Emotional reasoning is a cognitive process by which an individual concludes that their emotional reaction proves something is true, despite contrary empirical evidence. Emotional reasoning creates an ’emotional truth’, which may be in direct conflict with the inverse ‘perceptional truth’. It can create feelings of anxiety, fear, and apprehension in existing stressful situations, and as such, is often associated with or triggered by panic disorder or anxiety disorder. For example, even though a spouse has shown only devotion, a person using emotional reasoning might conclude, “I know my spouse is being unfaithful because I feel jealous.”
Plutchik Wheel
This process amplifies the effects of other cognitive distortions. For example, a student may feel insecure about their understanding of test material even though they are capable of answering the questions. If said student acts on their insecurity about failing the test, they might make the assumption that they misunderstand the material and therefore may guess answers randomly, causing their own failure in a self-fulfilling prophecy.
Emotional reasoning is related to other similar concepts, such as: motivated reasoning, a type of reasoning wherein individuals reach conclusions from bias instead of empirical motivations; emotional intelligence, which relates to the ways in which individuals use their emotions to understand situations or the information and reach conclusions; and cognitive distortion or cognitive deficiency, wherein individuals misinterpret situations or make decisions without considering a range of consequences.
Emotional reasoning, as a concept, was first introduced by psychiatrist Aaron Beck. It was included as a part of Beck’s broader research topic: cognitive distortions and depression. To counteract cognitive distortions, Beck developed a type of therapy formally known as cognitive therapy, which became associated with cognitive-behavioural therapy.
Emotional reasoning had been attributed to automatic thinking, but Beck believed that it stemmed from negative thoughts that were uncontrollable and happened without effort. This reasoning has been commonly accepted over the years. Most recently, a new explanation states that an “activating agent” or sensory trigger from the environment increases emotional arousal. With this increase in arousal, certain areas of the brain are inhibited. The combination of an increase in emotional arousal and the inhibition of parts of the brain leads to emotional reasoning.
Examples
The following are simple examples of emotional reasoning.
Emotion
Facts
False Conclusion
I feel jealous
My spouse is apparently faithful and loving.
My spouse is unfaithful, because I wouldn’t feel jealous if my spouse were faithful and loving.
I feel lonely
My friends and family seem to like me and normally treat me well.
I am unlovable, because I wouldn’t feel lonely if I were lovable.
I feel guilty
Neither I nor anyone around me is aware of any wrong I’ve done.
I did something wrong, because I wouldn’t feel guilty unless I had done something wrong.
I feel angry at her
I can’t think of anything upsetting she did or any harm she caused me.
She did something wrong, because I wouldn’t feel angry at her unless she had done something wrong.
I feel stupid
My academic and professional success is typical or better.
I am stupid, because I wouldn’t feel stupid or doubt my proven abilities unless I really was stupid.
Treatment
Before seeking professional help, an individual can influence the effect that emotional reasoning has on them based on his or her coping method. Using a proactive, problem-focused coping style is more effective at reducing stress and deterring stressful events. Additionally, having good social support also leads to lower psychological stress. If an individual chooses to seek professional help, a psychologist will often use cognitive-behavioural therapy to teach the patient how to challenge their cognitive distortions, including emotional reasoning. In this approach, the automatic thoughts that control emotional reasoning are identified, studied, and reasoned through by the patient. In doing so, the psychologist hopes to change the automatic thoughts of the patient and reduce the patient’s stress levels. Cognitive behavioural therapy has been generally regarded as the most-effective method of treatment for emotional reasoning.
Most recently, a new therapeutic approach uses the RIGAAR method to reduce emotional stress. RIGAAR is an abbreviation for: rapport building, information gathering, goal setting, accessing resources, agreeing strategies and rehearsing success.
Reducing emotional arousal is also suggested by the human givens approach in order to counter emotional reasoning. High emotional arousal inhibits brain regions necessary for logical complex reasoning. With less emotional arousal, cognitive reasoning is less affected and it is easier for the subject to disassociate reality from emotions.
