Psychoneuroimmunology (PNI), also referred to as psychoendoneuroimmunology (PENI) or psychoneuroendocrinoimmunology (PNEI), is the study of the interaction between psychological processes and the nervous and immune systems of the human body. It is a subfield of psychosomatic medicine. PNI takes an interdisciplinary approach, incorporating psychology, neuroscience, immunology, physiology, genetics, pharmacology, molecular biology, psychiatry, behavioural medicine, infectious diseases, endocrinology, and rheumatology.
The main interests of PNI are the interactions between the nervous and immune systems and the relationships between mental processes and health. PNI studies, among other things, the physiological functioning of the neuroimmune system in health and disease; disorders of the neuroimmune system (autoimmune diseases; hypersensitivities; immune deficiency); and the physical, chemical and physiological characteristics of the components of the neuroimmune system in vitro, in situ, and in vivo.
Brief History
Interest in the relationship between psychiatric syndromes or symptoms and immune function has been a consistent theme since the beginning of modern medicine.
Claude Bernard, a French physiologist of the Muséum national d’Histoire naturelle (National Museum of Natural History in English), formulated the concept of the milieu interieur in the mid-1800s. In 1865, Bernard described the perturbation of this internal state: “… there are protective functions of organic elements holding living materials in reserve and maintaining without interruption humidity, heat and other conditions indispensable to vital activity. Sickness and death are only a dislocation or perturbation of that mechanism” (Bernard, 1865). Walter Cannon, a professor of physiology at Harvard University coined the commonly used term, homeostasis, in his book The Wisdom of the Body, 1932, from the Greek word homoios, meaning similar, and stasis, meaning position. In his work with animals, Cannon observed that any change of emotional state in the beast, such as anxiety, distress, or rage, was accompanied by total cessation of movements of the stomach (Bodily Changes in Pain, Hunger, Fear and Rage, 1915). These studies looked into the relationship between the effects of emotions and perceptions on the autonomic nervous system, namely the sympathetic and parasympathetic responses that initiated the recognition of the freeze, fight or flight response. His findings were published from time to time in professional journals, then summed up in book form in The Mechanical Factors of Digestion, published in 1911.
Hans Selye, a student of Johns Hopkins University and McGill University, and a researcher at Université de Montréal, experimented with animals by putting them under different physical and mental adverse conditions and noted that under these difficult conditions the body consistently adapted to heal and recover. Several years of experimentation that formed the empiric foundation of Selye’s concept of the General Adaptation Syndrome. This syndrome consists of an enlargement of the adrenal gland, atrophy of the thymus, spleen, and other lymphoid tissue, and gastric ulcerations.
Selye describes three stages of adaptation, including an initial brief alarm reaction, followed by a prolonged period of resistance, and a terminal stage of exhaustion and death. This foundational work led to a rich line of research on the biological functioning of glucocorticoids.
Mid-20th century studies of psychiatric patients reported immune alterations in psychotic individuals, including lower numbers of lymphocytes and poorer antibody response to pertussis vaccination, compared with nonpsychiatric control subjects. In 1964, George F. Solomon, from the University of California in Los Angeles, and his research team coined the term “psychoimmunology” and published a landmark paper: “Emotions, immunity, and disease: a speculative theoretical integration.”
Origins
In 1975, Robert Ader and Nicholas Cohen, at the University of Rochester, advanced PNI with their demonstration of classic conditioning of immune function, and they subsequently coined the term “psychoneuroimmunology”. Ader was investigating how long conditioned responses (in the sense of Pavlov’s conditioning of dogs to drool when they heard a bell ring) might last in laboratory rats. To condition the rats, he used a combination of saccharin-laced water (the conditioned stimulus) and the drug Cytoxan, which unconditionally induces nausea and taste aversion and suppression of immune function. Ader was surprised to discover that after conditioning, just feeding the rats saccharin-laced water was associated with the death of some animals and he proposed that they had been immunosuppressed after receiving the conditioned stimulus. Ader (a psychologist) and Cohen (an immunologist) directly tested this hypothesis by deliberately immunising conditioned and unconditioned animals, exposing these and other control groups to the conditioned taste stimulus, and then measuring the amount of antibody produced. The highly reproducible results revealed that conditioned rats exposed to the conditioned stimulus were indeed immunosuppressed. In other words, a signal via the nervous system (taste) was affecting immune function. This was one of the first scientific experiments that demonstrated that the nervous system can affect the immune system.
In the 1970s, Hugo Besedovsky, Adriana del Rey and Ernst Sorkin, working in Switzerland, reported multi-directional immune-neuro-endocrine interactions, since they show that not only the brain can influence immune processes but also the immune response itself can affect the brain and neuroendocrine mechanisms. They found that the immune responses to innocuous antigens triggers an increase in the activity of hypothalamic neurons and hormonal and autonomic nerve responses that are relevant for immunoregulation and are integrated at brain levels. On these bases, they proposed that the immune system acts as a sensorial receptor organ that, besides its peripheral effects, can communicate to the brain and associated neuro-endocrine structures its state of activity. These investigators also identified products from immune cells, later characterised as cytokines, that mediate this immune-brain communication.
In 1981, David L. Felten, then working at the Indiana University School of Medicine, and his colleague JM Williams, discovered a network of nerves leading to blood vessels as well as cells of the immune system. The researchers also found nerves in the thymus and spleen terminating near clusters of lymphocytes, macrophages, and mast cells, all of which help control immune function. This discovery provided one of the first indications of how neuro-immune interaction occurs.
Ader, Cohen, and Felten went on to edit the groundbreaking book Psychoneuroimmunology in 1981, which laid out the underlying premise that the brain and immune system represent a single, integrated system of defence.
In 1985, research by neuropharmacologist Candace Pert, of the National Institutes of Health at Georgetown University, revealed that neuropeptide-specific receptors are present on the cell walls of both the brain and the immune system. The discovery that neuropeptides and neurotransmitters act directly upon the immune system shows their close association with emotions and suggests mechanisms through which emotions, from the limbic system, and immunology are deeply interdependent. Showing that the immune and endocrine systems are modulated not only by the brain but also by the central nervous system itself affected the understanding of emotions, as well as disease.
Contemporary advances in psychiatry, immunology, neurology, and other integrated disciplines of medicine has fostered enormous growth for PNI. The mechanisms underlying behaviourally induced alterations of immune function, and immune alterations inducing behavioural changes, are likely to have clinical and therapeutic implications that will not be fully appreciated until more is known about the extent of these interrelationships in normal and pathophysiological states.
The Immune-Brain Loop
PNI research looks for the exact mechanisms by which specific neuroimmune effects are achieved. Evidence for nervous-immunological interactions exist at multiple biological levels.
The immune system and the brain communicate through signalling pathways. The brain and the immune system are the two major adaptive systems of the body. Two major pathways are involved in this cross-talk: the Hypothalamic-pituitary-adrenal axis (HPA axis), and the sympathetic nervous system (SNS), via the sympathetic-adrenal-medullary axis (SAM axis). The activation of SNS during an immune response might be aimed to localise the inflammatory response.
The body’s primary stress management system is the HPA axis. The HPA axis responds to physical and mental challenge to maintain homeostasis in part by controlling the body’s cortisol level. Dysregulation of the HPA axis is implicated in numerous stress-related diseases, with evidence from meta-analyses indicating that different types/duration of stressors and unique personal variables can shape the HPA response. HPA axis activity and cytokines are intrinsically intertwined: inflammatory cytokines stimulate adrenocorticotropic hormone (ACTH) and cortisol secretion, while, in turn, glucocorticoids suppress the synthesis of proinflammatory cytokines.
Molecules called pro-inflammatory cytokines, which include interleukin-1 (IL-1), Interleukin-2 (IL-2), interleukin-6 (IL-6), Interleukin-12 (IL-12), Interferon-gamma (IFN-Gamma) and tumour necrosis factor alpha (TNF-alpha) can affect brain growth as well as neuronal function. Circulating immune cells such as macrophages, as well as glial cells (microglia and astrocytes) secrete these molecules. Cytokine regulation of hypothalamic function is an active area of research for the treatment of anxiety-related disorders.
Cytokines mediate and control immune and inflammatory responses. Complex interactions exist between cytokines, inflammation and the adaptive responses in maintaining homeostasis. Like the stress response, the inflammatory reaction is crucial for survival. Systemic inflammatory reaction results in stimulation of four major programmes:
The acute-phase reaction;
Sickness behaviour;
The pain programme; and
The stress response.
These are mediated by the HPA axis and the SNS. Common human diseases such as allergy, autoimmunity, chronic infections and sepsis are characterised by a dysregulation of the pro-inflammatory versus anti-inflammatory and T helper (Th1) versus (Th2) cytokine balance. Recent studies show pro-inflammatory cytokine processes take place during depression, mania and bipolar disease, in addition to autoimmune hypersensitivity and chronic infections.
Chronic secretion of stress hormones, glucocorticoids (GCs) and catecholamines (CAs), as a result of disease, may reduce the effect of neurotransmitters, including serotonin, norepinephrine and dopamine, or other receptors in the brain, thereby leading to the dysregulation of neurohormones. Under stimulation, norepinephrine is released from the sympathetic nerve terminals in organs, and the target immune cells express adrenoreceptors. Through stimulation of these receptors, locally released norepinephrine, or circulating catecholamines such as epinephrine, affect lymphocyte traffic, circulation, and proliferation, and modulate cytokine production and the functional activity of different lymphoid cells.
Glucocorticoids also inhibit the further secretion of corticotropin-releasing hormone from the hypothalamus and ACTH from the pituitary (negative feedback). Under certain conditions stress hormones may facilitate inflammation through induction of signalling pathways and through activation of the corticotropin-releasing hormone.
These abnormalities and the failure of the adaptive systems to resolve inflammation affect the well-being of the individual, including behavioural parameters, quality of life and sleep, as well as indices of metabolic and cardiovascular health, developing into a “systemic anti-inflammatory feedback” and/or “hyperactivity” of the local pro-inflammatory factors which may contribute to the pathogenesis of disease.
This systemic or neuro-inflammation and neuroimmune activation have been shown to play a role in the aetiology of a variety of neurodegenerative disorders such as Parkinson’s and Alzheimer’s disease, multiple sclerosis, pain, and AIDS-associated dementia. However, cytokines and chemokines also modulate central nervous system (CNS) function in the absence of overt immunological, physiological, or psychological challenges.
Psychoneuroimmunological Effects
There are now sufficient data to conclude that immune modulation by psychosocial stressors and/or interventions can lead to actual health changes. Although changes related to infectious disease and wound healing have provided the strongest evidence to date, the clinical importance of immunological dysregulation is highlighted by increased risks across diverse conditions and diseases. For example, stressors can produce profound health consequences. In one epidemiological study, all-cause mortality increased in the month following a severe stressor – the death of a spouse. Theorists propose that stressful events trigger cognitive and affective responses which, in turn, induce sympathetic nervous system and endocrine changes, and these ultimately impair immune function. Potential health consequences are broad, but include rates of infection HIV progression cancer incidence and progression, and high rates of infant mortality.
Understanding Stress and Immune Function
Stress is thought to affect immune function through emotional and/or behavioural manifestations such as anxiety, fear, tension, anger and sadness and physiological changes such as heart rate, blood pressure, and sweating. Researchers have suggested that these changes are beneficial if they are of limited duration, but when stress is chronic, the system is unable to maintain equilibrium or homeostasis; the body remains in a state of arousal, where digestion is slower to reactivate or does not reactivate properly, often resulting in indigestion. Furthermore, blood pressure stays at higher levels.
In one of the earlier PNI studies, which was published in 1960, subjects were led to believe that they had accidentally caused serious injury to a companion through misuse of explosives. Since then decades of research resulted in two large meta-analyses, which showed consistent immune dysregulation in healthy people who are experiencing stress.
In the first meta-analysis by Herbert and Cohen in 1993, they examined 38 studies of stressful events and immune function in healthy adults. They included studies of acute laboratory stressors (e.g. a speech task), short-term naturalistic stressors (e.g. medical examinations), and long-term naturalistic stressors (e.g. divorce, bereavement, caregiving, unemployment). They found consistent stress-related increases in numbers of total white blood cells, as well as decreases in the numbers of helper T cells, suppressor T cells, and cytotoxic T cells, B cells, and natural killer cells (NK). They also reported stress-related decreases in NK and T cell function, and T cell proliferative responses to phytohaemagglutinin [PHA] and concanavalin A [Con A]. These effects were consistent for short-term and long-term naturalistic stressors, but not laboratory stressors.
In the second meta-analysis by Zorrilla et al. in 2001, they replicated Herbert and Cohen’s meta-analysis. Using the same study selection procedures, they analysed 75 studies of stressors and human immunity. Naturalistic stressors were associated with increases in number of circulating neutrophils, decreases in number and percentages of total T cells and helper T cells, and decreases in percentages of natural killer cell (NK) cells and cytotoxic T cell lymphocytes. They also replicated Herbert and Cohen’s finding of stress-related decreases in NKCC and T cell mitogen proliferation to phytohaemagglutinin (PHA) and concanavalin A (Con A).
A study done by the American Psychological Association did an experiment on rats, where they applied electrical shocks to a rat, and saw how interleukin-1 was released directly into the brain. Interleukin-1 is the same cytokine released when a macrophage chews on a bacterium, which then travels up the vagus nerve, creating a state of heightened immune activity, and behavioural changes.
More recently, there has been increasing interest in the links between interpersonal stressors and immune function. For example, marital conflict, loneliness, caring for a person with a chronic medical condition, and other forms on interpersonal stress dysregulate immune function.
Communication between the Brain and Immune System
Stimulation of brain sites alters immunity (stressed animals have altered immune systems).
Damage to brain hemispheres alters immunity (hemispheric lateralisation effects).
Immune cells produce cytokines that act on the CNS.
Immune cells respond to signals from the CNS.
Communication between Neuroendocrine and Immune System
Glucocorticoids and catecholamines influence immune cells.
Hypothalamic Pituitary Adrenal axis releases the needed hormones to support the immune system.
Activity of the immune system is correlated with neurochemical/neuroendocrine activity of brain cells.
Connections between Glucocorticoids and Immune System
Anti-inflammatory hormones that enhance the organism’s response to a stressor.
Prevent the overreaction of the body’s own defence system.
Overactivation of glucocorticoid receptors can lead to health risks.
Regulators of the immune system.
Affect cell growth, proliferation and differentiation.
Cause immunosuppression which can lead to an extended amount of time fighting off infections.
High basal levels of cortisol are associated with a higher risk of infection.
Suppress cell adhesion, antigen presentation, chemotaxis and cytotoxicity.
Increase apoptosis.
Corticotropin-Releasing Hormone (CRH)
Release of corticotropin-releasing hormone (CRH) from the hypothalamus is influenced by stress.
CRH is a major regulator of the HPA axis/stress axis.
CRH Regulates secretion of adrenocorticotropic hormone (ACTH).
CRH is widely distributed in the brain and periphery
CRH also regulates the actions of the Autonomic nervous system ANS and immune system.
Furthermore, stressors that enhance the release of CRH suppress the function of the immune system; conversely, stressors that depress CRH release potentiate immunity.
Central mediated since peripheral administration of CRH antagonist does not affect immunosuppression.
HPA axis/stress axis responds consistently to stressors that are new, unpredictable and that have low-perceived control.
As cortisol reaches an appropriate level in response to the stressor, it deregulates the activity of the hippocampus, hypothalamus, and pituitary gland which results in less production of cortisol.
Relationships between Prefrontal Cortex Activation and Cellular Senescence
Psychological stress is regulated by the prefrontal cortex (PFC).
The PFC modulates vagal activity.
Prefrontally modulated and vagally mediated cholinergic input to the spleen reduces inflammatory responses.
Pharmaceutical Advances
Glutamate agonists, cytokine inhibitors, vanilloid-receptor agonists, catecholamine modulators, ion-channel blockers, anticonvulsants, GABA agonists (including opioids and cannabinoids), COX inhibitors, acetylcholine modulators, melatonin analogues (such as Ramelton), adenosine receptor antagonists and several miscellaneous drugs (including biologics like Passiflora edulis) are being studied for their psychoneuroimmunological effects.
For example, SSRIs, SNRIs and tricyclic antidepressants acting on serotonin, norepinephrine, dopamine and cannabinoid receptors have been shown to be immunomodulatory and anti-inflammatory against pro-inflammatory cytokine processes, specifically on the regulation of IFN-gamma and IL-10, as well as TNF-alpha and IL-6 through a psychoneuroimmunological process. Antidepressants have also been shown to suppress TH1 upregulation.
Tricyclic and dual serotonergic-noradrenergic reuptake inhibition by SNRIs (or SSRI-NRI combinations), have also shown analgesic properties additionally. According to recent evidences antidepressants also seem to exert beneficial effects in experimental autoimmune neuritis in rats by decreasing Interferon-beta (IFN-beta) release or augmenting NK activity in depressed patients.
These studies warrant investigation of antidepressants for use in both psychiatric and non-psychiatric illness and that a psychoneuroimmunological approach may be required for optimal pharmacotherapy in many diseases. Future antidepressants may be made to specifically target the immune system by either blocking the actions of pro-inflammatory cytokines or increasing the production of anti-inflammatory cytokines.
The endocannabinoid system appears to play a significant role in the mechanism of action of clinically effective and potential antidepressants and may serve as a target for drug design and discovery. The endocannabinoid-induced modulation of stress-related behaviours appears to be mediated, at least in part, through the regulation of the serotoninergic system, by which cannabinoid CB1 receptors modulate the excitability of dorsal raphe serotonin neurons. Data suggest that the endocannabinoid system in cortical and subcortical structures is differentially altered in an animal model of depression and that the effects of chronic, unpredictable stress (CUS) on CB1 receptor binding site density are attenuated by antidepressant treatment while those on endocannabinoid content are not.
The increase in amygdalar CB1 receptor binding following imipramine treatment is consistent with prior studies which collectively demonstrate that several treatments which are beneficial to depression, such as electroconvulsive shock and tricyclic antidepressant treatment, increase CB1 receptor activity in subcortical limbic structures, such as the hippocampus, amygdala and hypothalamus. And preclinical studies have demonstrated the CB1 receptor is required for the behavioural effects of noradrenergic based antidepressants but is dispensable for the behavioural effect of serotonergic based antidepressants.
Extrapolating from the observations that positive emotional experiences boost the immune system, Roberts speculates that intensely positive emotional experiences—sometimes brought about during mystical experiences occasioned by psychedelic medicines—may boost the immune system powerfully. Research on salivary IgA supports this hypothesis, but experimental testing has not been done.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Psychoneuroimmunology >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Neurohospitalist is a term used for physicians interested in inpatient neurological care.
It is an emerging subspecialty of neurology and a growing branch of neurology-internal medicine cross-functional care.
Journal
The Neurohospitalist is a quarterly, international, peer-reviewed journal dedicated to the practice and performance of neurohospitalist medicine.
The Neurohospitalist Society
The Neurohospitalist Society (NHS) was formed to create a central unifying organisation of neurohospitalists. Neurohospitalists are physicians and providers who care for hospitalised patients with, or at risk for, neurological disorders and disease.
History of the Neurohospitalist
In the early 2000s, “the term hospitalist was coined to describe specialists in internal medicine, whose focus was primarily on inpatient care.”
You can read about the “The Birth of Neurohospitalists” by William D. Freeman and S. Andrew Josephson here.
