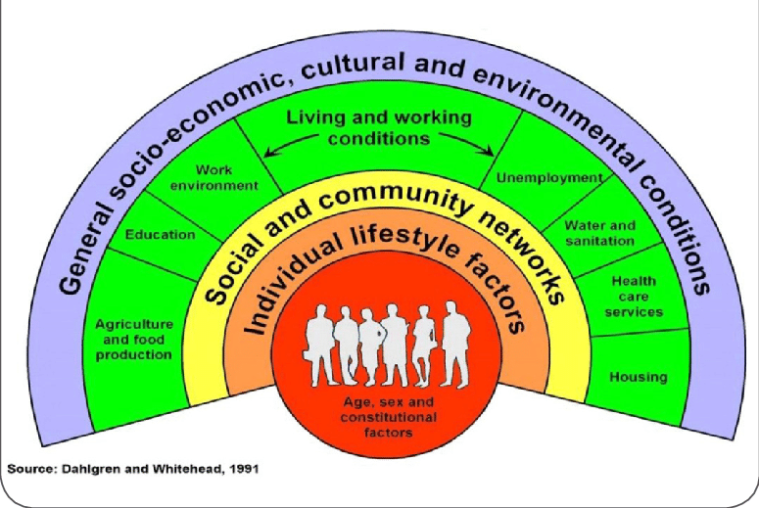
This model pays closer attention to the impact of lifestyle, social, economic circumstances, culture, and the environment. It attempts to show how these things influence an individual’s health and how they interact with one another.
The model shows that health is affected by a range of different factors, from those specific to the individual, to wider cultural and social issues.
An individual’s health will be influenced by their gender, age, by their individual personality, and relative strength or resilience. However, health is much more than individual factors. A person’s health is affected by their local community and the extent to which they have sense of belonging. Education, work, the ability to access and prepare healthy food, housing and sanitation are also significant factors, as are economic, cultural, and environmental conditions.
This model is useful for considering the extent to which a person has control over their own health, and how much health improvement needs to be driven by policy that recognises the impact of all these factors.
The model also acts as an important reminder that health is not purely about the individual. It is therefore unhelpful and misguided to blame those who are experiencing poor health.
Kinderman’s Psychological Model of Mental Disorder
A coherent conceptualisation of the role of psychological factors is of great importance in understanding mental disorder (Kinderman, 2005). Academic articles and professional reports alluding to psychological models of the aetiology of mental disorder are becoming increasingly common, and there is evidence of a marked policy shift toward the provision of psychological therapies and interventions.
This article discusses the relationship between biological, social, and psychological factors in the causation and treatment of mental disorder. It argues that simple biological reductionism is not scientifically justified, and also that the specific role of psychological processes within the biopsychosocial model requires further elaboration. The biopsychosocial model is usually interpreted as implying that biological, psychological, and social factors are co-equal partners in the aetiology of mental disorder.
The psychological model of mental disorder presented here suggests that disruption or dysfunction in psychological processes is a final common pathway in the development of mental disorder. These processes include, but are not limited to, cognitive processes.
The model proposes that biological and social factors, together with a person’s individual experiences, lead to mental disorder through their conjoint effects on those psychological processes. Implications for research, interventions, and policy are discussed.
The Biopsychosocial Model
The biopsychosocial approach was developed at Rochester decades ago by Dr’s. George Engel and John Romano, and published in 1977 (Engel, 1977; Frankel et al., 2003). While traditional biomedical models of clinical medicine focus on pathophysiology and other biological approaches to disease, the biopsychosocial approach emphasises the importance of understanding human health and illness in their fullest contexts. The biopsychosocial approach systematically considers biological, psychological, and social factors and their complex interactions in understanding health, illness, and health care delivery.
- Biological, psychological, and social factors exist along a continuum of natural systems, as depicted in the diagram above.