Factors
Cognitive schemas is one of the factors to cause emotional reasoning. Schema is made of how we look at this world and our real-life experiences. Schema helps us remember the important things or events that happened in our lives. The result of the learning process is the schema, and it is also made by classical and operant conditioning. For example, an individual can develop a schema about terrorists and spiders that are very dangerous. Based on their schema, people can change what they think or how they are biased about the way they perceive things. Information-processing biases of schema impact how a person thinks and remembers, and their understanding of experiences and information. The bias makes a person’s schema automatically access similar content of schema. For example, a person with rat phobia is more likely to visualise or perceive a rat being near them. Schemas also easily connect with schema-central stimuli. For example, when depressed people start to think about negative things, it can be very difficult for them to think of anything positive.
For memory bias, schema can affect an individual’s recollections to cause schema-incongruent memories. For example, if individuals have a schema about how intelligent they are, failure-related recollections have a high chance to be retained in their minds and they become likely to recall positive past events. The schema also make individuals biased through the way that they interpret information. In other words, schema alters their understanding of the information. For example, when people refuse to help low self-esteem children solve a math problem, the children may think they are too stupid to learn how to solve the problem rather than the other people being too busy to help.
Reduction Techniques
Techniques for reducing emotional reasoning include:
Validity testing: Patients defend their thoughts and ideas using objective evidence to support their assumptions. If they cannot, they might be exposed to emotional reasoning.
Cognitive reversal: Patients are told of a difficult situation that they had in the past, and work with a therapist to help them address and correct their problems. This can prepare the patient for similar situations so that they do not revert to emotional reasoning.
Guided discovery: The therapist asks the patients a series of questions designed to help them realise their cognition distortions.
Writing in a journal: Patients form a habit of writing in a journal to record the situations they face, emotions and thoughts they experience, and their responses or behaviours to them. The therapist and patient then analyse how the patient’s maladaptive thought patterns influence their behaviours.
Homework: Once the patient acquires the ability to perform self-recovery and remember the insights gained from therapy sessions, the patient is tasked with reviewing sessions and reading related books to focus their thoughts and behaviours, which are recorded and reviewed for the next therapy session.
Modelling: The therapist could use role-playing to act in different ways in response to imagined situations so that patients could understand and model their behaviour.
Systematic positive reinforcement: The behaviour-oriented therapist would use a reward system (systematic positive reinforcement) to motivate patients to reinforce specific behaviours.
Negative memories and stressful life circumstances have a chance to trigger depression. The main factor for causing depression is unresolved life experiences. People who experience emotional reasoning are more likely to connect to depression. Emotion-focused therapy (EFT) is a form of psychotherapy which can help people find a positive perspective of their emotional process. EFT is a research-based treatment that emphasizes emotional change, which is the goal of this therapy. EFT has two different alternative therapies for treatments: cognitive-behavioural therapy (CBT), which emphasizes changing self-defeating thoughts and behaviours; and interpersonal therapy (IPT), which emphasizes changing people’s skills to have better interaction with others.
EFT operates on the understanding that a person’s development is influenced by emotional memories and experiences. The purpose of the therapy is to change the emotional process by resurfacing painful emotional experiences and bringing them into awareness. This process helps patients to differentiate between what they experience and the influence of past experiences on how they feel. This can result in greater self-awareness of what they want in their life and enable better decision-making through reducing emotional reasoning. Another purpose of EFT is to promote emotional intelligence, which is the ability to understand their emotions and perceive emotional information, controlling their behaviour while responding to problems.
Emotion-focused coping is a way to focus on managing one’s emotions to reduce stress and also to reduce the chance to have emotional reasoning. Cognitive therapy is a form of therapy that helps patients recognise their negative thought patterns about themselves and events to revise these thought patterns and change their behaviour. Cognitive-behavioural therapy helps individuals to perform well at cognitive tasks and to help them rethink their situation in a way that can benefit them. The treatment of cognitive-behavioural therapy is through the process of learning and making the change for maladaptive emotions, thoughts, and behaviours.
Implications
If not treated, debilitating effects can occur, the most common being depression. However, emotional reasoning has the potential to be useful when appraising the outside world and not ourselves. How one feels when assessing an object, person or event, can be an instinctual survival response and a way to adapt to the world.