In the inaugural issue of The Neurohospitalist (January 2011), the authors sought to address 4 fundamental questions about neurohospitalists:
What is a neurohospitalist?
What fuelled the “birth” and growth of neurohospitalists?
What are the different functions of a neurohospitalist compared to other neurologists?; and
What areas of research will define this subspecialty (e.g. other than stroke and neurocritical care)?
What Illnesses do Neurohospitalists Treat?
Neurohospitalists see and treat a wide variety of illnesses ranging from autoimmune encephalitis to acute myasthenia gravis exacerbation, Guillain-Barre syndrome, refractory epilepsy, meningitis, headache, primary and secondary brain cancers, and delirium.
Neurology vs Neurohospitalist
In contrast to traditional neurology subspecialty practice that is outpatient-centred and disease specific, neurology hospitalists or “neurohospitalists” specialise in the care of patients admitted to the hospital with a wide array of nervous system disorders.
A neurohospitalist is (generally) a neurologist who has completed additional training to care for acutely ill, clinically complex patients with neurologic disease.
Neurology (from Greek: νεῦρον (neûron), “string, nerve” and the suffix -logia, “study of”) is the branch of medicine dealing with the diagnosis and treatment of all categories of conditions and disease involving the nervous system, which comprises the brain, the spinal cord and the peripheral nerves. Neurological practice relies heavily on the field of neuroscience, the scientific study of the nervous system.
A neurologist is a physician specialising in neurology and trained to investigate, diagnose and treat neurological disorders. Neurologists diagnose and treat myriad neurologic conditions, including stroke, epilepsy, movement disorders such as Parkinson’s disease, brain infections, autoimmune neurologic disorders such as multiple sclerosis, sleep disorders, brain injury, headache disorders like migraine, tumours of the brain and dementias such as Alzheimer’s disease. Neurologists may also have roles in clinical research, clinical trials, and basic or translational research. Neurology is a nonsurgical specialty, its corresponding surgical specialty is neurosurgery.
The academic discipline began between the 15th and 16th centuries with the work and research of many neurologists such as Thomas Willis, Robert Whytt, Matthew Baillie, Charles Bell, Moritz Heinrich Romberg, Duchenne de Boulogne, William A. Hammond, Jean-Martin Charcot, C. Miller Fisher and John Hughlings Jackson. Neo-Latin neurologia appeared in various texts from 1610 denoting an anatomical focus on the nerves (variably understood as vessels), and was most notably used by Willis, who preferred Greek νευρολογία.
Training
In the United States and Canada, neurologists are physicians who have completed a postgraduate training period known as residency specialising in neurology after graduation from medical school. This additional training period typically lasts four years, with the first year devoted to training in internal medicine. On average, neurologists complete a total of eight to ten years of training. This includes four years of medical school, four years of residency and an optional one to two years of fellowship.
While neurologists may treat general neurologic conditions, some neurologists go on to receive additional training focusing on a particular subspecialty in the field of neurology. These training programs are called fellowships, and are one to two years in duration. Subspecialties in the United States include brain injury medicine, clinical neurophysiology, epilepsy, neurodevelopmental disabilities, neuromuscular medicine, pain medicine, sleep medicine, neurocritical care, vascular neurology (stroke), behavioural neurology, child neurology, headache, neuroimmunology and infectious disease, movement disorders, neuroimaging, neurooncology, and neurorehabilitation.
In Germany, a compulsory year of psychiatry must be done to complete a residency of neurology.
In the United Kingdom and Ireland, neurology is a subspecialty of general (internal) medicine. After five years of medical school and two years as a Foundation Trainee, an aspiring neurologist must pass the examination for Membership of the Royal College of Physicians (or the Irish equivalent) and complete two years of core medical training before entering specialist training in neurology. Up to the 1960s, some intending to become neurologists would also spend two years working in psychiatric units before obtaining a diploma in psychological medicine. However, that was uncommon and, now that the MRCPsych takes three years to obtain, would no longer be practical. A period of research is essential, and obtaining a higher degree aids career progression. Many found it was eased after an attachment to the Institute of Neurology at Queen Square, London. Some neurologists enter the field of rehabilitation medicine (known as physiatry in the US) to specialise in neurological rehabilitation, which may include stroke medicine, as well as traumatic brain injuries.
Physical Examination
During a neurological examination, the neurologist reviews the patient’s health history with special attention to the patient’s neurologic complaints. The patient then takes a neurological exam. Typically, the exam tests mental status, function of the cranial nerves (including vision), strength, coordination, reflexes, sensation and gait. This information helps the neurologist determine whether the problem exists in the nervous system and the clinical localization. Localisation of the pathology is the key process by which neurologists develop their differential diagnosis. Further tests may be needed to confirm a diagnosis and ultimately guide therapy and appropriate management. Useful adjunct imaging studies in neurology include CT scanning and MRI. Other tests used to assess muscle and nerve function include nerve conduction studies and electromyography.
Clinical Tasks
Neurologists examine patients who are referred to them by other physicians in both the inpatient and outpatient settings. Neurologists begin their interactions with patients by taking a comprehensive medical history, and then performing a physical examination focusing on evaluating the nervous system. Components of the neurological examination include assessment of the patient’s cognitive function, cranial nerves, motor strength, sensation, reflexes, coordination, and gait.
In some instances, neurologists may order additional diagnostic tests as part of the evaluation. Commonly employed tests in neurology include imaging studies such as computed axial tomography (CAT) scans, magnetic resonance imaging (MRI), and ultrasound of major blood vessels of the head and neck. Neurophysiologic studies, including electroencephalography (EEG), needle electromyography (EMG), nerve conduction studies (NCSs) and evoked potentials are also commonly ordered. Neurologists frequently perform lumbar punctures to assess characteristics of a patient’s cerebrospinal fluid. Advances in genetic testing have made genetic testing an important tool in the classification of inherited neuromuscular disease and diagnosis of many other neurogenetic diseases. The role of genetic influences on the development of acquired neurologic diseases is an active area of research.
Some of the commonly encountered conditions treated by neurologists include headaches, radiculopathy, neuropathy, stroke, dementia, seizures and epilepsy, Alzheimer’s disease, attention deficit/hyperactivity disorder, Parkinson’s disease, Tourette’s syndrome, multiple sclerosis, head trauma, sleep disorders, neuromuscular diseases, and various infections and tumours of the nervous system. Neurologists are also asked to evaluate unresponsive patients on life support to confirm brain death.
Treatment options vary depending on the neurological problem. They can include referring the patient to a physiotherapist, prescribing medications, or recommending a surgical procedure.
Some neurologists specialise in certain parts of the nervous system or in specific procedures. For example, clinical neurophysiologists specialise in the use of EEG and intraoperative monitoring to diagnose certain neurological disorders. Other neurologists specialise in the use of electrodiagnostic medicine studies – needle EMG and NCSs. In the US, physicians do not typically specialize in all the aspects of clinical neurophysiology – i.e. sleep, EEG, EMG, and NCSs. The American Board of Clinical Neurophysiology certifies US physicians in general clinical neurophysiology, epilepsy, and intraoperative monitoring. The American Board of Electrodiagnostic Medicine certifies US physicians in electrodiagnostic medicine and certifies technologists in nerve-conduction studies. Sleep medicine is a subspecialty field in the US under several medical specialties including anaesthesiology, internal medicine, family medicine, and neurology. Neurosurgery is a distinct specialty that involves a different training path and emphasizes the surgical treatment of neurological disorders.
Also, many nonmedical doctors, those with doctoral degrees (usually PhDs) in subjects such as biology and chemistry, study and research the nervous system. Working in laboratories in universities, hospitals, and private companies, these neuroscientists perform clinical and laboratory experiments and tests to learn more about the nervous system and find cures or new treatments for diseases and disorders.
A great deal of overlap occurs between neuroscience and neurology. Many neurologists work in academic training hospitals, where they conduct research as neuroscientists in addition to treating patients and teaching neurology to medical students.
General Caseload
Neurologists are responsible for the diagnosis, treatment, and management of all the conditions mentioned above. When surgical or endovascular intervention is required, the neurologist may refer the patient to a neurosurgeon or an interventional neuroradiologist. In some countries, additional legal responsibilities of a neurologist may include making a finding of brain death when it is suspected that a patient has died. Neurologists frequently care for people with hereditary (genetic) diseases when the major manifestations are neurological, as is frequently the case. Lumbar punctures are frequently performed by neurologists. Some neurologists may develop an interest in particular subfields, such as stroke, dementia, movement disorders, neurointensive care, headaches, epilepsy, sleep disorders, chronic pain management, multiple sclerosis, or neuromuscular diseases.
Overlapping Areas
Some overlap also occurs with other specialties, varying from country to country and even within a local geographic area. Acute head trauma is most often treated by neurosurgeons, whereas sequelae of head trauma may be treated by neurologists or specialists in rehabilitation medicine. Although stroke cases have been traditionally managed by internal medicine or hospitalists, the emergence of vascular neurology and interventional neuroradiology has created a demand for stroke specialists. The establishment of Joint Commission-certified stroke centres has increased the role of neurologists in stroke care in many primary, as well as tertiary, hospitals. Some cases of nervous system infectious diseases are treated by infectious disease specialists. Most cases of headache are diagnosed and treated primarily by general practitioners, at least the less severe cases. Likewise, most cases of sciatica are treated by general practitioners, though they may be referred to neurologists or surgeons (neurosurgeons or orthopaedic surgeons). Sleep disorders are also treated by pulmonologists and psychiatrists. Cerebral palsy is initially treated by paediatricians, but care may be transferred to an adult neurologist after the patient reaches a certain age. Physical medicine and rehabilitation physicians may treat patients with neuromuscular diseases with electrodiagnostic studies (needle EMG and nerve-conduction studies) and other diagnostic tools. In the United Kingdom and other countries, many of the conditions encountered by older patients such as movement disorders, including Parkinson’s disease, stroke, dementia, or gait disorders, are managed predominantly by specialists in geriatric medicine.
Clinical neuropsychologists are often called upon to evaluate brain-behaviour relationships for the purpose of assisting with differential diagnosis, planning rehabilitation strategies, documenting cognitive strengths and weaknesses, and measuring change over time (e.g. for identifying abnormal ageing or tracking the progression of a dementia).
Relationship to Clinical Neurophysiology
In some countries such as the United States and Germany, neurologists may subspecialise in clinical neurophysiology, the field responsible for EEG and intraoperative monitoring, or in electrodiagnostic medicine nerve conduction studies, EMG, and evoked potentials. In other countries, this is an autonomous specialty (e.g. UK, Sweden, Spain).
In the past, prior to the advent of more advanced diagnostic techniques such as MRI some neurologists have considered psychiatry and neurology to overlap. Although mental illnesses are believed by many to be neurological disorders affecting the central nervous system, traditionally they are classified separately, and treated by psychiatrists. In a 2002 review article in the American Journal of Psychiatry, Professor Joseph B. Martin, Dean of Harvard Medical School and a neurologist by training, wrote:
“the separation of the two categories is arbitrary, often influenced by beliefs rather than proven scientific observations. And the fact that the brain and mind are one makes the separation artificial anyway”.
Neurological disorders often have psychiatric manifestations, such as post-stroke depression, depression and dementia associated with Parkinson’s disease, mood and cognitive dysfunctions in Alzheimer’s disease, and Huntington disease, to name a few. Hence, the sharp distinction between neurology and psychiatry is not always on a biological basis. The dominance of psychoanalytic theory in the first three-quarters of the 20th century has since then been largely replaced by a focus on pharmacology. Despite the shift to a medical model, brain science has not advanced to a point where scientists or clinicians can point to readily discernible pathological lesions or genetic abnormalities that in and of themselves serve as reliable or predictive biomarkers of a given mental disorder.
Neurological Enhancement
The emerging field of neurological enhancement highlights the potential of therapies to improve such things as workplace efficacy, attention in school, and overall happiness in personal lives. However, this field has also given rise to questions about neuroethics.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Neurology >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
The American Board of Psychiatry and Neurology, Inc. (ABPN) is a not-for-profit corporation that was founded in 1934 following conferences of committees appointed by the American Psychiatric Association, the American Neurological Association, and the then “Section on Nervous and Mental Diseases” of the American Medical Association. This action was taken as a method of identifying qualified specialists in psychiatry and neurology. The ABPN is one of 24 member boards of the American Board of Medical Specialties.
Organisation
The Board of Directors consists of sixteen voting members. Elections to fill the places of members whose terms have expired take place annually. Neurology and psychiatry are represented on the board. It is independently incorporated.
Certificates
In addition to the specialties of psychiatry, neurology, and neurology with a special qualification in child neurology, the ABPN (sometimes in collaboration with other member boards) has sought from the ABMS and gained approval for recognition of 15 sub-specialties, as listed below:
Addiction psychiatry
Brain injury medicine
Child and adolescent psychiatry
Clinical neurophysiology
Consultation-liaison psychiatry
Epilepsy
Forensic psychiatry
Geriatric psychiatry
Hospice and palliative medicine
Neurocritical care
Neurodevelopmental disabilities
Neuromuscular medicine
Pain medicine
Sleep medicine
Vascular neurology
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/American_Board_of_Psychiatry_and_Neurology >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
The transtheoretical model of behaviour change is an integrative theory of therapy that assesses an individual’s readiness to act on a new healthier behaviour, and provides strategies, or processes of change to guide the individual. The model is composed of constructs such as: stages of change, processes of change, levels of change, self-efficacy, and decisional balance.
The transtheoretical model is also known by the abbreviation “TTM” and sometimes by the term “stages of change”, although this latter term is a synecdoche since the stages of change are only one part of the model along with processes of change, levels of change, etc. Several self-help books—Changing for Good (1994), Changeology (2012), and Changing to Thrive (2016) – and articles in the news media have discussed the model. In 2009, an article in the British Journal of Health Psychology called it “arguably the dominant model of health behaviour change, having received unprecedented research attention, yet it has simultaneously attracted exceptional criticism”.
Brief History and Core Constructs
James O. Prochaska of the University of Rhode Island, and Carlo Di Clemente and colleagues developed the transtheoretical model beginning in 1977. It is based on analysis and use of different theories of psychotherapy, hence the name “transtheoretical”. Prochaska and colleagues refined the model on the basis of research that they published in peer-reviewed journals and books.
Stages of Change
This construct refers to the temporal dimension of behavioural change. In the transtheoretical model, change is a “process involving progress through a series of stages”:
Precontemplation (“not ready”) – “People are not intending to take action in the foreseeable future, and can be unaware that their behaviour is problematic”.
Contemplation (“getting ready”) – “People are beginning to recognize that their behaviour is problematic, and start to look at the pros and cons of their continued actions”.
Preparation (“ready”) – “People are intending to take action in the immediate future, and may begin taking small steps toward behaviour change”.
Action – “People have made specific overt modifications in modifying their problem behaviour or in acquiring new healthy behaviours”.
Maintenance – “People have been able to sustain action for at least six months and are working to prevent relapse”.
Termination – “Individuals have zero temptation and they are sure they will not return to their old unhealthy habit as a way of coping”.
In addition, the researchers conceptualised “Relapse” (recycling) which is not a stage in itself but rather the “return from Action or Maintenance to an earlier stage”.
The quantitative definition of the stages of change (see below) is perhaps the most well-known feature of the model. However it is also one of the most critiqued, even in the field of smoking cessation, where it was originally formulated. It has been said that such quantitative definition (i.e. a person is in preparation if he intends to change within a month) does not reflect the nature of behaviour change, that it does not have better predictive power than simpler questions (i.e. “do you have plans to change…”), and that it has problems regarding its classification reliability.
Communication theorist and sociologist Everett Rogers suggested that the stages of change are analogues of the stages of the innovation adoption process in Rogers’ theory of diffusion of innovations.
Details of Each Stage
Stage
Precontemplation
Contempplation
Preparation
Action
Maintenance
Relapse
Standard Time
More than 6 months
In the next 6 months
In the next month
Now
At least 6 months
Any time
Stage 1: Precontemplation (Not Ready)
People at this stage do not intend to start the healthy behaviour in the near future (within 6 months), and may be unaware of the need to change. People here learn more about healthy behaviour: they are encouraged to think about the pros of changing their behaviour and to feel emotions about the effects of their negative behaviour on others.
Precontemplators typically underestimate the pros of changing, overestimate the cons, and often are not aware of making such mistakes.
One of the most effective steps that others can help with at this stage is to encourage them to become more mindful of their decision making and more conscious of the multiple benefits of changing an unhealthy behaviour.
Stage 2: Contemplation (Getting Ready)
At this stage, participants are intending to start the healthy behaviour within the next 6 months. While they are usually now more aware of the pros of changing, their cons are about equal to their Pros. This ambivalence about changing can cause them to keep putting off taking action.
People here learn about the kind of person they could be if they changed their behaviour and learn more from people who behave in healthy ways.
Others can influence and help effectively at this stage by encouraging them to work at reducing the cons of changing their behaviour.
Stage 3: Preparation (Ready)
People at this stage are ready to start taking action within the next 30 days. They take small steps that they believe can help them make the healthy behaviour a part of their lives. For example, they tell their friends and family that they want to change their behaviour.
People in this stage should be encouraged to seek support from friends they trust, tell people about their plan to change the way they act, and think about how they would feel if they behaved in a healthier way. Their number one concern is: when they act, will they fail? They learn that the better prepared they are, the more likely they are to keep progressing.
Stage 4: Action (Current Action)
People at this stage have changed their behaviour within the last 6 months and need to work hard to keep moving ahead. These participants need to learn how to strengthen their commitments to change and to fight urges to slip back.
People in this stage progress by being taught techniques for keeping up their commitments such as substituting activities related to the unhealthy behaviour with positive ones, rewarding themselves for taking steps toward changing, and avoiding people and situations that tempt them to behave in unhealthy ways.
Stage 5: Maintenance (Monitoring)
People at this stage changed their behaviour more than 6 months ago. It is important for people in this stage to be aware of situations that may tempt them to slip back into doing the unhealthy behaviour—particularly stressful situations.
It is recommended that people in this stage seek support from and talk with people whom they trust, spend time with people who behave in healthy ways, and remember to engage in healthy activities (such as exercise and deep relaxation) to cope with stress instead of relying on unhealthy behaviour.
Relapse (Recycling)
Relapse in the TTM specifically applies to individuals who successfully quit smoking or using drugs or alcohol, only to resume these unhealthy behaviours. Individuals who attempt to quit highly addictive behaviours such as drug, alcohol, and tobacco use are at particularly high risk of a relapse. Achieving a long-term behaviour change often requires ongoing support from family members, a health coach, a physician, or another motivational source. Supportive literature and other resources can also be helpful to avoid a relapse from happening.
Processes of Change
The 10 processes of change are “covert and overt activities that people use to progress through the stages”.
To progress through the early stages, people apply cognitive, affective, and evaluative processes. As people move toward Action and Maintenance, they rely more on commitments, counter conditioning, rewards, environmental controls, and support.
Prochaska and colleagues state that their research related to the transtheoretical model shows that interventions to change behaviour are more effective if they are “stage-matched”, that is, “matched to each individual’s stage of change”.
In general, for people to progress they need:
A growing awareness that the advantages (the “pros”) of changing outweigh the disadvantages (the “cons”) – the TTM calls this decisional balance.
Confidence that they can make and maintain changes in situations that tempt them to return to their old, unhealthy behaviour – the TTM calls this self-efficacy.
Strategies that can help them make and maintain change – the TTM calls these processes of change.