- Systematic consideration of psychological and social factors requires application of relevant social sciences, just as consideration of biological factors requires application of relevant natural sciences. Therefore, both the natural and social sciences are ‘basic’ to medical practice. In other words, psychological and social factors are not merely epiphenomena: they can be understood in scientific ways at their own levels as well as in regard to their biological correlates.
- Humanistic qualities are highly valued complements to the biopsychosocial approach, which involves the application of the scientific method to diverse biological, psychological, and social phenomena as related to human health.
- While the biomedical approach takes the reductionistic view that all phenomena are best understood at the lowest level of natural systems (e.g., cellular or molecular), the biopsychosocial approach recognises that different clinical scenarios may be most usefully understood scientifically at several levels of the natural systems continuum.
To apply the biopsychosocial approach to clinical practice, the clinician should (Engel, 1980):
- Recognise that relationships are central to providing health care.
- Use self-awareness as a diagnostic and therapeutic tool.
- Elicit the patient’s history in the context of life circumstances.
- Decide which aspects of biological, psychological, and social domains are most important to understanding and promoting the patient’s health.
- Provide multidimensional treatment.
Rethinking the Biopsychosocial Model of Health
In 2017, Lehman colleagues suggested that the biopsychosocial model had dominated research and theory in health psychology. Their 2017 article expanded the biopsychosocial model by applying systems theories proposed by developmental scholars, including Bronfenbrenner’s ecological models and Sameroff’s transactional model, as well as contemporary philosophical work on dynamic systems. The proposed dynamic biopsychosocial model construed human health as a product of the reciprocal influences of biological, psychological, interpersonal, and macrosystem contextual dynamics that unfold over personal and historical time. The importance, or centrality, of these influences varies within a person over time. The model is explicated using two hypothetical case studies derived from existing interdisciplinary health research. Implications for health, theory, research, and policy are discussed.
The Biomedical Model of Mental Disorder
Deacon (2013) states that the biomedical model posits that mental disorders are brain diseases and emphasises pharmacological treatment to target presumed biological abnormalities.
A biologically-focused approach to science, policy, and practice has dominated the American healthcare system for more than three decades. During this time, the use of psychiatric medications has sharply increased and mental disorders have become commonly regarded as brain diseases caused by chemical imbalances that are corrected with disease-specific drugs.
However, despite widespread faith in the potential of neuroscience to revolutionise mental health practice, the biomedical model era has been characterised by a broad lack of clinical innovation and poor mental health outcomes.
In addition, the biomedical paradigm has profoundly affected clinical psychology via the adoption of drug trial methodology in psychotherapy research. Although this approach has spurred the development of empirically supported psychological treatments for numerous mental disorders, it has neglected treatment process, inhibited treatment innovation and dissemination, and divided the field along scientist and practitioner lines.
The neglected biopsychosocial model represents an appealing alternative to the biomedical approach, and an honest and public dialog about the validity and utility of the biomedical paradigm is urgently needed.
References
Dahlgren, G. & Whitehead, M. (1991) Policies and Strategies to Promote Social Equality in Health. Stockholm: Institute for Future Studies.
Deacon, B.J. (2013) The Biomedical Model of Mental Disorder: A Critical Analysis of its Validity, Utility, and Effects on Psychotherapy Research. Clinical Psychology Review. 33, pp.846-861.
Engel, G.L. (1977) The Need for a New Medical Model: A Challenge for Biomedicine. Science. 196, pp.129-136.
Engel, G.L. (1980) The Clinical Application of the Biopsychosocial Model. American Journal of Psychiatry. 137, pp.535-544.
Frankel, R.M., Quill, T.E. & McDaniel, S.H. (Eds). (2003) The Biopsychosocial Approach: Past, Present, Future. Rochester, New York: University of Rochester Press.
Kinderman, P. (2005) A Psychological Model of Mental Disorder. Harvard Review of Psychiatry. 13(4), pp.206-217.
Lehman, B.J., David, D.M. & Gruber, J.A. (2017) Rethinking the Biopsycholosocial Model of Health: Understanding Health as a Dynamic System. Social and Personality Psychology Compass. 11(8).