“The amygdala buried deep in the limbic system serves as an early warning device for novelty, precisely so that attention can be mobilized to alert the mind to potential danger and to prepare for a potential of flight or fight.”
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Emotional_reasoning >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Emotional contagion is a form of social contagion that involves the spontaneous spread of emotions and related behaviours. Such emotional convergence can happen from one person to another, or in a larger group. Emotions can be shared across individuals in many ways, both implicitly or explicitly. For instance, conscious reasoning, analysis, and imagination have all been found to contribute to the phenomenon. The behaviour has been found in humans, other primates, dogs, and chickens.
Plutchik Wheel
Emotional contagion is important to personal relationships because it fosters emotional synchrony between individuals. A broader definition of the phenomenon suggested by Schoenewolf is:
“a process in which a person or group influences the emotions or behavior of another person or group through the conscious or unconscious induction of emotion states and behavioral attitudes.”
One view developed by Elaine Hatfield, et al., is that this can be done through automatic mimicry and synchronisation of one’s expressions, vocalisations, postures, and movements with those of another person. When people unconsciously mirror their companions’ expressions of emotion, they come to feel reflections of those companions’ emotions.
In a 1993 paper, Psychologists Elaine Hatfield, John Cacioppo, and Richard Rapson define emotional contagion as “the tendency to automatically mimic and synchronize expressions, vocalizations, postures, and movements with those of another person’s [sic] and, consequently, to converge emotionally”.
Hatfield, et al., theorise emotional contagion as a two-step process: First, we imitate people (e.g. if someone smiles at you, you smile back). Second, our own emotional experiences change based on the non-verbal signals of emotion that we give off. For example, smiling makes one feel happier, and frowning makes one feel worse. Mimicry seems to be one foundation of emotional movement between people.
Emotional contagion and empathy share similar characteristics, with the exception of the ability to differentiate between personal and pre-personal experiences, a process known as individuation. In The Art of Loving (1956), social psychologist Erich Fromm explores these differences, suggesting that autonomy is necessary for empathy, which is not found in emotional contagion.
Etymology
James Baldwin addressed “emotional contagion” in his 1897 work Social and Ethical Interpretations in Mental Development, though using the term “contagion of feeling”. Various 20th century scholars discussed the phenomena under the heading “social contagion”. The term “emotional contagion” first appeared in Arthur S. Reber’s 1985 The Penguin Dictionary of Psychology.
Influencing Factors
Several factors determine the rate and extent of emotional convergence in a group, including membership stability, mood-regulation norms, task interdependence, and social interdependence. Besides these event-structure properties, there are personal properties of the group’s members, such as openness to receive and transmit feelings, demographic characteristics, and dispositional affect that influence the intensity of emotional contagion.
Research
Research on emotional contagion has been conducted from a variety of perspectives, including organisational, social, familial, developmental, and neurological. While early research suggested that conscious reasoning, analysis, and imagination accounted for emotional contagion, some forms of more primitive emotional contagion are far more subtle, automatic, and universal.
Hatfield, Cacioppo, and Rapson’s 1993 research into emotional contagion reported that people’s conscious assessments of others’ feelings were heavily influenced by what others said. People’s own emotions, however, were more influenced by others’ nonverbal clues as to what they were really feeling. Recognizing emotions and acknowledging their origin can be one way to avoid emotional contagion. Transference of emotions has been studied in a variety of situations and settings, with social and physiological causes being two of the largest areas of research.
In addition to the social contexts discussed above, emotional contagion has been studied within organisations. Schrock, Leaf, and Rohr (2008) say organizations, like societies, have emotion cultures that consist of languages, rituals, and meaning systems, including rules about the feelings workers should, and should not, feel and display. They state that emotion culture is quite similar to “emotion climate”, otherwise known as morale, organisational morale, and corporate morale. Furthermore, Worline, Wrzesniewski, and Rafaeli (2002): 318 mention that organizations have an overall “emotional capability”, while McColl-Kennedy, and Smith (2006) examine “emotional contagion” in customer interactions. These terms arguably all attempt to describe a similar phenomenon; each term differs in subtle and somewhat indistinguishable ways.