The ten processes of change include:
Consciousness-raising (Get the facts) — increasing awareness via information, education, and personal feedback about the healthy behaviour.
Dramatic relief (Pay attention to feelings) — feeling fear, anxiety, or worry because of the unhealthy behaviour, or feeling inspiration and hope when hearing about how people are able to change to healthy behaviours.
Self-re-evaluation (Create a new self-image) — realising that the healthy behaviour is an important part of who they want to be.
Environmental re-evaluation (Notice your effect on others) — realizing how their unhealthy behaviour affects others and how they could have more positive effects by changing.
Social liberation (Notice public support) — realising that society is supportive of the healthy behaviour.
Self-liberation (Make a commitment) — believing in one’s ability to change and making commitments and re-commitments to act on that belief.
Helping relationships (Get support) — finding people who are supportive of their change.
Counterconditioning (Use substitutes) — substituting healthy ways of acting and thinking for unhealthy ways.
Reinforcement management (Use rewards) — increasing the rewards that come from positive behaviour and reducing those that come from negative behaviour.
Stimulus control (Manage your environment) — using reminders and cues that encourage healthy behaviour and avoiding places that do not.
Health researchers have extended Prochaska’s and DiClemente’s 10 original processes of change by an additional 21 processes. In the first edition of Planning Health Promotion Programmes, Bartholomew et al. (2006) summarised the processes that they identified in a number of studies; however, their extended list of processes was removed from later editions of the text, perhaps because the list mixes techniques with processes. There are unlimited ways of applying processes. The additional strategies of Bartholomew et al. were:
Risk comparison (Understand the risks) – comparing risks with similar dimensional profiles: dread, control, catastrophic potential and novelty
Cumulative risk (Get the overall picture) – processing cumulative probabilities instead of single incident probabilities
Qualitative and quantitative risks (Consider different factors) – processing different expressions of risk
Positive framing (Think positively) – focusing on success instead of failure framing
Self-examination relate to risk (Be aware of your risks) – conducting an assessment of risk perception, e.g. personalisation, impact on others
Re-evaluation of outcomes (Know the outcomes) – emphasising positive outcomes of alternative behaviours and re-evaluating outcome expectancies
Perception of benefits (Focus on benefits) – perceiving advantages of the healthy behaviour and disadvantages of the risk behaviour
Self-efficacy and social support (Get help) – mobilising social support; skills training on coping with emotional disadvantages of change
Decision making perspective (Decide) – focusing on making the decision
Tailoring on time horizons (Set the time frame) – incorporating personal time horizons
Focus on important factors (Prioritise) – incorporating personal factors of highest importance
Trying out new behaviour (Try it) – changing something about oneself and gaining experience with that behaviour
Persuasion of positive outcomes (Persuade yourself) – promoting new positive outcome expectations and reinforcing existing ones
Modelling (Build scenarios) – showing models to overcome barriers effectively
Skill improvement (Build a supportive environment) – restructuring environments to contain important, obvious and socially supported cues for the new behaviour
Coping with barriers (Plan to tackle barriers) – identifying barriers and planning solutions when facing these obstacles
Goal setting (Set goals) – setting specific and incremental goals
Skills enhancement (Adapt your strategies) – restructuring cues and social support; anticipating and circumventing obstacles; modifying goals
Dealing with barriers (Accept setbacks) – understanding that setbacks are normal and can be overcome
Self-rewards for success (Reward yourself) – feeling good about progress; reiterating positive consequences
Coping skills (Identify difficult situations) – identifying high risk situations; selecting solutions; practicing solutions; coping with relapse
While most of these processes and strategies are associated with health interventions such as stress management, exercise, healthy eating, smoking cessation and other addictive behaviour, some of them are also used in other types of interventions such as travel interventions. Some processes are recommended in a specific stage, while others can be used in one or more stages.
Decisional Balance
This core construct “reflects the individual’s relative weighing of the pros and cons of changing”. Decision making was conceptualised by Janis and Mann as a “decisional balance sheet” of comparative potential gains and losses. Decisional balance measures, the pros and the cons, have become critical constructs in the transtheoretical model. The pros and cons combine to form a decisional “balance sheet” of comparative potential gains and losses. The balance between the pros and cons varies depending on which stage of change the individual is in.
Sound decision making requires the consideration of the potential benefits (pros) and costs (cons) associated with a behaviour’s consequences. TTM research has found the following relationships between the pros, cons, and the stage of change across 48 behaviours and over 100 populations studied.
The cons of changing outweigh the pros in the Precontemplation stage.
The pros surpass the cons in the middle stages.
The pros outweigh the cons in the Action stage.
The evaluation of pros and cons is part of the formation of decisional balance. During the change process, individuals gradually increase the pros and decrease the cons forming a more positive balance towards the target behaviour. Attitudes are one of the core constructs explaining behaviour and behaviour change in various research domains. Other behaviour models, such as the theory of planned behaviour (TPB) and the stage model of self-regulated change, also emphasise attitude as an important determinant of behaviour. The progression through the different stages of change is reflected in a gradual change in attitude before the individual acts.
Due to the use of decisional balance and attitude, travel behaviour researchers have begun to combine the TTM with the TPB. Forward uses the TPB variables to better differentiate the different stages. Especially all TPB variables (attitude, perceived behaviour control, descriptive and subjective norm) are positively show a gradually increasing relationship to stage of change for bike commuting. As expected, intention or willingness to perform the behaviour increases by stage. Similarly, Bamberg uses various behaviour models, including the transtheoretical model, theory of planned behaviour and norm-activation model, to build the stage model of self-regulated behaviour change (SSBC). Bamberg claims that his model is a solution to criticism raised towards the TTM. Some researchers in travel, dietary, and environmental research have conducted empirical studies, showing that the SSBC might be a future path for TTM-based research.
Self-Efficacy
This core construct is “the situation-specific confidence people have that they can cope with high-risk situations without relapsing to their unhealthy or high risk-habit”. The construct is based on Bandura’s self-efficacy theory and conceptualises a person’s perceived ability to perform on a task as a mediator of performance on future tasks. In his research Bandura already established that greater levels of perceived self-efficacy leads to greater changes in behaviour. Similarly, Ajzen mentions the similarity between the concepts of self-efficacy and perceived behavioural control. This underlines the integrative nature of the transtheoretical model which combines various behaviour theories. A change in the level of self-efficacy can predict a lasting change in behaviour if there are adequate incentives and skills. The transtheoretical model employs an overall confidence score to assess an individual’s self-efficacy. Situational temptations assess how tempted people are to engage in a problem behaviour in a certain situation.
Levels of Change
This core construct identifies the depth or complexity of presenting problems according to five levels of increasing complexity. Different therapeutic approaches have been recommended for each level as well as for each stage of change. The levels are:
In one empirical study of psychotherapy discontinuation published in 1999, measures of levels of change did not predict premature discontinuation of therapy. Nevertheless, in 2005 the creators of the TTM stated that it is important “that both therapists and clients agree as to which level they attribute the problem and at which level or levels they are willing to target as they work to change the problem behavior”.
Psychologist Donald Fromme, in his book Systems of Psychotherapy, adopted many ideas from the TTM, but in place of the levels of change construct, Fromme proposed a construct called contextual focus, a spectrum from physiological microcontext to environmental macrocontext: “The horizontal, contextual focus dimension resembles TTM’s Levels of Change, but emphasizes the breadth of an intervention, rather than the latter’s focus on intervention depth.”
Outcomes of Programmes
The outcomes of the TTM computerised tailored interventions administered to participants in pre-Action stages are outlined below.
Stress Management
A national sample of pre-Action adults was provided a stress management intervention. At the 18-month follow-up, a significantly larger proportion of the treatment group (62%) was effectively managing their stress when compared to the control group. The intervention also produced statistically significant reductions in stress and depression and an increase in the use of stress management techniques when compared to the control group. Two additional clinical trials of TTM programmes by Prochaska et al. and Jordan et al. also found significantly larger proportions of treatment groups effectively managing stress when compared to control groups.
Adherence to Antihypertensive Medication
Over 1,000 members of a New England group practice who were prescribed antihypertensive medication participated in an adherence to antihypertensive medication intervention. The vast majority (73%) of the intervention group who were previously pre-Action were adhering to their prescribed medication regimen at the 12-month follow-up when compared to the control group.
Adherence to Lipid-Lowering Drugs
Members of a large New England health plan and various employer groups who were prescribed a cholesterol lowering medication participated in an adherence to lipid-lowering drugs intervention. More than half of the intervention group (56%) who were previously pre-Action were adhering to their prescribed medication regimen at the 18-month follow-up. Additionally, only 15% of those in the intervention group who were already in Action or Maintenance relapsed into poor medication adherence compared to 45% of the controls. Further, participants who were at risk for physical activity and unhealthy diet were given only stage-based guidance. The treatment group doubled the control group in the percentage in Action or Maintenance at 18 months for physical activity (43%) and diet (25%).
Depression Prevention
Participants were 350 primary care patients experiencing at least mild depression but not involved in treatment or planning to seek treatment for depression in the next 30 days. Patients receiving the TTM intervention experienced significantly greater symptom reduction during the 9-month follow-up period. The intervention’s largest effects were observed among patients with moderate or severe depression, and who were in the Precontemplation or Contemplation stage of change at baseline. For example, among patients in the Precontemplation or Contemplation stage, rates of reliable and clinically significant improvement in depression were 40% for treatment and 9% for control. Among patients with mild depression, or who were in the Action or Maintenance stage at baseline, the intervention helped prevent disease progression to Major Depression during the follow-up period.
Weight Management
Five-hundred-and-seventy-seven overweight or moderately obese adults (BMI 25-39.9) were recruited nationally, primarily from large employers. Those randomly assigned to the treatment group received a stage-matched multiple behaviour change guide and a series of tailored, individualized interventions for three health behaviours that are crucial to effective weight management: healthy eating (i.e. reducing calorie and dietary fat intake), moderate exercise, and managing emotional distress without eating. Up to three tailored reports (one per behaviour) were delivered based on assessments conducted at four time points: baseline, 3, 6, and 9 months. All participants were followed up at 6, 12, and 24 months. Multiple Imputation was used to estimate missing data. Generalized Labour Estimating Equations (GLEE) were then used to examine differences between the treatment and comparison groups. At 24 months, those who were in a pre-Action stage for healthy eating at baseline and received treatment were significantly more likely to have reached Action or Maintenance than the comparison group (47.5% vs. 34.3%). The intervention also impacted a related, but untreated behaviour: fruit and vegetable consumption. Over 48% of those in the treatment group in a pre-Action stage at baseline progressed to Action or Maintenance for eating at least 5 servings a day of fruit and vegetables as opposed to 39% of the comparison group. Individuals in the treatment group who were in a pre-Action stage for exercise at baseline were also significantly more likely to reach Action or Maintenance (44.9% vs. 38.1%). The treatment also had a significant effect on managing emotional distress without eating, with 49.7% of those in a pre-Action stage at baseline moving to Action or Maintenance versus 30.3% of the comparison group. The groups differed on weight lost at 24 months among those in a pre-Action stage for healthy eating and exercise at baseline. Among those in a pre-Action stage for both healthy eating and exercise at baseline, 30% of those randomised to the treatment group lost 5% or more of their body weight vs. 16.6% in the comparison group. Coaction of behaviour change occurred and was much more pronounced in the treatment group with the treatment group losing significantly more than the comparison group. This study demonstrates the ability of TTM-based tailored feedback to improve healthy eating, exercise, managing emotional distress, and weight on a population basis. The treatment produced the highest population impact to date on multiple health risk behaviours.
The effectiveness of the use of this model in weight management interventions (including dietary or physical activity interventions, or both, and also combined with other interventions) for overweight and obese adults was assessed in a 2014 systematic review. The results revealed that there is inconclusive evidence regarding the impact of these interventions on sustainable (one year or longer) weight loss. However, this approach may produce positive effects in physical activity and dietary habits, such as increased in both exercise duration and frequency, and fruits and vegetables consumption, along with reduced dietary fat intake, based on very low quality scientific evidence.
Criticisms
In 2009, an article in the British Journal of Health Psychology called the TTM “arguably the dominant model of health behaviour change, having received unprecedented research attention, yet it has simultaneously attracted exceptional criticism”, and said “that there is still value in the transtheoretical model but that the way in which it is researched needs urgently to be addressed”. Depending on the field of application (e.g. smoking cessation, substance abuse, condom use, diabetes treatment, obesity and travel) somewhat different criticisms have been raised.
In a systematic review, published in 2003, of 23 randomized controlled trials, the authors found that “stage based interventions are no more effective than non-stage based interventions or no intervention in changing smoking behaviour”. However, it was also mentioned that stage based interventions are often used and implemented inadequately in practice. Thus, criticism is directed towards the use rather the effectiveness of the model itself. Looking at interventions targeting smoking cessation in pregnancy found that stage-matched interventions were more effective than non-matched interventions. One reason for this was the greater intensity of stage-matched interventions. Also, the use of stage-based interventions for smoking cessation in mental illness proved to be effective. Further studies, e.g. a randomised controlled trial published in 2009, found no evidence that a TTM based smoking cessation intervention was more effective than a control intervention not tailored to stage of change. The study claims that those not wanting to change (i.e. precontemplators) tend to be responsive to neither stage nor non-stage based interventions. Since stage-based interventions tend to be more intensive they appear to be most effective at targeting contemplators and above rather than pre-contemplators. A 2010 systematic review of smoking cessation studies under the auspices of the Cochrane Collaboration found that “stage-based self-help interventions (expert systems and/or tailored materials) and individual counselling were neither more nor less effective than their non-stage-based equivalents”. A 2014 Cochrane systematic review concluded that research on the use of TTM stages of change “in weight loss interventions is limited by risk of bias and imprecision, not allowing firm conclusions to be drawn”.
Main criticism is raised regarding the “arbitrary dividing lines” that are drawn between the stages. West claimed that a more coherent and distinguishable definition for the stages is needed. Especially the fact that the stages are bound to a specific time interval is perceived to be misleading. Additionally, the effectiveness of stage-based interventions differs depending on the behaviour. A continuous version of the model has been proposed, where each process is first increasingly used, and then decreases in importance, as smokers make progress along some latent dimension. This proposal suggests the use of processes without reference to stages of change.
West claimed that the model “assumes that individuals typically make coherent and stable plans”, when in fact they often do not. However, the model does not require that all people make a plan: for example, the SAMSHA document Enhancing Motivation for Change in Substance Use Disorder Treatment, which uses the TTM, also says: “Don’t assume that all clients need a structured method to develop a change plan. Many people can make significant lifestyle changes and initiate recovery from SUDs without formal assistance”.
Within research on prevention of pregnancy and sexually transmitted diseases, a systematic review from 2003 comes to the conclusion that “no strong conclusions” can be drawn about the effectiveness of interventions based on the transtheoretical model. Again this conclusion is reached due to the inconsistency of use and implementation of the model. This study also confirms that the better stage-matched the intervention the more effect it has to encourage condom use.
Within the health research domain, a 2005 systematic review of 37 randomized controlled trials claims that “there was limited evidence for the effectiveness of stage-based interventions as a basis for behaviour change. Studies with which focused on increasing physical activity levels through active commute however showed that stage-matched interventions tended to have slightly more effect than non-stage matched interventions. Since many studies do not use all constructs of the TTM, additional research suggested that the effectiveness of interventions increases the better it is tailored on all core constructs of the TTM in addition to stage of change. In diabetes research the “existing data are insufficient for drawing conclusions on the benefits of the transtheoretical model” as related to dietary interventions. Again, studies with slightly different design, e.g. using different processes, proved to be effective in predicting the stage transition of intention to exercise in relation to treating patients with diabetes.
TTM has generally found a greater popularity regarding research on physical activity, due to the increasing problems associated with unhealthy diets and sedentary living, e.g. obesity, cardiovascular problems. A 2011 Cochrane Systematic Review found that there is little evidence to suggest that using the transtheoretical model stages of change (TTM SOC) method is effective in helping obese and overweight people lose weight. There were only five studies in the review, two of which were later dropped due to not being relevant since they did not measure weight. Earlier in a 2009 paper, the TTM was considered to be useful in promoting physical activity. In this study, the algorithms and questionnaires that researchers used to assign people to stages of change lacked standardisation to be compared empirically, or validated.
Similar criticism regarding the standardisation as well as consistency in the use of TTM is also raised in a 2017 review on travel interventions. With regard to travel interventions only stages of change and sometimes decisional balance constructs are included. The processes used to build the intervention are rarely stage-matched and short cuts are taken by classifying participants in a pre-action stage, which summarises the precontemplation, contemplation and preparation stage, and an action/maintenance stage. More generally, TTM has been criticised within various domains due to the limitations in the research designs. For example, many studies supporting the model have been cross-sectional, but longitudinal study data would allow for stronger causal inferences. Another point of criticism is raised in a 2002 review, where the model’s stages were characterised as “not mutually exclusive”. Furthermore, there was “scant evidence of sequential movement through discrete stages”. While research suggests that movement through the stages of change is not always linear, a study of smoking cessation conducted in 1996 demonstrated that the probability of forward stage movement is greater than the probability of backward stage movement. Due to the variations in use, implementation and type of research designs, data confirming TTM are ambiguous. More care has to be taken in using a sufficient amount of constructs, trustworthy measures, and longitudinal data.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Transtheoretical_model >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
The American Psychiatric Association (APA) is the main professional organisation of psychiatrists and trainee psychiatrists in the United States, and the largest psychiatric organiaation in the world. It has more than 38,000 members who are involved in psychiatric practice, research, and academia representing a diverse population of patients in more than 100 countries. The association publishes various journals and pamphlets, as well as the Diagnostic and Statistical Manual of Mental Disorders (DSM). The DSM codifies psychiatric conditions and is used mostly in the United States as a guide for diagnosing mental disorders.
The organisation has its headquarters in Washington, D.C.
Brief History
At a meeting in 1844 in Philadelphia, thirteen superintendents and organisers of insane asylums and hospitals formed the Association of Medical Superintendents of American Institutions for the Insane (AMSAII). The group included Thomas Kirkbride, creator of the asylum model which was used throughout the United States. The group was chartered to focus “primarily on the administration of hospitals and how that affected the care of patients”, as opposed to conducting research or promoting the profession.
In 1893, the organisation changed its name to the American Medico-Psychological Association. In 1921, the association changed that name to the present American Psychiatric Association. The association was incorporated in 1927.
The cover of the publication Semi-Centennial Proceedings of the American Medical Psychological Association, which the association distributed in 1894 at its 50th annual meeting in Philadelphia, contained the first depiction of the association’s official seal. The seal has undergone several changes since that time.
The present seal is a round medallion with a purported likeness of Benjamin Rush’s profile and 13 stars over his head to represent the 13 founders of the organisation. The outer ring contains the words “American Psychiatric Association 1844.” Rush’s name and an MD are below the picture.
An association history of the seal states:
The choice of Rush (1746–1813) for the seal reflects his place in history. …. Rush’s practice of psychiatry was based on bleeding, purging, and the use of the tranquilizer chair and gyrator. By 1844 these practices were considered erroneous and abandoned. Rush, however, was the first American to study mental disorder in a systematic manner, and he is considered the father of American Psychiatry.
In 2015, the association adopted a new logo that depicts the serpent-entwined Rod of Asclepius superimposed over the image of two hemispheres of a human brain. The logo appears next to the words “American Psychiatric Association”, with the word “Psychiatric” in bold type; the tagline “Medical leadership for mind, brain and body” appears below the logo. The association will continue to use the seal bearing Rush’s profile for ceremonial purposes and for some internal documents.
Organisation and Membership
APA is led by the President of the American Psychiatric Association and a board of trustees with an executive committee.
APA reports that its membership is primarily medical specialists who are qualified, or in the process of becoming qualified, as psychiatrists. The basic eligibility requirement is completion of a residency programme in psychiatry accredited by the Residency Review Committee for Psychiatry of the Accreditation Council for Graduate Medical Education (ACGME), the Royal College of Physicians and Surgeons of Canada (RCPS[C]), or the American Osteopathic Association (AOA). Applicants for membership must also hold a valid medical license (with the exception of medical students and residents) and provide one reference who is an APA member.
APA holds an annual conference attended by an American and international audience.
APA is made up of some 76 district associations throughout the country.
Foundation
APA operates a non-profit subsidiary called the American Psychiatric Association Foundation (APAF), offering community-based programs and research initiatives intended to better understand and support issues of mental health. Its strategic partners include the Council of State Governments (CSG) Justice Centre, Substance Abuse and Mental Health Services Administration (SAMHSA) and the National Association of Counties (NACo).
Corporate Alliance
APAF partners with industry organisations to collaborate on mental health research and development through its Corporate Alliance. Current and recent members of the alliance include:
AbbVie
Acadia Pharmaceuticals
Alkermes
Allergan
Bausch Health
Boehringer Ingelheim
Eisai
Indivior
Janssen Pharmaceuticals
Jazz Pharmaceuticals
Lundbeck
Myriad Genetics
Neurocrine Biosciences
Otsuka Pharmaceutical
Pfizer
Sunovion
Takeda Pharmaceutical Company
Donors to the foundation in 2019 include the Austen Riggs Centre, BB&T, Cenveo, McLean Hospital, Menninger Foundation, NeuroStar, Newport Academy, NewYork-Presbyterian Hospital, Sheppard Pratt, and Silver Hill Hospital.
Publications and Campaigns
APA position statements, clinical practice guidelines, and descriptions of its core diagnostic manual (the DSM) are published.
APA publishes several journals focused on different areas of psychiatry, for example, academic, clinical practice, or news.
Top Five Choosing Wisely Recommendations
In coordination with the American Board of Internal Medicine, the APA proposes five recommendations for physicians and patients. The list was compiled by members of the Council on Research and Quality Care. The APA places a primary focus on antipsychotic medications due to a rapid increase in sales, from $9.6 billion in 2004 to $18.5 billion in 2011.
Do not prescribe antipsychotic medications to patients for any indication without appropriate initial evaluation and appropriate ongoing monitoring.
Do not routinely prescribe 2 or more antipsychotic medications concurrently.
Do not prescribe antipsychotic medications as a first-line intervention to treat behavioural and psychological symptoms of dementia.
Do not routinely prescribe antipsychotic medications as a first-line intervention for insomnia in adults.
Do not routinely prescribe antipsychotic medications as a first-line intervention for children or adolescents for any diagnosis other than psychotic disorders.
Notable Figures
Donald Cameron, was president of the American Psychiatric Association in 1952-1953. He conducted coercive experiments widely denounced as unethical, including involuntary electroshock therapy, drug administration, and prolonged confinement and sensory deprivation funded as part of the Central Intelligence Agency Project MKUltra.
Enoch Callaway, psychiatrist, pioneer in biological psychiatry.
Adolf Meyer, former psychiatrist-in-chief at the Johns Hopkins Hospital, was the president of the American Psychiatric Association from 1927 to 1928 and was one of the most influential figures in psychiatry in the first half of the twentieth century.
Mark Ragins: American psychiatrist in the recovery movement, founding member of the Village ISA. He won the 1995 van Ameringen Award for his outstanding contribution to the field of psychiatric rehabilitation and was named a Distinguished Fellow of the American Psychiatric Association in 2006.
Herb Pardes past president and noted figure in American psychiatry.
Robert Spitzer was the chair of the task force of the third edition of the DSM.
Drug Company Ties
In his book Anatomy of an Epidemic (2010), Robert Whitaker described the partnership that has developed between the APA and pharmaceutical companies since the 1980s. APA has come to depend on pharmaceutical money. The drug companies endowed continuing education and psychiatric “grand rounds” at hospitals. They funded a political action committee in 1982 to lobby Congress. The industry helped to pay for the APA’s media training workshops. It was able to turn psychiatrists at top schools into speakers, and although the doctors felt they were independents, they rehearsed their speeches and likely would not be invited back if they discussed drug side effects. “Thought leaders” became the experts quoted in the media. As Marcia Angell wrote in The New England Journal of Medicine (2000), “thought leaders” could agree to be listed as an author of ghostwritten articles, and she cites Thomas Bodenheimer and David Rothman who describe the extent of the drug industry’s involvement with doctors. The New York Times published a summary about antipsychotic medications in October 2010.
In 2008, for the first time, Senator Charles Grassley asked the APA to disclose how much of its annual budget came from drug industry funds. The APA said that industry contributed 28 percent of its budget ($14 million at that time), mainly through paid advertising in APA journals and funds for continuing medical education.
The APA receives additional funding from the pharmaceutical industry through its American Psychiatric Association Foundation (APAF), including Boehringer Ingelheim, Janssen Pharmaceuticals, and Takeda Pharmaceutical Company, among others.
Controversies
In the 1964 election, Fact magazine polled American Psychiatric Association members on whether Barry Goldwater was fit to be president and published “The Unconscious of a Conservative: A Special Issue on the Mind of Barry Goldwater”. This led to a ban on the diagnosis of a public figure by psychiatrists who have not performed an examination or been authorised to release information by the patient. This became the Goldwater rule.
Supported by various funding sources, the APA and its members have played major roles in examining points of contention in the field and addressing uncertainties about psychiatric illness and its treatment, as well as the relationship of individual mental health concerns to those of the community. Controversies have related to anti-psychiatry and disability rights campaigners, who regularly protest at American Psychiatric Association offices or meetings. In 1970, members of the Gay Liberation Front organisation protested the APA conference in San Francisco. In 2003 activists from MindFreedom International staged a 21-day hunger strike, protesting at a perceived unjustified biomedical focus and challenging APA to provide evidence of the widespread claim that mental disorders are due to chemical imbalances in the brain. APA published a position statement in response and the two organisations exchanged views on the evidence.
The APA’s DSM came under criticism from autism specialists Tony Attwood and Simon Baron-Cohen for proposing the elimination of Asperger’s syndrome as a disorder and replacing it with an autism spectrum severity scale. Roy Richard Grinker wrote a controversial editorial for The New York Times expressing support for the proposal.
The APA president in 2005, Steven Sharfstein, praised the pharmaceutical industry but argued that American psychiatry had “allowed the biopsychosocial model to become the bio-bio-bio model” and accepted “kickbacks and bribes” from pharmaceutical companies leading to the over-use of medication and neglect of other approaches.
In 2008 APA was the focus of congressional investigations on how pharmaceutical industry money shapes the practices of non-profit organisations that purport to be independent. The drug industry accounted in 2006 for about 30 percent of the association’s $62.5 million in financing, half through drug advertisements in its journals and meeting exhibits, and the other half sponsoring fellowships, conferences and industry symposiums at its annual meeting. The APA came under increasing scrutiny and questions about conflicts of interest.
The APA president in 2009–10, Alan Schatzberg, was identified as the principal investigator on a federal study into the drug mifepristone for use as an antidepressant being developed by Corcept Therapeutics, a company Schatzberg had created and in which he had several million dollars’ equity.
In 2021, the APA issued an apology for its historical role in perpetuating racism.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/American_Psychiatric_Association >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Services for mental health disorders provide treatment, support, or advocacy to people who have psychiatric illnesses. These may include medical, behavioural, social, and legal services.
Medical services are usually provided by mental health experts like psychiatrists, psychologists, and behavioural health counsellors in a hospital or outpatient clinic. Behavioural services go hand-in-hand with medical services, referring specifically to pharmacological and cognitive therapy. Social services are usually provided by the government or non-profit organisations. They arrange housing options, job training, or other community resources overseen by experienced professionals to ensure overall productivity and well-being of individuals with mental illnesses. Legal services ensure that people with mental health disorders are not discriminated against in society and advocate for their basic human rights. In addition, legal services make sure that those individuals who might be a danger to themselves or others are diverted away from the judicial system to receive adequate treatment for underlying mental health issues.
The information provided below is primarily regarding services offered within the US, unless otherwise specified.
Medical Services
There are several types of medical service settings that can serve to deliver mental health care or services. These include, but are not limited to family practice, psychiatric hospitals or clinics, general hospitals, and community mental or behavioural health centres. One medical service that is not used as much is the self-help plan. The self-help plan is where a person with mental illness addresses their condition then find strategies to get better. This may include addressing any triggers, recovery options or warning signs. Different services endorse different payment models. Some may be more government-based or patient-based, while others may endorse mixed-models payment systems. Not all service types or institutions are accessible by all patients. A considerable barrier surrounds the difficulty in finding in-network mental health care providers, given the backdrop of our current and critical nationwide shortage of mental health professionals.
Family practice or general practice centres in communities are often the first line for assessment of mental health conditions. The basic services provided may include prescribing psychiatric drugs and sometimes providing basic counselling or therapy for “common mental disorders.” Secondary medical services may include psychiatric hospitals, or clinics. However, given the trend towards the deinstitutionalisation of mental health hospitals – the movement of mental health patients out of the “asylum-based” mental health care system towards community-oriented care – psychiatric hospitals have been going out of favour, with services being directed to wards within general hospitals as well as more locally based community mental health services.
Mental health services may be provided either on an inpatient or, more commonly, an outpatient basis. A wide range of treatments may be provided to patients, with a mainstay of treatment being centred on psychiatric drugs. However, medication does not cure any mental illness but it does help manage symptoms. Various mental health professionals may be involved including psychiatrists, psychiatric and mental health nurses and, less commonly, non-medical professionals such as clinical psychologists, social workers, and various kinds of therapists or counsellors. Usually headed by psychiatrists and therefore based on a medical model, multidisciplinary teams may be involved in assertive community treatment and early intervention and may be coordinated via a case management system (sometimes referred to as “service coordination”).
Behavioural Therapy Services
Numerous services exist exclusively for the therapy of mental disorders and distress. Since symptoms vary across individuals, therapy is usually individualised for patients. All behaviours can be learned and also can be changed. Behavioural therapy is a method of therapy that is used to help identify unhealthy behaviours and to help change such behaviours. Methods exist that target numerous areas at once, such as integrative psychotherapy (an eclectic tailored mix of approaches). Integrative psychotherapists consider many factors when treating a patient, such as preferences, physical capabilities, or family support. In contrast to integrative psychotherapy, many approaches focus on particular areas. Cognitive behavioural therapy, psychodynamic therapy, interpersonal therapy, and dialectical behavioural therapy are all examples of approaches that have primary focuses when attempting to treat a patient. Conditions that can be treated by these therapies include anxiety, eating disorders, substance use disorders, obsessive compulsive disorders, and insomnia. The chosen therapy depends on several factors, with patient preference being a significant one.
Each type of therapy has its own strengths and weaknesses. Cognitive behavioural therapy is an attempt to allow patients to realise any inaccurate thoughts they may have and to allow them to perceive situations differently. Roughly about 75% of people who have used the cognitive behaviour therapy have experience a great outcome, which shows how effective this type of therapy is. There is also another type of cognitive therapy which is called cognitive behavioural play therapy. This therapy is particularly used for children. It is done by the therapist watching the child play then determining what the child is uncomfortable expressing. Psychodynamic therapy differs from cognitive behavioural therapy in that it is a longer-term therapy that usually requires more sessions for its effectiveness. Psychodynamic therapy is less structured and relies heavily on the relationship between the therapist and the patient. Although cognitive behavioural therapy has become the more favoured form of therapy, psychodynamic therapy continues to be viewed as the more effective treatment. When medication and psychodynamic are being used together it gives a higher chance of recovery. An integrative approach would allow one therapist to implement both cognitive behavioural therapy and psychodynamic therapy while treating the same patient. Interpersonal therapy is highly structured and is usually targeted at depression. There is evidence that suggests interpersonal therapy provides a benefit that is equal to pharmacologic therapy for depression. Dialectical behavioural therapy is an evidence-based psychotherapy that is usually used to treat suicidal behaviours. Each form of behavioural therapy uses different strategies to reach the goal of improving the quality of life for patients.
Social Services
Community-based social services often include supportive housing, clubhouses, and national hotlines. These resources may be provided by people who are successfully living with psychiatric disorders. Peer-led support encourage those individuals struggling with mental health disorders to seek self-help strategies and belong to social support network.
Supportive Housing
Supportive housing is an innovative solution that aims to provide permanent, accessible, and affordable housing options for individuals with mental health disorders. Additional help is often available to manage one’s finances, daily activities, and healthcare needs. Rent is usually less than 30% of one’s income and is further made affordable through rental assistance programmes offered by the government. It, also, provides access to public transportation as well as healthcare providers and other community resources. In supervised or partially-supervised supportive housing, trained staff may be present to help with medication management, paying bills, cleaning, cooking, and other day-to-day tasks. These environments are usually group home settings, where individuals have their own bedroom and bathroom but share common areas with other residents. Alternatively, individuals may also choose to live in independent supportive housing if they do not require frequent supervision regarding their activities of daily living. It is important to note that tenants have the freedom to choose which services they would like to utilise based on their degree of independence and unmet needs.
One of the limitations that prevent the widespread availability of supportive housing is the cost associated with hiring trained staff and maintaining the building as well as surrounding premises, while still keeping the rent affordable. However, studies have shown that the integrated services offered by supportive housing helps to decrease homelessness, incarceration rates, emergency room visits, and the number of days patients stay in a hospital. Such widespread effects can promote the lowering of costs associated with services in the above-mentioned areas and these funds can be diverted to sustain supportive housing projects.
Clubhouse Model
Clubhouses are community centres that are usually run by individuals who have a current or previous history of mental illness. The main purpose of these establishments is to promote rehabilitation and self-sufficiency of individuals by offering them employment opportunities. This includes access to community workshops, job training programmes, and educational opportunities. Additionally, clubhouse staff may maintain partnerships with local employers to provide full-time or part-time employment opportunities. Members, also, have access to social events and team-based activities, which helps them to develop a social support network.
Phone-Based Services
A mental health hotline is a free, confidential, and convenient way to receive information regarding various mental health services that are available in the community. The hotline is operated by trained employees and volunteers who can connect callers with the appropriate medical, legal, or social resources. There are no restrictions regarding how many times an individual may utilise a particular hotline. Some services may be available 24 hours a day, 7 days a week and via text messaging applications.
A few phone-based services exclusively deal with mental health emergencies or crisis situations, such as suicide and substance abuse. Suicide prevention lifelines are operated by mental health counsellors or community volunteers. They are trained to identify suicide risk, de-escalate an emergent crisis, and provide emotional support for those in distress. Substance abuse and relapse helplines provide behavioural support to those struggling with addiction as well as connect them with rehabilitation centres for treatment.
Phone-based services also allow for providers to remove language barriers. This is due to the fact that there are several online translation services in order to record and relay information in real time, across several different languages. By eliminating language barriers, providers are also able to prevent patients from experiencing social prejudice. Patients can now reach out to a wider variety of providers and are no longer bound to their local community practitioners, where there could be added stigma.
Telehealth Services
The use of Telehealth, health related services distributed electronically, has exploded in popularity across the world of medicine following the 2019-2020 COVID-19 pandemic. Remote health services have opened up a new dimension for healthcare providers to provide care to patients with efficiency and a wider range of accessibility. The inclusion of mental health services in this expansion has helped dispel the belief that mental health is not capable of being done electronically and has opened up new possibilities in the field of mental health services, and service provision. There are still limits restricting Telehealth including the fact that many people still do not have access to technology such as phones and computers, and that it cannot replace more intensive treatment settings.
Apps Providing Psychological Services
Mental health apps are an increasingly popular means of providing mental health services. They are cost effective, easy to access at almost any location, affordable, anonymous, can provide around the clock support, can reach a greater number of people, and are capable of providing a supporting role to other services for mental disorders. Even though apps have great potential to accomplish new and innovative goals in the field of mental health, they do still have some limitations. Not everyone has access to technology through which the apps can be run, there are elements of data collection which may make some users uncomfortable, there is not much regulation of these mental health services, and the apps may turn people away from using harder to access but more provenly effective services that they could benefit from.
Legal Services
Legal services supervise the involuntary commitment or outpatient commitment of those judged to have mental disorders and to be a danger to themselves or others. Some legal organisations provide specialised services for those diagnosed with mental disorders who may be challenging discrimination or involuntary commitment.
Mental health courts are specialised court dockets that provide community treatment and supervision in lieu of incarceration for criminal offenders with mental illness. A judge assesses the defendant’s background as well as the influence of his or her mental disorder on the committed crime. A team of mental health professionals and legal advisors ensures that a particular mental health treatment programme provides appropriate opportunities for rehabilitation and prevent future criminal behaviour. The defendant is given the choice to decide if they want to participate in the treatment, unless they are unable to provide informed consent. In such cases, a conservator could make treatment decisions on behalf of the defendant and may give permission to use medications, if appropriate. Successful completion of the programme may result in reduced sentences or all charges against the defendant to be dropped.
Global Situation
Statistics
In 2017, more than 970 million or 1-in-7 individuals were purported to have one or more mental or substance use disorder(s). Anxiety and depressive disorders were, by far, the most attributed. Moreover, around 5%, and up to 12%, of global disease burden was attributable to mental or substance use disorders. Countries that have the greatest disease burden from mental or substance use disorders include Kuwait, Qatar, Australia, among others.
A Global Mental Health Group in coordination with the World Health Organisation has called for an urgent scaling up of the funding, staffing and coverage of services for mental disorders in all countries, especially in low-income and middle-income countries.
According to the Recovery model, services must always support an individual’s personal journey of recovery and independence, and a person may or may not need services at any particular time, or at all. The UK is moving towards paying mental health providers by the outcome results that their services achieve.
Traditional and Alternative Services
Traditional healing centres are popular worldwide and provide accessible mental health services for the native population. This community-based practice is led by folk healers, who use herbal remedies, spiritual rituals, and indigenous perspectives to provide comfort for individuals. These services are highly culture-specific and, therefore, its structure varies across the globe. Traditional healing approaches are sometimes used alongside conventional or western medicine.
In addition, each country has its own view on mental health disorders. While many nations share advocacy for mental health, there are still several countries that stigmatize medical or behavioural treatment for these disease states. Examples of these are Canada and China, such that both have high mental health illness rates but low utilisation rates of mental health services. While the cause of this is unknown, it is believed to be due to general stigma in those communities towards seeking help for mental health.
Problems with Mental Health Services
Expanding Increase in Demand
As awareness of mental health increases more and more people require mental health services. According to studies in 2023 over half of adults (54.7%) suffering from a mental illness are not receiving treatment, and almost a 3rd (28.2%) of adults with mental illness cannot get the treatment they need. There is increasing demand for new paths to provide mental services such as telehealth to make the distribution of services more streamlined along with need for more service providers to account for growing demand for treatment.
Struggle to Provide Services for Underserved Communities
Service providers for mental health have long struggled to provide adequate care for underserved communities such as minorities, the homeless, and incarcerated populations. These groups generally are in need of greater amounts of care in part due to the adversities that have both created and perpetuated their situations like systemic racism, troubled backgrounds, access to housing, and poverty. There are barriers to access for mental health services that continue to make them inaccessible such as high cost, language barriers, and access to providers in many communities.
Systemic Barriers
Many governments across the globe continue to neglect the importance of mental health services. The United States for example continues to not provide healthcare accommodation for mental health services and struggles to fulfil policies like The Mental Health and Addiction Parity Act of 2008 that are intended to make mental health services more accessible. Many governments continue to fail to recognise mental health services as important facets of healthcare and properly provide for them. Many countries still consider mental health a problem of which only high earning countries face and fail to recognize mental health as a developing struggle that affects people of all backgrounds.
Push Toward Change
There is an increasing push for new innovative ways to provide mental health services. Telehealth has been a massively eye opening success following its widespread usage during the 2019-2020 COVID-19 Pandemic and has changed the belief that mental health services cannot be useful when provided electronically. Suggestions such as governmental change and the creation of workers who bring mental health services to hard to reach communities and individuals have been theorised to be possible solutions. Apps for psychological services are also looked at as a promising new development that could greatly expand people’s access to psychological services in the future due to their numerous benefits such as convenience, anonymity, and outreach.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Services_for_mental_disorders >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
The Alaska Mental Health Enabling Act of 1956 (Public Law 84-830) was an Act of Congress passed to improve mental health care in the United States territory of Alaska. It became the focus of a major political controversy after opponents nicknamed it the “Siberia Bill” and denounced it as being part of a communist plot to hospitalise and brainwash Americans. Campaigners asserted that it was part of an international Jewish, Roman Catholic or psychiatric conspiracy intended to establish United Nations-run concentration camps in the United States.
The legislation in its original form was sponsored by the Democratic Party, but after it ran into opposition, it was rescued by the conservative Republican Senator Barry Goldwater. Under Goldwater’s sponsorship, a version of the legislation without the commitment provisions that were the target of intense opposition from a variety of far-right, anti-Communist and fringe religious groups was passed by the United States Senate. The controversy still plays a prominent role in the Church of Scientology‘s account of its campaign against psychiatry.
The Act succeeded in its initial aim of establishing a mental health care system for Alaska, funded by income from lands allocated to a mental health trust. However, during the 1970s and early 1980s, Alaskan politicians systematically stripped the trust of its lands, transferring the most valuable land to private individuals and state agencies. The asset stripping was eventually ruled to be illegal following several years of litigation, and a reconstituted mental health trust was established in the mid-1980s.
Background
Alaska possessed no mental health treatment facilities prior to the passage of the 1956 Act. At the time of the Act’s passage, Alaska was not a US state, being constituted instead as a territory of the United States. The treatment of the mentally ill was governed by an agreement with the state of Oregon dating back to the turn of the 20th century. On June 6, 1900, the United States Congress enacted a law permitting the government of the then District of Alaska to provide mental health care for Alaskans. In 1904, a contract was signed with Morningside Hospital, privately owned and operated by Henry Waldo Coe in Portland, Oregon, under which Alaskan mental patients would be sent to the hospital for treatment. A commitment regime was established under which a person said to be mentally ill was to be brought before a jury of six people for a ruling on insanity. The patient was routinely sent to prison until his release or transfer to Portland; at no point in this ruling was a medical or psychiatric examination required.
By the 1940s, it was recognised that this arrangement was unsatisfactory. The American Medical Association conducted a series of studies in 1948, followed by a Department of the Interior study in 1950. They highlighted the deficiencies of the program: commitment procedures in Alaska were archaic, and the long trip to Portland had a negative effect on patients and their families. In addition, an audit of the hospital contract found that the Sanatorium Company, which owned the hospital, had been padding its expenses. This had enabled it to make an excess profit of $69,000 per year (equivalent to over $588,000 per year at 2007 prices).
The studies recommended a comprehensive overhaul of the system, with the development of an in-territory mental health programme for Alaska. This proposal was widely supported by the public and politicians. At the start of 1956, in the second session of the 84th Congress, Representative Edith Green (D-Oregon) introduced the Alaska Mental Health Bill (H.R. 6376) in the House of Representatives. The bill had been written by Bob Bartlett, the Congressional Delegate from the Alaska Territory who later became a US Senator. Senator Richard L. Neuberger (D-Oregon) sponsored an equivalent bill, S. 2518, in the Senate.
Details of the Bill
The Alaska Mental Health Bill’s stated purpose was to “transfer from the Federal Government to the Territory of Alaska basic responsibility for the hospitalisation, care and treatment of the mentally ill of Alaska.” In connection with this goal, it aimed:
To modernise procedures for such hospitalisation (including commitment), care, and treatment and to authorise the Territory to modify or supersede such procedures;
To assist in providing for the Territory necessary facilities for a comprehensive mental-health programme in Alaska, including inpatient and outpatient facilities;
To provide for a land grant to the Territory to assist in placing the programme on a firm long-term basis; and
To provide for a ten-year programme, of grants-in-aid to the Territory to enable the Territory gradually to assume the full operating costs of the programme.
The bill provided for a cash grant of $12.5 million (about $94 million at 2007 prices) to be disbursed to the Alaskan government in a number of phases, to fund the construction of mental health facilities in the territory. To meet the ongoing costs of the programme, the bill transferred one million acres (4,000 km2) of federally owned land in Alaska to the ownership of the proposed new Alaska Mental Health Trust as a grant-in-aid—the federal government owned about 99% of the land of Alaska at the time. The trust would then be able to use the assets of the transferred land (principally mineral and forestry rights) to obtain an ongoing revenue stream to fund the Alaskan mental health programme. Similar provisions had applied in other US territories to support the provision of public facilities prior to the achievement of statehood.
In addition, the bill granted the Governor of Alaska authority to enter into reciprocal mental health treatment agreements with the governors of other states. Alaskans who became mentally ill in the lower 48 states would be properly treated locally until they could be returned to Alaska; likewise, citizens of the lower 48 who fell mentally ill in Alaska would receive care there, before being returned to their home states.
The bill was seen as entirely innocuous when it was introduced on 16 January 1956. It enjoyed bipartisan support, and on January 18 it was passed unanimously by the House of Representatives. It then fell to the Senate to consider the equivalent bill in the upper chamber, S. 2518, which was expected to have an equally untroubled passage following hearings scheduled to begin on 20 February.
Controversy
Initial Opposition
In December 1955, a small anti-communist women’s group in Southern California, the American Public Relations Forum (APRF), issued an urgent call to arms in its monthly bulletin. It highlighted the proposed text of the Alaska Mental Health Bill, calling it “one that tops all of them”. The bulletin writers commented: “We could not help remembering that Siberia is very near Alaska and since it is obvious no one needs such a large land grant, we were wondering if it could be an American Siberia.” They said that the bill “takes away all of the rights of the American citizen to ask for a jury trial and protect him[self] from being railroaded to an asylum by a greedy relative or ‘friend’ or, as the Alaska bill states, ‘an interested party’.”
The APRF had a history of opposing mental health legislation; earlier in 1955, it had played a key role in stalling the passage of three mental health bills in the California Assembly. It was part of a wider network of far-right organizations which opposed psychiatry and psychology as being pro-communist, anti-American, anti-Christian and pro-Jewish. The Keep America Committee, another Californian “superpatriot” group, summed up the anti-mental-health mood on the far right in a pamphlet issued in May 1955. Calling “mental hygiene” part of the “unholy three” of the “Communistic World Government”, it declared: “Mental Hygiene is a subtle and diabolical plan of the enemy to transform a free and intelligent people into a cringing horde of zombies”.
The APRF’s membership overlapped with that of the much larger Minute Women of the U.S.A., a nationwide organisation of militant anti-communist housewives which claimed up to 50,000 members across the United States. In mid-January 1956, Minute Woman Leigh F. Burkeland of Van Nuys, California issued a bulletin protesting against the bill. It was mimeographed by the California State Chapter of the Minute Women and mailed across the nation. On 24 January 1956, the strongly anti-statist Santa Ana Register newspaper reprinted Burkeland’s statement under the headline, “Now — Siberia, U.S.A.” Burkeland issued a lurid warning of what the future might hold if the Alaska Mental Health Bill was passed by the Senate:
Is it the purpose of H.R. 6376 to establish a concentration camp for political prisoners under the guise of treatment of mental cases? The answer, based on a study of the bill, indicates that it is entirely within the realm of possibility that we may be establishing in Alaska our own version of the Siberia slave camps run by the Russian government. … This legislation, say its opponents, will place every resident of the United States at the mercy of the whims and fancies of any person with whom they might have a disagreement, causing a charge of ‘mental illness’ to be placed against them, with immediate deportation to SIBERIA, U.S.A!
Further Opposition
After the Santa Ana Register published its article, a nationwide network of activists began a vociferous campaign to torpedo the Alaska Mental Health Bill. The campaigners included, among other groups and individuals, the white supremacist Rev. Gerald L.K. Smith; Women for God and Country; the For America League; the Minute Women of the U.S.A.; the right-wing agitator Dan Smoot; the anti-Catholic former US Army Brigadier General Herbert C. Holdridge; and L. Ron Hubbard’s Church of Scientology, which had been founded only two years earlier.
Increasingly strong statements were made by the bill’s opponents through the course of the spring and summer of 1956. In his 17 February bulletin, Dan Smoot told his subscribers: “I do not doubt that the Alaska Mental Health Act was written by sincere, well-intentioned men. Nonetheless, it fits into a sinister pattern which has been forming ever since the United Nations was organized.” Dr. George A. Snyder of Hollywood sent a letter to all members of Congress in which he demanded an investigation of the Alaska Mental Health Bill’s proponents for “elements of treason against the American people behind the front of the mental health program”. The Keep America Committee of Los Angeles similarly called the proponents of the bill a “conspiratorial gang” that ought to be “investigated, impeached, or at least removed from office” for treason. Retired brigadier general Herbert C. Holdridge sent a public letter to President Dwight Eisenhower on 12 March, in which he called the bill “a dastardly attempt to establish a concentration camp in the Alaskan wastes”. He went on:
This bill establishes a weapon of violence against our citizenry far more wicked than anything ever known in recorded history — far worse than the Siberian prison camps of the Czars or the Communists, or the violence of the Spanish Inquisition … The plot of wickedness revealed in this bill fairly reeks of the evil odor of the black forces of the Jesuits who dominate the Vatican, and, through officiates in our Government, dominate our politics.
For their part, America’s professional health associations (notably the American Medical Association and American Psychiatric Association) came out in favour of the bill. There was some initial opposition from the Association of American Physicians and Surgeons, a small and extremely conservative body which opposed socialized medicine; Dr. L. S. Sprague of Tucson, Arizona said in its March 1956 newsletter that the bill widened the definition of mental health to cover “everything from falling hair to ingrown toenails”. However, the association modified its position after it became clear that the AMA took the opposite view.
By March 1956, it was being said in Washington, D.C. that the amount of correspondence on the bill exceeded anything seen since the previous high-water mark of public controversy, the Lend-Lease Act of 1941. Numerous letter-writers protested to their Congressional representatives that the bill was “anti-religious” or that the land to be transferred to the Alaska Mental Health Trust would be fenced off and used as a concentration camp for the political enemies of various state governors. The well-known broadcaster Fulton Lewis described how he had “received, literally, hundreds of letters protesting bitterly against the bill. I have had telephone calls to the same effect from California, Texas and other parts of the country. Members of Congress report identical reactions.” A letter printed in the Daily Oklahoman newspaper in May 1956 summed up many of the arguments made by opponents of the bill:
The advocates of world government, who regard patriotism as the symptom of a diseased mind, took a step closer to their goal of compulsory asylum ‘cure’ for opponents of UNESCO, when, on January 18, the U.S. House of Representatives passed the Alaska Mental Health Act.
The Act was prepared by the U.S. Department of Justice, Department of the Interior and the socialist-oriented Department of Health, Education and Welfare. It closely follows the Model Code, drafted by the American Psychiatric association, which has been working with the World Health Organization, a specialized agency of the United Nations …
All of you who don’t want members of your family railroaded to an asylum had better start writing your senator, now.
During February and March 1956, hearings were held before the Senate Subcommittee on Territories and Insular Affairs. Proponents and opponents of the bill faced off in a series of tense exchanges, with strong accusations being made against the people and groups involved in the bill’s introduction. Stephanie Williams of the American Public Relations Forum said that the bill would enable Russia to reclaim its former Alaskan territory: “[It] contains nothing to prevent Russia from buying the entire million acres — they already say Alaska belongs to them.”
Mrs. Ernest W. Howard of the Women’s Patriotic Committee on National Defence castigated the slackness of Congress for not picking up on the bill’s perceived dangers: “Those of us who have been in the study and research work of the United Nations, we feel that we are experts in this … you as Senators with all the many commitments and the many requirements, are not able to go into all these things.” John Kaspar, a White Citizens’ Council organiser who had achieved notoriety for starting a race riot in Clinton, Tennessee, declared that “almost one hundred percent of all psychiatric therapy is Jewish and about eighty percent of psychiatrists are Jewish … one particular race is administering this particular thing.” He argued that Jews were nationalists of another country who were attempting to “usurp American nationality”.
Passing the Bill
The arguments of the bill’s opponents attracted little support in the Senate. The Eisenhower administration, the Alaska territorial government and mainstream religious groups were all in favour of the bill. The Alaska Presbyterian Church gave the bill its unanimous support, issuing a statement declaring: “As Christian citizens of Alaska we believe this is a progressive measure for the care and treatment of the mentally ill of Alaska. We deplore the present antiquated methods of handling our mentally ill.” It also urged the National Council of Churches to mobilise support for the bill. An overwhelming majority of senators of both parties were also supportive. The bill’s original author, Alaska Delegate Bob Bartlett, spoke for many of the bill’s proponents when he expressed his bafflement at the response that it had received:
I am completely at a loss in attempting to fathom the reasons why certain individuals and certain groups have now started a letter-writing campaign … to defeat the act. I am sure that if the letter writers would consult the facts, they would join with all others not only in hoping this act would become law but in working for its speedy passage and approval.
Other senators expressed similar mystification at the agitation against the bill. Senator Henry M. Jackson of Washington stated that he was “at a loss” to see how the bill affected religion, as its opponents said. Senator Alan Bible of Nevada, the acting chairman of the Subcommittee on Territories and Insular Affairs, told the bill’s opponents that nothing in the proposed legislation would permit the removal of any non-Alaskan to the territory for confinement.
Republican Senator Barry Goldwater of Arizona proposed an amended bill that removed the commitment procedures in Title I of the House bill and stated that “Nothing in this title shall be construed to authorize the transfer to Alaska, pursuant to any agreement or otherwise, of any mentally ill person who is not a resident of Alaska.” In effect, this eliminated the bill’s most controversial element—the provision for the transfer of mental patients from the lower 48 states to Alaska. The final recommendation of the Senate Committee on Interior and Insular Affairs followed Goldwater’s lead that the bill be amended to strike all the controversial “detailed provisions for commitment, hospitalization, and care of the mentally ill of Alaska” included in Title I of the original House bill. This amended proposal left only the transfer of responsibility for mental health care to the territory of Alaska and the establishment of land grants to support this care. The committee stressed that they were not invalidating the Title I provisions of the original bill but that they had been misunderstood, a recurrent theme in supporters of the bill:
However, the proposed provisions were misunderstood by many persons in parts of the country other than Alaska. Partly as a result of this misunderstanding, but more because the members of the committee are convinced that the people of Alaska are fully capable of drafting their own laws for a mental health program for Alaska, the committee concluded that authority should be vested in them in this field comparable to that of the States and other Territories.
Thus amended, the Senate bill (S. 2973) was passed unanimously by the Senate on 20 July after only ten minutes of debate.
Aftermath
Following the passage of the act, an Alaska Mental Health Trust was set up to administer the land and grants appropriated to fund the Alaskan mental health program. During the 1970s, the issue of the trust’s land became increasingly controversial, with the state coming under increasing pressure to develop the land for private and recreational use. In 1978, the Alaska Legislature passed a law to abolish the trust and transfer the most valuable parcels of lands to private individuals and the government. By 1982, 40,000 acres (160 km2) had been conveyed to municipalities, 50,000 acres (200 km2) transferred to individuals, and slightly over 350,000 acres (1,400 km2) designated as forests, parks or wildlife areas. Around 35% of the land trust remained unencumbered and in state ownership.
In 1982, Alaska resident Vern Weiss filed a lawsuit on behalf of his son, who required mental health services that were not available in Alaska. The case of Weiss v State of Alaska eventually became a class action lawsuit involving a range of mental health care groups. The Alaska Supreme Court ruled in 1985 that the abolition of the trust had been illegal and ordered it to be reconstituted. However, as much of the original land had been transferred away, the parties had to undergo a long and complex series of negotiations to resolve the situation. A final settlement was reached in 1994 in which the trust was reconstituted with 500,000 acres (2,000 km2) of original trust land, 500,000 acres (2,000 km2) of replacement land, and $200 million to replace lost income and assets.
Scientology and the Alaska Mental Health Bill
The Alaska Mental Health Bill plays a major part in the Church of Scientology’s account of its campaign against psychiatry. The Church participated in the campaign against the bill and still refers to it as the “Siberia Bill”. Scientology may also have provided an important piece of the “evidence” which the anti-bill campaigners used — a booklet titled Brain-Washing: A Synthesis of the Russian Textbook on Psychopolitics.
Miscavige on Nightline
Similarly, David Miscavige, the church’s leader, in 1992 told Ted Koppel in an interview on the Nightline programme:
I don’t know if you’re aware that there was a plan in 1955 in this country, Ted, to repeat what was done in Russia. There was going to be a Siberia, USA, set up on a million acres in Alaska to send mental patients. They were going to lessen the commitment laws, you could basically get into an argument with somebody and be sent up there. This sounds very odd. Nobody’s ever heard about it. That’s in no small part thanks to the Church of Scientology. I must say, though, that when that bill was killed in Congress, the war was on with psychiatry where they declared war on us … It was a major, major, major flap for the psychiatrists when it got voted down, because then the slogan around the country began, ‘Siberia, USA,’ and it was really the first time that psychiatry had been denigrated publicly, that they weren’t the science that they had been promoting themselves to be. And they took it upon themselves then to start dealing with anybody who would oppose them.
Conspiracy Theories
In Ron’s Journal 67, Hubbard identified “the people behind the Siberia Bill”, who he asserted were:
less than twelve men. They are members of the Bank of England and other higher financial circles. They own and control newspaper chains, and they are, oddly enough, directors in all the mental health groups in the world which have sprung up. Now these chaps are very interesting fellows: They have fantastically corrupt backgrounds; illegitimate children; government graft; a very unsavory lot. And they apparently, sometime in the rather distant past, had determined on a course of action. Being in control of most of the gold supplies of the planet, they entered upon a program of bringing every government to bankruptcy and under their thumb, so that no government would be able to act politically without their permission.
According to David Miscavige, the bill was the product of a conspiracy by the American Psychiatric Association. In a public address in 1995, he told Scientologists that it was “in 1955 that the agents for the American Psychiatric Association met on Capitol Hill to ram home the infamous Siberia Bill, calling for a secret concentration camp in the wastes of Alaska.” It was “here that Mr. Hubbard, as the leader of a new and dynamic religious movement, knocked that Siberia Bill right out of the ring — inflicting a blow they would never forget.” The assertion that Scientologists defeated the bill is made frequently in Scientology literature. In fact, the original version of the bill with the offending Title I commitment provisions only passed the House of Representatives; it was subsequently amended in conference to strike the commitment portion and retain the transfer of responsibility for mental health care. The revised bill passed easily without further changes.
Contemporary Publications
Contemporary Church publications suggest that although Hubbard was tracking progress of the bill at least as early as February 1956, Scientology did not become involved in the controversy until the start of March 1956, over two months after the American Public Relations Forum had first publicized the bill. A March “Professional Auditor’s Bulletin” issued by Hubbard, who was staying in Dublin at the time, includes a telegram from his Washington-based son L. Ron Hubbard, Jr. and two other Scientologists alerting him to the upcoming February Senate hearings:
HOUSE BILL 6376 PASSED JANUARY 18TH STOP GOES SENATE NEXT WEEK STOP BILL PERMITS ADMISSION OF PERSON TO MENTAL INSTITUTION BY WRITTEN APPLICATION OF INTERESTED PERSON BEFORE JUDICIAL PROCEEDINGS ARE HELD STOP DISPENSES WITH REQUIREMENT THAT PATIENT BE PRESENT AT HEARING STOP ANYONE CAN BE EXCLUDED FROM HEARING STOP BILL PERTAINS TO ALASKA AT MOMENT STOP BILL SETS UP ONE MILLION ACRES SIBERIAL [sic] IN ALASKA FOR INSTITUTIONS STOP LETTER AND BILL FOLLOW STOP WHAT ACTION YOU WANT TAKEN.
Although the church says that Scientologists led the opposition to the bill, the Congressional Record’s account of the Senate hearings into the bill does not mention the church. A contemporary review of the opposition to the bill likewise attributes the lead role elsewhere and to right-wing groups, rather than the “civil liberties” organisations cited by the church:
Only a few organized groups got behind the hue and cry. Most influential was the libertarian Association of Physicians and Surgeons, and Dan Smoot’s newsletter. Right-wing groups bombarded Congress with protests and demands for hearings.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Alaska_Mental_Health_Enabling_Act >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Since the founding of the Church of Scientology in 1954 by L. Ron Hubbard, the relationship between Scientology and psychiatry has been dominated by strong opposition by the organisation against the medical specialty of psychiatry and of psychology with themes relating to this opposition occurring repeatedly throughout Scientology literature and doctrine. According to the Church of Scientology, psychiatry has a long history of improper and abusive care. The group’s views have been disputed, criticised, and condemned by experts in the medical and scientific community and have been a source of public controversy.
L. Ron Hubbard had a complex and changing relationship with psychiatry. He recalled positive experiences with psychiatrists in his youth and requested psychiatric treatment in adulthood. By 1948, Hubbard claimed to volunteer in a psychiatric clinic and two years later published Dianetics: The Modern Science of Mental Health. In 1951, however, Hubbard’s wife Sara Northrup Hollister reportedly consulted psychiatrists who recommended Hubbard be institutionalised; thereafter, Hubbard was increasingly hostile towards psychiatry.
In 1995, Scientologist Lisa McPherson died at Church of Scientology Flag Service Organisation (FSO) at Flag Land Base after leaving a hospital where she refused psychiatric treatment.
In 2003, a man with untreated schizophrenia murdered his mother after his paranoid delusions caused him to become convinced that the Scientology-approved vitamins she was giving him in lieu of effective medication were poisonous.
In 2005, celebrity Scientologist Tom Cruise strongly asserted his public opposition to psychiatry.
L. Ron Hubbard and Psychiatry
L. Ron Hubbard was an American author of science fiction and fantasy stories. Hubbard reported many encounters with psychiatrists from the age of 12 onward.
During World War II, Hubbard was hospitalised; in 1947, Hubbard requested psychiatric treatment and the following year moved with his wife to Savannah, Georgia, where he was reportedly associated with a psychiatric clinic.
In 1950, Hubbard published Dianetics: The Modern Science of Mental Health.
In 1951, it was publicly reported that Hubbard’s wife Sara had been advised by a psychiatrist that Hubbard should be institutionalised for treatment of paranoid schizophrenia. They divorced, and the following year, Hubbard founded Scientology, an anti-psychiatry religious movement.
Hubbard’s beliefs and practices, drawn from a diverse set of sources, influenced numerous offshoots, splinter-groups, and new movements.
Overview
Hubbard’s views on psychiatry evolved over time.
Hubbard spoke positively of his childhood and teen encounters with psychiatrists in the 1920s and 30s. At the age of 12, Hubbard was accompanied by Navy psychiatrist Joseph Thompson on an ocean trip from Seattle to Washington, D.C. Hubbard likewise wrote positively of teenage/young-adult encounters with D.C.-based psychiatrist William Alanson White. Some of Hubbard’s later works included acknowledgements of both Thompson and White, and Hubbard would later claim to have received clinical training from both Thompson and White.
In contrast, Hubbard spoke more critically of his later encounters with psychiatrists and psychiatric institutions. Although Hubbard had written positively of psychiatric hospital superintendent William Alanson White, White’s successor (Winfred Overholser) was singled out for criticism. Hubbard likewise spoke critically of his encounters with a Washington, D.C., institution for the treatment of schizophrenia called “Walnut Lodge” (presumably Chestnut Lodge).
During the Second World War, Hubbard was hospitalised at Oak Knoll Military Hospital. In 1947, Hubbard wrote a letter to the VA requesting psychiatric treatment. The following year, Hubbard and his wife Sara moved to Savannah, Georgia, where Hubbard would later recall having been associated with a charity mental health clinic.
According to Hubbard, he worked as a volunteer helping to treat charity patients during his time in Savannah. While in Savannah, Hubbard began working on a “book of psychology” about “the cause and cure of nervous tension”; the next year, he published Dianetics: The Modern Science of Mental Health.
In 1951, Hubbard’s wife Sara reportedly consulted a psychiatrist who recommended Hubbard be institutionalised. Hubbard initially responded by kidnapping Sara. Thereafter, he took their daughter and fled to Havana. After Sara went public with her story, Hubbard returned her daughter. In his final known encounter with a psychiatrist, Hubbard consulted a practitioner in order to rebut public claims of his own mental illness.
Thereafter, Hubbard was increasingly hostile towards psychiatry. In the 50s, Hubbard sought to identify “Subversive” psychiatrists or other “Potential Subversives”. By the early 70s, Hubbard wrote of having redefined the word “psychiatrist” to mean “an antisocial enemy of the people”.
Hubbard’s Early Encounters with Psychiatry
Hubbard claimed to have personal encounters with several named psychiatrists beginning in his childhood. Some, like Thompson and White, would later be remembered favourably – Hubbard explicitly cited both as sources for his work. Others, such as Overholser and Center, were the subject of scorn.
Joseph Cheesman Thompson
In 1923, Navy medical doctor and psychoanalyst Joseph “Snake” Thompson accompanied Hubbard on a voyage. Hubbard recalled “I traveled with Commander Thompson from Seattle, Washington through the Panama Canal to Washington, D.C. when I was about twelve and knew him during all that time that I was in Washington and later.” Hubbard recalled that “[Thompson’s] friends called him ‘Snake’ and his enemies called him ‘Crazy’. He had lots of both.”[20] In another recording of Hubbard sharing anecdotes from his life, he considered Thompson to be a “very great man” who sparked Hubbard’s interest in “the human mind”. Hubbard said that Thompson told him, “If it’s not true for you, it’s not true.”
In 1952, Hubbard recalled that “I was just a kid and Commander Thompson didn’t have any boy of his own, and he and I just got along fine.” Hubbard continued “Why he [Thompson] took it into his head to start beating Freud into my head, I don’t know. But he did.”
In 1953, Hubbard argued “It’s very odd to realize, as I did one day, that in subsequent years I have approximated to a very remarkable degree the career of Commander Thompson – to show you what an impressed – impressionable boy can have handed to him suddenly.”
In 1954, Hubbard described an encounter with psychiatrists in which playing sports was seen as a positive indicator:
“I knew people, and the people who were trained by these people. And, if there was anything they were in awe of, it was somebody who engaged in sports. So this fellow was phenomenal to them. They knew this was very good somehow or another, but they couldn’t quite put their finger on it. And to this day it is enough to tell a psychiatrist that, and prove to him, that you are very energetic and engaged in sports, to have him dismiss you immediately as being completely sane. Only that’s just, bing. He just says, “Well, I…” He just goes into apathy right at that point. That’s the truth. “The… it was an interesting thing, for instance, to William Allen White. And Commander Thompson. Both of them, where I was concerned, that I wasn’t very interested in sitting around figuring about this stuff and didn’t seem to be terribly interested in the insane.”
Hubbard described later encounters with Thompson: “In 1930 I knew a fellow by the name of Commander Thompson. I had known him before, actually”.
In 1958, Hubbard told an audience: “I have made people feel better by using straight Freudian analysis the way I got it from Commander Thompson who imported it to the US Navy, not via Catherine [sic] Horney”.
Thompson died in 1943, seven years before the publication of Dianetics. Thompson was included in the Acknowledgements section of 1951’s Science of Survival, as was William A. White.
William Alanson White
William Alanson White was an American neurologist and psychiatrist who served as superintendent of St. Elizabeths Hospital. A letter from the Hubbard Association of Scientologists International to the FBI, dated 12 June 1954, claims that Hubbard was trained by both Joseph Thompson and William Alanson White. Hubbard recalled “Dr. William Alanson White, a very fine man. He was head of the big St. Elizabeth’s, the big mental institution there in Washington, D.C., and he had been a friend of mine for quite a while. I had met him through other friends of Dr. Thompson’s”. In a lecture, Hubbard described consulting White about a theoretical calculation of human memory capacity, apparently during Hubbard’s university days. Hubbard recalled that “he [White] used to see me every once in a while”.
In a 1951 lecture, Hubbard described St. Elizabeth’s as “where they sent the naval officers after they had received their fifth contradiction from the Navy Department”.
For two years in the 1920s, White had opened the doors of St. Elizabeths to Alfred Korzybski, enabling Korzybski to directly study mental illness, research that contributed heavily to Korzybski’s 1933 Science and Sanity: An Introduction to Non-Aristotelian Systems and General Semantics. Hubbard cited the relationship between Korzybski and White in his lectures.
White died in 1937, thirteen years before the publication of Dianetics. White was included in the Acknowledgements section of 1951’s Science of Survival, as was Joseph Thompson.
“Walnut Lodge”
For much of the 1920s and 30s, L. Ron Hubbard lived in Washington D.C. In 1932, Hubbard listed the US Naval Hospital in Washington as his address; In 1933, Hubbard listed a P.O. Box in Beallsville, Maryland.
In a 1952 lecture, Hubbard recalls his interaction with staff and patients at a facility specialising in schizophrenia which he calls “Walnut Lodge” (presumably Chestnut Lodge):
there’s a place by the name of Walnut Lodge. I… I… They don’t see anything humorous in that, by the way; it’s Walnut Lodge. […] They… they… they sent three people to see, to… to see me and every one of them was under treatment. And this was their staff. But anyway, very good people there, I’m sure, didn’t happen to meet any. Have some fine patients though. Anyway, they… they treat only schizophrenia. And so they take only schizophrenics. Now how do they get only schizophrenics? Well, anybody sent to Walnut Lodge is a classified schizophrenic. And they take somebody who is a dementia praecox unclassified or a more modern definition, a mania-depressive and they take him from Saint Elizabeth’s and they take him over to Walnut Lodge and he goes onto the books as a schizophrenic. Why? Because Walnut Lodge takes only schizophrenics.
In 1966, Hubbard recalled “Identification by classification. This is a type of thing Psychiatry does all the time. They say this is a Dementia Praecox case. They’ve gotten so idiotic with it now that if someboy goes to Chestnut Lodge… if a person is transferred to Chestnut Lodge, regardless of their symptoms before, they now have schizophrenia.”
Hubbard would return to “Walnut Lodge” in future writings. A 1970 bulletin states that “$2,000 a month for board only is the price at Walnut Lodge in Washington DC, an average place.” In his work Mission Earth, Hubbard writes “Arginal P. Pauper was today committed to Walnut Lodge Nut House”.
Hubbard as Patient
During World War Two, Hubbard was hospitalised at a California military hospital. After his release, he wrote to the Veterans Administration to request further treatment. Thereafter, he and his wife moved to Savannah, Georgia, where he was reportedly associated with a charity mental health clinic.
Oak Knoll Military Hospital
In 1945, Hubbard was a patient at Oak Knoll Military Hospital. Hubbard’s estranged son, L. Ron Hubbard, Jr., later known as Ron DeWolf, would later state that Hubbard received psychiatric treatment during his hospitalisation. Hubbard would later cite his time with psychiatric patients at Oak Knoll “using a park bench as a consulting room” as a major influence on his development of Dianetics.
Request for Psychiatric Treatment
After his discharge, Hubbard sought out psychiatric help to treat his “long periods of moroseness and suicidal inclinations” but reported that he could not afford it. A letter dated 15 October 1947, which Hubbard wrote to the Veterans Administration (VA) begins: “This is a request for treatment”. The letter continues:
After trying and failing for two years to regain my equilibrium in civil life, I am utterly unable to approach anything like my own competence. My last physician informed me that it might be very helpful if I were to be examined and perhaps treated psychiatrically or even by a psychoanalyst. Toward the end of my service I avoided out of pride any mental examinations, hoping that time would balance a mind which I had every reason to suppose was seriously affected. I cannot account for nor rise above long periods of moroseness and suicidal inclinations, and have newly come to realize that I must first triumph above this before I can hope to rehabilitate myself at all. … I cannot, myself, afford such treatment. Would you please help me?
The following year, Hubbard and his wife moved to Savannah, Georgia, where he was associated with a charity psychiatric clinic.
Hubbard as Would-Be Psychologist
After his arrival in Savannah, Hubbard began to describe himself as mental health practitioner, ultimately authoring Dianetics.
Savannah, Georgia Psychiatric Clinic
Beginning in June 1948, the nationally-syndicated wire service United Press ran a story on an American Legion-sponsored psychiatric ward in Savannah, Georgia, which sought to keep mentally-ill war veterans out of jail. That summer, Hubbard was arrested by the San Luis Obispo sheriff on a charge of petty theft for passing a fraudulent check.
In late 1948, Hubbard and his second wife Sara moved from California to Savannah, Georgia, where he would later claim to have “worked” as a “volunteer” in the psychiatric clinic, where he claimed he “processed an awful lot of Negroes”. Hubbard later wrote of having observed a “Dr. Center” in Savannah:
I well recall a conversation I had with a Dr. Center in Savannah, Georgia, in 1949. It well expresses the arrogance and complete contempt for law and order of the psychiatrist.
A man had just called to inquire after his wife who was “under treatment” in Center’s hospital. Center asked him, “Do you have the money…? That’s right, thirty thousand… well you better get it or I’ll have to send your dear wife to the state institution and you know what will happen then!”
I was there doing work on charity patients the local psychiatrists wouldn’t touch. Center had forgotten I was in the room.
In a 1966 interview, Hubbard recalled a man receiving a bill for psychoanalysis: “These people, you know, in psychoanalysis, they worked on somebody for a year just to find out if they could help him and then they charged him about 9000 quid for having not helped him”.
Dianetics
In January 1949, Hubbard wrote that he was working on a “book of psychology” about “the cause and cure of nervous tension”, which he was going to call The Dark Sword, Excalibur or Science of the Mind. In April 1949, Hubbard wrote from Savannah to inform the Gerontological Society at Baltimore City Hospital that he was preparing a paper entitled Certain Discoveries and Researches Leading to the Removal of Early Traumatic Experiences Including Attempted Abortion, Birth Shock and Infant Illnesses and Accidents with an Examination of their Effects Physiological and Psychological and their Potential Influence on Longevity on the Adult Individual with an Account of the Techniques Evolved and Employed. The Society apparently declined involvement.
He also wrote to the American Medical Association and the American Psychiatric Association. These letters, and their responses, have not been published, though Hubbard later said that they had been negative. Hubbard later wrote, “In 1948 I wrote a thesis on an elementary technique of application and submitted it to the medical and psychiatric professions for their use or consideration. The data was not utilized.”
In December 1949, Hubbard composed a letter to publisher John Campbell in which he provided an article entitled “A Criticism of Dianetics” to be published under the pen name Irving R. Kutzman, M.D. (ostensibly an opponent of Dianetic auditing). In his letter to Campbell, Hubbard described synthesizing the opinions of multiple doctors:
The philosophic derivation comments are direct quote from Davies of APA. The comment on operators is direct quote from Craig, MD PhD of Savannah.[53][54] The pre-frontal lobotomy angle (changed only to trans-orbital leukotomy) is a direct quote from Delchamp, MD PhD. You heard nearly all these things repeated by Kahn, MD and he did not diverge in any particular from the standard attitude toward Dianetics, General Semantics (quote on this from Davies of APA), Cybernetics (Boswell, MD) etc. etc. This article would be found by an MD psychiatrist to be a pretty valid statement of their case because they have so stated the case many times.
The following year, Hubbard authored Dianetics: the Modern Science of Mental Health, a handbook for “the psychiatrist, psycho-analyst and intelligent layman”.
By September 1950, the American Psychological Association’s governing body unanimously adopted a resolution advising its members against using Hubbard’s techniques with their patients and leading psychologists spoke out against Dianetics. Thereafter, Hubbard was critical of psychiatry.
Winfred Overholser was superintendent of St. Elizabeths Hospital after 1937. By 1950, he was president of the American Psychiatric Association. In a 1953 lecture, Hubbard claimed:
Doctor Upholstered is in charge of … he’s in charge of the rest home for feeble minded government officials here in Washington, Saint Elizabeths.
In 1972, Hubbard recalled:
he [Overholser] blew the whistle on Dianetics when St. Elizabeth psychiatrists were just beginning to use it and were for the first time getting results on patients at the National Asylum. He forbade them to use it but they disagreed heavily and privately used it for many years under cover. This broke up introducing Dianetics on regular channels – May 1950.
Thereafter a violent and gory attack was mounted. It was begun by Oberholser, went over to George Wash U. Psychology Dept at once and there a student of the first Dianetics class (Dolly Jones) also a psychology student was hypnotized, beaten, told to go crazy, did so and we had to hospitalize her.
[…] He (Oberholser) was a member of the Club.
In another lecture, Hubbard claimed he gave a speech in which he hypnotized the staff of St. Elizabeth’s.
In late 1950, Hubbard criticised mainstream psychiatry but still wrote positively of Sigmund Freud as a fellow persecuted trailblazer, arguing that “to talk of the faults of Freud, as do those who practice psychoanalysis today, is ungenerous. This great pioneer, against the violent objections of medical doctors and the psychiatrists of his day, ventured to put forth the theory that memory was connected with present time behavior” Hubbard elaborated: “Freud was so thoroughly shunned by neurologists of his day and medicine ever since, that only his great literary skill brought his work as far as it has come.”
As late as 1955, Hubbard still identified himself with mental health professions, describing himself as “a writer, a scientist, and a psychologist”.
Attempted Institutionalisation and Aftermath
In 1951, Hubbard’s wife Sara sought advice from a psychiatrist who recommend Hubbard be institutionalised. Upon learning of the plan, Hubbard initially kidnapped Sara; After her release, Hubbard fled to Havana with their young daughter. Hubbard then underwent a public divorce in which his wife publicly alleged that Hubbard had been diagnosed with paranoid schizophrenia. Upon his return to the US, Hubbard consulted with a psychiatrist to rebut public claims of his mental illness.
Sara Consults Psychiatrist
In 1951, Hubbard’s wife Sara went to a psychiatrist to obtain advice about his increasingly violent and irrational behaviour, and was told that he probably needed to be institutionalised and that she was in serious danger. She gave Hubbard an ultimatum: get treatment or she would leave with the baby. He was furious and threatened to kill their daughter Alexis rather than let Northrup care for her. Sara later recalled: “He didn’t want her to be brought up by me because I was in league with the doctors. He thought I had thrown in with the psychiatrists, with the devils.”
In a letter to the Attorney General dated May 1951, Hubbard claims that on “Feb. 25 she [Sara] flew to San Francisco and my general managers Jack Maloney in New Jersey received a phone call from her and Miles Hollister and a psychiatrist named Meyer Zelig in San Francisco that I had gone insane and that they needed money to incarcerate me quickly.”
Two decades later, in 1972, Hubbard would write to followers:
the NY Times Literary Section began an attack and a lot of violent track ran by which included DR. MEYER-ZELIG, a psychiatrist in San Francisco master-minding a kidnapping of me to fly me to St. Louis and be put away. His (Zelig’s) plans miscarried. MILES HOLLISTER, formerly a psych student, got hold of SARA NORTHRUP (really Komknoidominoff) (or ov) and handed her over to Zelig who put her in deep hypnosis, fixated her on the idea I was trying to kill her and spun her in, in which state she has remained since. This caused the final destruction of the HDRF (Hubbard Dianetic Research Foundation) as national press only played up her divorce.
Hubbard Kidnaps Wife, Daughter
On the night of 24 February, 1951, Hubbard allegedly took daughter Alexis while Sara was at a movie theatre. A few hours later, he returned with two of his Dianetics Foundation staff and told Sara, who was now back at her apartment: “We have Alexis and you’ll never see her alive unless you come with us.” She was bundled into the back of a car and driven to San Bernardino, California, where Hubbard attempted to find a doctor to examine his wife and declare her insane. His search was unsuccessful and he released her at Yuma Airport across the state line in Arizona. He promised that he would tell her where Alexis was if she signed a piece of paper saying that she had gone with him voluntarily. She agreed but Hubbard reneged on the deal and flew to Chicago, where he found a psychologist who wrote a favourable report about his mental condition to refute Northrup’s accusations. Rather than telling Northrup where Alexis was, he called her and said that “he had cut [Alexis] into little pieces and dropped the pieces in a river and that he had seen little arms and legs floating down the river and it was my fault, I’d done it because I’d left him.”
From March to May 1951, Hubbard fled to Havana with his infant daughter. According to his estranged son Ronald DeWolf, Hubbard was under psychiatric care at this time.
Public Allegation of Hubbard having ‘Paranoid Schizophrenia’
After her release, Sara filed for divorce, charging Hubbard with causing her “extreme cruelty, great mental anguish and physical suffering”. Her allegations produced more lurid headlines: not only was Hubbard accused of bigamy and kidnapping, but she had been subjected to “systematic torture, including loss of sleep, beatings, and strangulations and scientific experiments”. Because of his “crazy misconduct” she was in “hourly fear of both the life of herself and of her infant daughter, who she has not seen for two months”.
On 23 April 1951, it was publicly reported that Sara had consulted doctors who “concluded that said Hubbard was hopelessly insane, and crazy, and that there was no hope for said Hubbard, or any reason for her to endure further; that competent medical advisers recommended that said Hubbard be committed to a private sanatorium for psychiatric observation and treatment of a mental ailment known as paranoid schizophrenia.” The San Francisco Chronicle coverage used the headline “Ron Hubbard Insane, Says His Wife”.
Hubbard’s lover, Barbara Klowden, recorded in her journal:
He [Hubbard] talked about what he was going to do to psychiatrists.
How he brought psychotic into present time in psychiatrists office and how that psychiatrist said to him “If you think you’ve cured this woman you’re crazy. If you claim to cure people by doing that, if you’re not careful, we’ll lock you up.” He laughed and laughed.
Then, tearing indignantly at chicken leg, he said “They all came to me and said I was a psychotic. Hah. They called me a paranoid. Can you imagine?”
My blood ran cold as he was saying that and it was all I could do to keep from weeping. Wouldn’t it tear your heart out coming from the one you love when you knew all the time was a psychotic and a paranoid?
Psychiatry as Evil
In 1955, Hubbard wrote that “nearly all the backlash in society against Dianetics and Scientology has a common source — the psychiatrist-psychologist-psychoanalyst clique”. In a letter addressed to the FBI dated 11 July, Hubbard reports having been the victim of an “attack made by psychiatrists using evidently Communist connected personnel”.
In 1956, Hubbard wrote an article entitled “A Critique of Psychoanalysis” which embodies Hubbard’s harder stance. Writes Hubbard: “Now and then it becomes necessary to eradicate from a new subject things which it has inherited from an old. And only because this has become necessary am I persuaded to tread upon the toes of the “grandfather” to Dianetics and Scientology.” In the essay, Hubbard admits that from “the earliest beginnings of Dianetics it is possible to trace a considerable psychoanalytic influence.” Hubbard makes a distinction between Dianetics and Scientology writing that “Scientology, unlike Dianetics, is not a psychotherapy. It is therefore from the dominance of Scientology rather than from the viewpoint of Dianetics that one can understand the failings of psychoanalysis, its dangers and the reasons why it did not produce what it should have produced.”
We discover psychoanalysis to have been superseded by tyrannous sadism, practiced by unprincipled men, themselves evidently in the last stages of dementia. This, then, is the end of the trail for psychoanalysis—a world of failure and brutality. Today men who call themselves analysts are merrily sawing out patients’ brains, shocking them with murderous drugs, striking them with high voltages, burying them underneath mounds of ice, placing them in restraints, “sterilizing” them sexually and generally conducting themselves much as their patients would were they given the chance. It is up to us to realize, then, that psychoanalysis in its pure practice is dead the moment the spirit of humanity in which Freud developed the work is betrayed by the handing over of a patient to the merciless misconduct which passes today for treatment.
In 1957, Hubbard founded the “National Academy of American Psychology” which sought to issue a “loyalty oath” to psychologists and psychiatrists. Those who opposed the oath were to be labelled “Subversive” psychiatrists, while those who merely refused to sign the oath would be labelled “Potentially Subversive”.
In 1958, Hubbard wrote that “Destroy is the same as help to a psychiatrist”. His 1958 writings cited “Psychiatry: The Greatest Flub of the Russian Civilization” by Tom Esterbrook; Hubbard’s son would later reveal that Tom Eastebrook was one of Hubbard’s many pen-names.
In 1966 Hubbard declared all-out war on psychiatry, telling Scientologists that “We want at least one bad mark on every psychiatrist in England, a murder, an assault, or a rape or more than one.” He committed the Church of Scientology to the goal of eradicating psychiatry in 1969, announcing that “Our war has been forced to become ‘To take over absolutely the field of mental healing on this planet in all forms.'”
By 1967, Hubbard claimed that psychiatrists were behind a worldwide conspiracy to attack Scientology and create a “world government” run by psychiatrists on behalf of the USSR:
Our enemies are less than twelve men. They are members of the Bank of England and other higher financial circles. They own and control newspaper chains and they, oddly enough, run all the mental health groups in the world that had sprung up […]. Their apparent programme was to use mental health, which is to say psychiatric electric shock and pre-frontal lobotomy, to remove from their path any political dissenters […]. These fellows have gotten nearly every government in the world to owe them considerable quantities of money through various chicaneries and they control, of course, income tax, government finance — [Harold] Wilson, for instance, the current Premier of England, is totally involved with these fellows and talks about nothing else actually.
Referring to psychiatrists as “psychs”, Hubbard wrote of psychiatrists as denying human spirituality and peddling fake cures. He taught that psychiatrists were themselves deeply unethical individuals, committing “extortion, mayhem and murder. Our files are full of evidence on them.”
Hubbard’s efforts to cast the field of psychiatry as the source of all of humanity’s problems are exemplified in a policy letter written in 1971, in which he attempted to redefine the word “psychiatrist” to mean “an antisocial enemy of the people”:
Psychiatry and psychiatrist are easily redefined to mean ‘an antisocial enemy of the people.’ This takes the kill-crazy psychiatrist off the preferred list of professions. This is a good use of the technique [of redefining words] as for a century the psychiatrist has been setting an all-time record for inhumanity to Man.
Anti-psychiatric themes also appear in some of Hubbard’s later fictional works. In Hubbard’s ten-volume series Mission Earth, various characters debate the methods and validity of psychology. In his novel Battlefield Earth, the evil Catrists (a pun on psychiatrists), are described as a group of charlatans claiming to be mental health experts.
The Church of Scientology and Psychiatry
A 1969 book, Believe What You Like, described an attempt by Scientologists to secretly infiltrate the National Association of Mental Health in Britain and turn official policy against mental health treatment. Though they were expelled from the organization after their identity and mission were revealed, the Church of Scientology then filed a number of suits against the NAMH.
When Operation Snow White, a Church of Scientology campaign to purge unfavorable records about Scientology and its founder L. Ron Hubbard, was revealed in 1980, it came to light that Scientology agents of the Guardian’s Office had also conducted a similar campaign against the World Federation for Mental Health and the National Association of Mental Health.
Scientology’s views are expressed by its president in the following quote:
What the Church opposes are brutal, inhumane psychiatric treatments. It does so for three principal reasons: 1) procedures such as electro-shock, drugs and lobotomy injure, maim and destroy people in the guise of help; 2) psychiatry is not a science and has no proven methods to justify the billions of dollars of government funds that are poured into it; and 3) psychiatric theories that man is a mere animal have been used to rationalize, for example, the wholesale slaughter of human beings in World Wars I and II.
An October 2006 article in the Evening Standard underlines the strong opposition of Scientology toward the psychiatric profession:
Up front, David Miscavige is dramatically — and somewhat bizarrely — attacking psychiatrists, his words backed by clips from a Scientology-produced DVD are broadcast on four giant high-definition TV screens and sensationally called: Psychiatry: an industry of death […]. ‘A woman is safer in a park at midnight than on a psychiatrist’s couch’, booms Miscavige, backed by savage graphics of psychiatrists — or ‘psychs’ as he calls them — being machine-gunned out of existence.
The group says that they are near victory in their war against psychiatry. In their treatise Those Who Oppose Scientology, it is stated:
Today, there are 500 Dianeticists and Scientologists to every psychiatrist […] while Scientology is more visible than ever, with churches dotting every continent on Earth and millions of parishioners around the world, one is hard pressed to find even a single psychiatrist with a shingle on his door.
Scientology claims a worldwide membership of more than 8 million, the total of people who have taken the Scientology introductory course. The Church of Scientology claims 3.5 million members in the United States, though an independent survey has found the number of people in the United States would state their religion as ‘Scientology’ is close to 55,000. By comparison, the American Psychiatric Association and the American Psychological Association, which are composed of psychiatrists and psychologists, have 38,000 and 148,000 members respectively.
Mental health care professionals are not concerned that the public will take Citizens Commission on Human Rights (CCHR) materials seriously, because of the organisation’s connection with the church; however, they argue that these materials can have a harmful impact when quoted without attribution.
Except for court trials and media publications and public rallies, published materials have received little notice outside of Scientology and CCHR; of reviews available, few are positive. Psychology professor Benjamin Beit-Hallahmi’s short review of Psychiatrists: The Men Behind Hitler states:
Scientology has attracted much attention through its propaganda effort against what it calls psychiatry. This has involved great expense and organizational effort, carried out through a variety of fronts. If the book Psychiatrists: The Men Behind Hitler (Roder, Kubillus, & Burwell, 1995) is a representative example, and I believe it is, it proves decisively that the campaign is rooted in total paranoia and pathetic ignorance. Reading this book, and I will urge you not to waste too much time doing it, makes clear that the authors simply have no idea what psychiatry is.
The American Psychiatric Association’s Lynn Schultz-Writsel adds:
We have not responded in any way, shape or form. There has not been a hue and cry from members to respond. And anyway, the publication speaks for itself.
Michael Burke, the president of the Kansas Psychiatric Association, said regarding Scientology, “They aren’t really able to support their position with any scientific data, which they tend to ignore. … the public seems to be able to look right past the Scientology hoopla.”
The commercial motivation of Scientology in questioning psychiatry, with their alternative practice, dianetics, has been questioned by Peter W. Huber.
According to Susan Raine in Scientology in Popular Culture (2017), The Church of Scientology’s programs against psychiatry “complicates the movement’s quest for religious legitimacy.” This is because of “the way in which Hubbard tried to replace psychiatry, psychology and other forms of counseling and therapy with Scientology.”
In a 2017 article in The Humanistic Psychologist, John H. Wolfe notes that Scientology has been widely discredited, and describes the ways in which Scientology differs from mainstream psychotherapy. He mentions that Scientology counselling is systematically thorough, meaning it considers a client’s issue individually and thoroughly before moving on to the next one. Wolfe also compares Scientology auditing to the “nondirective therapy” of Carl Rogers, “who stressed the importance of having the client find the client’s own answers, while the counselor refrains from interpretation, but listens with empathic understanding.” Unlike Roger’s technique however, Scientology’s auditors ask leading questions, instead of letting them independently stumble upon answers on their own.
Legal Waivers
Following legal actions involving the Church of Scientology’s relationship with its members, it has become standard practice within the group for members to sign lengthy legal contracts and waivers before engaging in Scientology services. In 2003, a series of media reports examined the legal contracts required by Scientology, which require that, among other things, Scientology followers deny any and all psychiatric care that their doctors may prescribe to them:
I do not believe in or subscribe to psychiatric labels for individuals. It is my strongly held religious belief that all mental problems are spiritual in nature and that there is no such thing as a mentally incompetent person — only those suffering from spiritual upset of one kind or another dramatized by an individual. I reject all psychiatric labels and intend for this Contract to clearly memorialize my desire to be helped exclusively through religious, spiritual means and not through any form of psychiatric treatment, specifically including involuntary commitment based on so-called lack of competence. Under no circumstances, at any time, do I wish to be denied my right to care from members of my religion to the exclusion of psychiatric care or psychiatric directed care, regardless of what any psychiatrist, medical person, designated member of the state or family member may assert supposedly on my behalf.
Citizens Commission on Human Rights
The Citizens Commission on Human Rights (CCHR), an institution set up by Scientology and Thomas Szasz, also claims that the real nature of psychiatry is that of human rights abuse.
In 1966, Hubbard declared all-out war on psychiatry, telling Scientologists that “We want at least one bad mark on every psychiatrist in England, a murder, an assault, or a rape or more than one.” He committed the Church of Scientology to the goal of eradicating psychiatry in 1969, announcing that “Our war has been forced to become ‘To take over absolutely the field of mental healing on this planet in all forms.'”
Not coincidentally, the Church of Scientology founded the Citizens Commission on Human Rights that same year as its primary vehicle for attacking psychiatry. CCHR still quotes Hubbard’s above-cited statement that all psychiatrists are criminals: “There is not one institutional psychiatrist alive who, by ordinary criminal law, could not be arraigned and convicted of extortion, mayhem and murder. Our files are full of evidence on them.”
CCHR has conducted campaigns against Prozac, against electroconvulsive therapy, against Ritalin (and the existence of ADHD) and against various health legislations. CCHR opened an exhibit in their building: Psychiatry: An Industry of Death.
Tom Cruise
Tom Cruise has been highly vocal in attacking the use of psychiatric medication, gaining particular attention for becoming extremely animated on the subject during an interview on Today on 25 June 2005. His position has attracted considerable criticism from psychiatrists and other physicians (American Psychiatric Association and National Mental Health Association), and individuals suffering from depression.
In January 2004, Cruise made the controversial statement “I think psychiatry should be outlawed.” Further controversy erupted in 2005 after he openly criticised actress Brooke Shields for using the drug Paxil (paroxetine), an anti-depressant to which Shields attributes her recovery from postpartum depression after the birth of her first daughter in 2003. Cruise asserted that there is no such thing as a chemical imbalance and that psychiatry is a form of pseudoscience. Shields responded that Cruise “should stick to saving the world from aliens and let women who are experiencing postpartum depression decide what treatment options are best for them”. This led to a heated argument between Matt Lauer and Cruise on NBC’s Today on 24 June 2005.
Medical authorities view Cruise’s comments as furthering the social stigma of mental illness. Shields herself called Cruise’s comments “a disservice to mothers everywhere.” In late August 2006, Cruise apologised in person to Shields for his comments.
Scientology is well known for its opposition to mainstream psychiatry and the psychoactive drugs which are routinely prescribed for treatment. It was reported that Cruise’s anti-psychiatry actions led to a rift with director Steven Spielberg. Spielberg had reportedly mentioned in Cruise’s presence the name of a doctor friend who prescribed psychiatric medication. Shortly thereafter, the doctor’s office was picketed by Scientologists, reportedly angering Spielberg.
Books by Scientologists
Bruce Wiseman from CCHR published the book Psychiatry: The Ultimate Betrayal (Scientology’s Freedom Publications, 1995), in which he portrays psychiatry as creating Adolf Hitler.
The German Scientologists Thomas Roder and Volker Kubillus wrote the book Psychiatrists: the Men Behind Hitler (also published by Scientology’s Freedom Publications, 1995–2001), that advances a conspiracy theory of all-powerful psychiatrists to overwhelm the world.
Death of Lisa McPherson
In 1994, Scientologist Lisa McPherson moved from Dallas, Texas, to Clearwater, Florida, with her employer, AMC Publishing, which was at that time owned by Bennetta Slaughter and operated and staffed primarily by Scientologists. During June 1995, the church placed McPherson in an “introspection rundown” due to perceived mental instability. Lisa completed the rundown, and she attested to the state of Clear in September.
On 18 November 1995, McPherson was involved in a minor car accident. Paramedics initially left her alone because she was ambulatory, but after she began to remove her clothes, the paramedics decided to take her to the hospital. She remarked to the paramedics that she had taken off her clothes in hopes of obtaining counselling. Hospital staff agreed that she was unharmed, but recommended keeping her overnight for observation. Following intervention by fellow Scientologists, McPherson refused psychiatric observation or admission at the hospital and checked herself out after a short evaluation.
Pinellas-Pasco Circuit Judge Frank Quesada concluded:
Lisa McPherson refused psychiatric observation or admission at the hospital; she expressly stated her desire to receive the religious care and assistance from her fellow congregants that she and they wanted her to have.
McPherson was then taken to the Flag Land Base for “rest and relaxation” according to the Church of Scientology, but sworn statements demonstrate that McPherson was brought there for another introspection rundown.
Mark McGarry, an attorney with the Florida Office of the State Attorney, characterised McPherson’s stay at the Flag Land Base as an “isolation watch”:
My understanding now is, from talking to many, many witnesses, the purpose of her being there in the Church, correct me if I’m wrong, she was experiencing some mental problems, and you guys were going to stabilize her through an isolation watch. And after that watch occurred, there was going to be a procedure run on her, and the procedure was an introspection rundown.
The church accommodated McPherson in a cabana and kept a “24 hours’ watch” over her. Detailed logs were kept on McPherson’s day-to-day care. These logs were handwritten on plain white paper. Most of these logs were kept but the logs for the last three days were summarised from the originals and the originals shredded. Brian J. Anderson, the then Commanding Officer of the Church’s Office of Special Affairs (OSA) in Clearwater, said in his sworn statement:
I saw the handwritten notes, gave a cursory look to see if the summary—see if they matched and matched, and I threw the handwritten reports in my shred basket, and I had the report, kept the report.
McPherson’s “care logs” narrate the last seventeen days of her life: she was incoherent and sometimes violent, her nails were cut so she would not scratch herself or the staff, she bruised her fists and feet while hitting the wall. She had trouble sleeping and was being given natural supplements and the drug chloral hydrate to help her sleep. A Church staffer noted that McPherson “looked ill like measles or chicken pox on her face.” On repeated occasions she refused food and protein shakes that the staff offered. On 26 and 30 November and 03 to 04 December, the staff attempted to force feed her, noting that she spat the food out. She was noted to be very weak, not standing up nor on some days moving at all. Scientologists who questioned this handling were told to “butt out”.
On 05 December 1995, the Church staffers contacted David Minkoff, a Scientologist medical doctor who twice prescribed McPherson Valium and chloral hydrate without examining her. They requested for him to prescribe an antibiotic to McPherson because she seemed to have an infection. Minkoff refused and stated that McPherson should be taken to a hospital and he needed to see her before prescribing anything. They objected, expressing fear that McPherson would be put under psychiatric care. Dr. Janice Johnson, a senior medical officer at Flag Land Base who was assigned to care for McPherson, stated that McPherson had been gasping and had laboured breathing while en route. However they passed a total of four hospitals along the way to their ultimate destination. When they arrived at Minkoff’s hospital 45 minutes north of Clearwater, McPherson exhibited no vital signs. Hospital staff attempted to resuscitate her for 20 minutes before declaring her dead.
Jeremy Perkins
On 13 March 2003, Scientologist Jeremy Perkins killed his mother, Elli, by stabbing her 77 times. Jeremy, previously diagnosed with schizophrenia, never received treatment after previous incidents with violence and hallucinations. His mother, active in the Buffalo Church of Scientology, felt that vitamins and Scientology routines were better than psychological counselling and anti-psychotic medication.
Linda Waliki
On 05 July 2007, a 25-year-old Australian woman, Linda Waliki, killed her 52-year-old father Michael, 15-year-old sister Kathryn, and injured her mother Sue with a knife. Her name was released in the print edition of the Sydney Morning Herald, on 07 July 2007. It was previously unreleased due to one of the victims being under age. She was diagnosed with a psychiatric illness, but her parents denied her continued psychiatric treatment due to their Scientology beliefs. Instead they replaced this medication with one specially imported from Scientologists in the United States.
Relations with Anti-Psychiatry Movement
The Citizens Commission on Human Rights was co-founded by anti-psychiatrist Thomas Szasz and the Church of Scientology in 1969. Some anti-psychiatry websites and psychiatric survivors groups have sought to distance themselves from Scientology and the CCHR. In particular, the organisation Mind Freedom has specifically made public statements to emphasise that it is not connected with either CCHR or the Church of Scientology.
Despite sharing notable anti-psychiatry views on some issues with the secular critics, Scientology doctrine does differ in some respects. Scientology has promoted psychiatry-related conspiracy theories, including that psychiatrists were behind the Yugoslav Wars and that 11 September was caused by psychiatrists. Scientologists are committed never to take psychiatric drugs and to reject psychology outright.
The socio-political roots of the movements have different origins. Advocates of the anti-psychiatric world view such as David Cooper, R.D. Laing and Michel Foucault had ties with the political left of the 1960s; Thomas Szasz, with the civil libertarians of the right, as well as an outspoken atheist. Many advocates of the anti-psychiatry movement have stated that they consider the idea of “mental illness” as a convenient and inaccurate label assigned by society rather than an objective biomedical state, rejecting psychiatric terms such as schizophrenia which they may see as stigmatising. By contrast, Hubbard referred to “schizophrenics” in his writings on Scientology theory, and developed the emotional tone scale to, in part, gauge the health of a person’s mental state. Furthermore, in his Science of Survival Hubbard suggested putting people very low on the scale into quarantine, a practice at odds with, for instance, the aim of the American Association for the Abolition of Involuntary Mental Hospitalisation: an organisation co-founded by Szasz to end involuntary commitment.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Scientology_and_psychiatry >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Elizabeth F. Loftus (born 1944) is an American psychologist who is best known in relation to the misinformation effect, false memory and criticism of recovered memory therapies.
Loftus’s research includes the effects of phrasing on the perceptions of automobile crashes, the “lost in the mall” technique and the manipulation of food preferences through the use of false memories. In the Jane Doe case that began in 1997, Loftus and Melvin J. Guyer revealed serious concerns about the background and validity of the initial research. She has also served on the executive council of the Committee for Skeptical Inquiry and was a keynote speaker at the British Psychological Society‘s 2011 annual conference.
As well as her scientific work, Loftus has provided expert testimony or consultation for lawyers in over 300 court cases, including for the legal teams of Ghislaine Maxwell, Harvey Weinstein, Ted Bundy, O.J. Simpson, Angelo Buono and Robert Durst. She has also written many books, including The Myth of Repressed Memory: False Memories & Allegations of Sexual Abuse and Witness for the Defense.
Early Life and Education
Born Elizabeth Fishman on 16 October 1944, Loftus grew up in a Jewish family in Bel Air, California. Her father (Sidney Fishman) was a doctor and her mother (Rebecca Fishman) a librarian. When Loftus was 14 years old, her mother drowned.
She received a Bachelor of Arts degree in mathematics and psychology from the University of California, Los Angeles, in 1966, followed by a master’s and PhD in mathematical psychology from Stanford University in 1967 and 1970 respectively. Her thesis was entitled “An Analysis of the Structural Variables That Determine Problem-Solving Difficulty on a Computer-Based Teletype”.
Career
1970 to 1989
From 1970 to 1973, Loftus was employed as a cognitive psychologist at the New School for Social Research in New York City, after becoming dissatisfied with university work such as calibrating math and word problems for fifth-grade students. At the time, she had also been investigating semantic memory with Professor Jonathan Freedman at Stanford University.
Loftus was employed at the University of Washington from 1973 to 2001, initially as an assistant professor. She shifted from laboratory work to using “real world” situations of criminal court cases.
Around this time, the United States Department of Transportation was offering funding for research into car crashes. Loftus’s first experiment in this area involved showing 45 students videos of car crashes and then asking the students to estimate the speed of the car. Her findings were that the mean estimates of the speeds were 32 mph when the question was phrased as the speed that the cars “collided”, 34 mph when the question was phrased as “hit each other” instead, and 41 mph when the question was phrased as “smashed each other”. Loftus concluded that “these results are consistent with the view that the questions asked subsequent to an event can cause a reconstruction in one’s memory of that event”.
In 1974, Loftus published two articles with her observations about the conflicting eyewitness accounts in a particular murder trial and about the reliability of witness testimony in general. This resulted in several lawyers contacting her about current cases, beginning her career of paid work providing advice to lawyers. Early attempts for Loftus to act as an expert witness for these lawyers were deemed inadmissible by judges, however in June 1975 Loftus presented the first expert witness testimony in Washington State on the topic of eyewitness identification.
1990 to 1996
In 1990, George Franklin was on trial for murdering a young girl 20 years prior. The prosecution’s evidence included eyewitness testimony from Franklin’s daughter that she had witnessed the murder, based on a recovered memory which was unearthed during a therapy session a year before the trial. The defence attorney had a theory that the daughter had never seen the crime and that the testimony was based on a false memory. Loftus was employed by the attorney to provide expert testimony in support of this theory. Loftus referred to an experiment where she showed people video of a crime and then an incorrect television news report about the crime. Afterwards, the viewers had mixed up some events from the original video with those in the news report. Loftus argued that the same must have happened to Franklin’s daughter, causing a “memory” of an event that she had not witnessed.
However, the prosecutor forced Loftus to admit that she had never studied memories like those of Franklin’s daughter. Loftus’s studies found that people could misidentify random perpetrators, not that they could mistakenly accuse their own fathers. It was also not proven that memories could be wholly invented, rather than altered. The prosecution was successful and Franklin was convicted, though the conviction was later overturned on appeal and the prosecution declined to retry Franklin.
In 1991 there were several high-profile court cases of people having recovered memories of having been molested by their parents, which gained Loftus’s attention. She read through several then-current psychology books (The Courage to Heal) which instructed women and therapists in methods of recovering “lost” memories of sexual abuse, and urging therapists to query their clients about childhood incest. Also in 1991, Loftus was deemed an honorary fellow of the British Psychological Society.
Around this time, Loftus’s undergraduate student Jim Coan developed the “lost in the mall” technique. This technique involved Coan giving his younger brother three stories of actual events from his childhood, plus a false story about the brother being lost in a mall. The younger brother believed all stories to be true and provided further details of the false story.
A similar experiment by Loftus found that 25% of subjects believed that they could remember the event which had never taken place; however, this study was criticised by Lynn Crook and Martha Dean based on the ethics of the subject recruitment method used and Kenneth Pope has argued she overgeneralised the findings to draw conclusions about false memories and therapeutic techniques. A later study by Loftus (involving 332 undergraduate students who received course credit for participating) found that approximately one third of students accepted as true a false story about having their ear licked by a drug-addled Pluto character during a childhood visit to Disneyland.
Following the publication of these studies, armed guards accompanied Loftus at lectures. Also, Loftus had previously received death threats after the publication of her 1994 book The Myth of Repressed Memory. The same year, Loftus received an In Praise of Reason award from the Committee for Skeptical Inquiry.
In the 1997 New Hampshire vs Joel Hungerford case, the judge set strict conditions on the admissibility of recovered memory testimony.
1997 to 2000
In 1997, psychiatrists David Corwin and Erna Olafson published a case study of a recovered memory of apparently genuine childhood sexual abuse, which became known as the Jane Doe case. Loftus and Melvin Guyer interviewed Jane’s stepmother who revealed that she was involved in building a case against Jane’s mother in a battle for custody of Jane. Jane contacted the University of Washington and accused Loftus of breaching her privacy. The university put Loftus under investigation, including confiscating her files. The investigation lasted for 21 months, during which time Loftus was not allowed to share her findings. The university cleared Loftus of breaking research protocols, and Loftus and Guyer published their findings in 2002.
Loftus’s invitation to give the keynote address at the New Zealand Psychological Society’s conference in August 2000 provoked the society’s director of scientific affairs, John Read, to resign from his position and for conference attendees to distribute materials critical of Loftus’s work. Loftus stated that she “didn’t wear her best jacket” to give her address for “fear of flying tomatoes”. Prior to the conference, Loftus was the subject of several internet posts by conspiracy theorist Diana Napolis which alleged that Loftus was conspiring to help child molesters.
2001 to Present
By 2001, Loftus had become disappointed with the University of Washington’s unwillingness to stand by her during the controversy involving the Jane Doe case, and she left the university. The same year, Loftus received a William James Fellow Award from the Association for Psychological Science.
From 2001 to 2003, Loftus worked for the University of California, Irvine, (UCI) as a distinguished professor in the department of Criminology, Law and Society and the department of Psychological Science. She was also a fellow in the UCI Department of Cognitive Sciences and the Centre for the Neurobiology of Learning and Memory. Her work included an experiment on 131 undergraduate students in relation to preferences for cookies and strawberry ice cream. The students were given false information that they had become sick from these foods when they were under 10 years old, and were asked before and afterwards to rate the likelihood of this event having occurred.
In 2002, Loftus was ranked 58th in the Review of General Psychology’s list of the 100 most influential psychological researchers of the 20th century. The following year, Loftus received the award for Distinguished Scientific Applications of Psychology from the American Psychological Association (APA). Also in 2003, Loftus was elected a fellow of the American Academy of Arts and Sciences.
In 2003, the Taus v. Loftus case in the Supreme Court of California saw Loftus, Melvin J. Guyer and Skeptical Inquirer magazine being sued by Nicole Taus regarding the article they published about her case. The lawsuit included 21 claims of defamation, invasion of privacy, infliction of emotional distress and fraud. Initially, all but one of the claims was dismissed. The remaining claim was regarding Loftus’ self- misrepresentation as Corwin’s colleague and supervisor while interviewing Taus’s foster mother. In August 2007, the remaining claim was withdrawn by Taus, after reaching an agreement that Loftus’s insurance company would pay a settlement of $7,500 to Nicole Taus. The following year, Loftus published her studies on the case.
In 2004, she attempted to implant a false memory in Alan Alda on Scientific American Frontiers. Alda did not accept the false memory of becoming sick as a child from eating a hard-boiled egg. Loftus stated that Alda’s questionnaire self-correction from “definitely didn’t happen” to “happened” supported the false memory theory. The variance in Alda’s pre- and post-experiment responses was not stated. Loftus attended and was a speaker at the Beyond Belief symposium in November 2006. In 2005, she received the Grawemeyer Award in psychology from the University of Louisville. In 2009, she received the Joseph Priestley Award presented by Dickinson College. In 2010, she received the Scientific Freedom and Responsibility Award from the American Association for the Advancement of Science.
From 2011, Loftus was on the executive council of the Committee for Skeptical Inquiry. Loftus was a keynote speaker at the British Psychological Society’s annual conference in 2011.
In June 2013, Loftus presented at the TEDGlobal Conference in Edinburgh, Scotland. She was also the keynote speaker at the 2013 Psychonomic Society annual meeting. In 2015, Loftus received an honorary doctorate in psychology from Goldsmiths, University of London. In 2016, Loftus received the John Maddox Prize, In 2018, she won the Western Psychological Association’s Lifetime Achievement Award and the University College Dublin’s Ulysses Medal.
In 2022, Loftus made Research.com’s list of world’s top female scientists, ranking at No. 451 in the United States.
The Recovered Memory / False Memory Debate
Elizabeth Loftus has been an active participant in controversies over memory since the last decades of the 20th century, known as the recovered memory / false memory debate, or as the “Memory Wars” (as in the title of the book The Memory Wars).
Loftus was a member of the False Memory Syndrome Foundation Scientific Advisory Board. She along with Peter Freyd, Pamela Freyd and the False Memory Syndrome Foundation have argued that there is sufficient experimental evidence that people distort their memories, that human memory is not usually faithful to objective facts, and that false memories can be implanted in other people through suggestion and recovered-memory therapy. Thus, in many or most cases, the memories of childhood abuse that people recover in psychotherapy, and which are sometimes presented in court, are false memories.
Other scholars and specialists including Bessel van der Kolk, Lenore Terr, Jennifer Freyd and Linda Williams argue that there are well-documented cases of forgetting and later remembering traumatic events that occurred during childhood or adulthood by people in both clinical and non-clinical populations.
Elizabeth Loftus has argued that the concept of memory inhibition or repression is inadequate and that there is no such thing as repressed and later recovered memories of traumatic events. Loftus criticises recovered-memory therapy and in particular Freud’s psychoanalysis for spreading these inadequate concepts.
Richard McNally argues that forgetting of childhood abuse events can be explained by other factors such as ordinary forgetting or nondisclosure and that the theory of a motivational mechanism for forgetting (repression) is unnecessary.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) and the Eleventh revision of the International Classification of Diseases (ICD-11) do not use the concept of repression but that of dissociative amnesia. Dissociative amnesia is the forgetfulness due to psychological causes, including stress, of certain autobiographical events, which can cover short or long periods. The DSM-5 includes dissociative amnesia as a disorder (a clinical syndrome) and also as a symptom (among others) of post-traumatic stress disorder.
In 1977 Florence Rush argued that Freud’s theory about the Oedipus complex was created to cover up real cases of sexual abuse committed by adults against children. According to this, Freud changed his initially posited seduction theory because he wanted to hide the reality of the traumas that his patients would have suffered. In 1984 Jeffrey Moussaieff Masson published The Assault on Truth, where, like Rush, he argues that Freud covered up the reality of sexual abuse.
Drawing on Rush and Masson, Susie Orbach argues that Freud replaced his theory of seduction and childhood sexual trauma with the theory of the Oedipus complex. Freud changed his views and decided that his patients’ memories of sexual abuse were actually imaginary, neurotic fantasies of unrealised events and Oedipal wishes. This change in Freudian theory was criticised by Sandor Ferenczi and John Bowlby among other mental health specialists.
Phil Mollon claims that Freud was ahead of his time and that the new findings on false memory syndrome confirm the claims Freud made a century ago about imaginary memories.
On the other hand, in addition to Elizabeth Loftus, several reputable modern psychologists and psychiatrists, including Ulric Neisser, Julia Shaw and Daniel Schacter agree that human memory is usually not true to the facts.
The book edited by Robert Belli True and False Recovered Memories. Toward a Reconciliation of the Debate (2012) tries to make a synthesis that takes into account the part of truth and reason that both parts have in the debate.
Involvement in Legal Cases
Loftus has testified in over 300 cases, and consulted on many more. Her legal cases include:
Robert Durst’s 2020 trial for murder: Loftus testified for the defence regarding the killing of Susan Berman.
Ghislaine Maxwell’s 2021 trial for sex-trafficking: Loftus testified for the defence during Maxwell’s trial regarding sex trafficking of under-age girls for Jeffrey Epstein. This was the first case where Loftus claimed that the potential for financial rewards could cause a human brain to create a false traumatic memory; when questioned about the basis of the theory by the jury, Loftus stated “I am not aware of any studies on that, but based on my research, it’s definitely plausible.”
Harvey Weinstein’s 2020 trial for rape and sexual assault: Loftus testified for the defence during Weinstein’s trial for sexual assault of two women.
Loftus has also been involved with the cases of Ted Bundy, O.J. Simpson, Rodney King, Oliver North, Martha Stewart, Lewis Libby, Michael Jackson, the Menéndez brothers and the Oklahoma City bombers.
Personal Life
From 1968 to 1991, Elizabeth was married to fellow psychologist Geoffrey Loftus.
Publications
Loftus has written or co-authored many journal articles and books, including the 1994 book titled The Myth of Repressed Memory.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Elizabeth_Loftus >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.










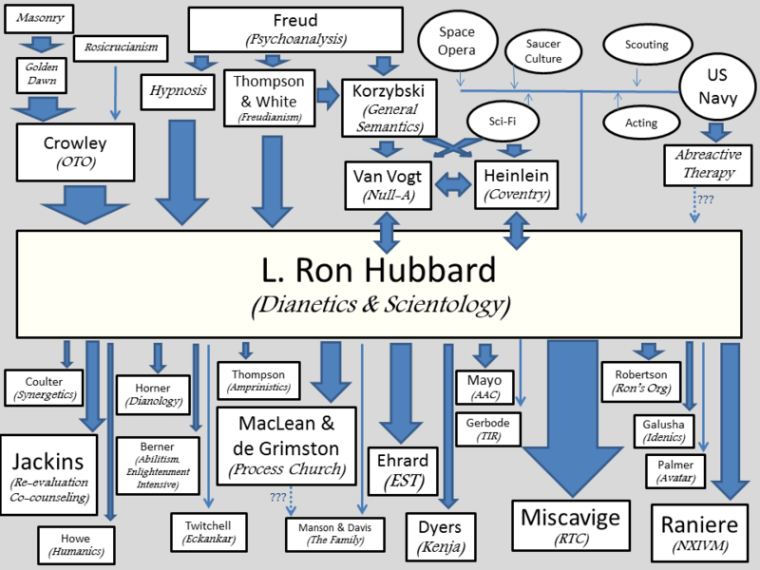

You must be logged in to post a comment.