Controversy
A controversial experiment demonstrating emotional contagion by using the social media platform Facebook was carried out in 2014 on 689,000 users by filtering positive or negative emotional content from their news feeds. The experiment sparked uproar among people who felt the study violated personal privacy. The 2014 publication of a research paper resulting from this experiment, “Experimental evidence of massive-scale emotional contagion through social networks”, a collaboration between Facebook and Cornell University, is described by Tony D. Sampson, Stephen Maddison, and Darren Ellis (2018) as a “disquieting disclosure that corporate social media and Cornell academics were so readily engaged with unethical experiments of this kind.” Tony D. Sampson et al. criticise the notion that “academic researchers can be insulated from ethical guidelines on the protection for human research subjects because they are working with a social media business that has ‘no obligation to conform’ to the principle of ‘obtaining informed consent and allowing participants to opt out’.” A subsequent study confirmed the presence of emotional contagion on Twitter without manipulating users’ timelines.
Beyond the ethical concerns, some scholars criticised the methods and reporting of the Facebook findings. John Grohol, writing for Psych Central, argued that despite its title and claims of “emotional contagion,” this study did not look at emotions at all. Instead, its authors used an application (called “Linguistic Inquiry and Word Count” or LIWC 2007) that simply counted positive and negative words in order to infer users’ sentiments. A shortcoming of the LIWC tool is that it does not understand negations. Hence, the tweet “I am not happy” would be scored as positive: “Since the LIWC 2007 ignores these subtle realities of informal human communication, so do the researchers.” Grohol concluded that given these subtleties, the effect size of the findings are little more than a “statistical blip.”
Kramer et al. (2014) found a 0.07%—that’s not 7 percent, that’s 1/15th of one percent!!—decrease in negative words in people’s status updates when the number of negative posts on their Facebook news feed decreased. Do you know how many words you’d have to read or write before you’ve written one less negative word due to this effect? Probably thousands.
Types
Emotions can be shared and mimicked in many ways. Taken broadly, emotional contagion can be either: implicit, undertaken by the receiver through automatic or self-evaluating processes; or explicit, undertaken by the transmitter through a purposeful manipulation of emotional states, to achieve a desired result.
Implicit
Unlike cognitive contagion, emotional contagion is less conscious and more automatic. It relies mainly on non-verbal communication, although emotional contagion can and does occur via telecommunication. For example, people interacting through e-mails and chats are affected by the other’s emotions, without being able to perceive the non-verbal cues.
One view, proposed by Hatfield and colleagues, describes emotional contagion as a primitive, automatic, and unconscious behaviour that takes place through a series of steps. When a receiver is interacting with a sender, he perceives the emotional expressions of the sender. The receiver automatically mimics those emotional expressions. Through the process of afferent feedback, these new expressions are translated into feeling the emotions the sender feels, thus leading to emotional convergence.
Another view, emanating from social comparison theories, sees emotional contagion as demanding more cognitive effort and being more conscious. According to this view, people engage in social comparison to see if their emotional reaction is congruent with the persons around them. The recipient uses the emotion as a type of social information to understand how he or she should be feeling. People respond differently to positive and negative stimuli; negative events tend to elicit stronger and quicker emotional, behavioural, and cognitive responses than neutral or positive events. So unpleasant emotions are more likely to lead to mood contagion than are pleasant emotions. Another variable is the energy level at which the emotion is displayed. Higher energy draws more attention to it, so the same emotional valence (pleasant or unpleasant) expressed with high energy is likely to lead to more contagion than if expressed with low energy.
Explicit
Aside from the automatic infection of feelings described above, there are also times when others’ emotions are being manipulated by a person or a group in order to achieve something. This can be a result of intentional affective influence by a leader or team member. Suppose this person wants to convince the others of something, he may do so by sweeping them up in his enthusiasm. In such a case, his positive emotions are an act with the purpose of “contaminating” the others’ feelings. A different kind of intentional mood contagion would be, for instance, giving the group a reward or treat, in order to alleviate their feelings.
The discipline of organisational psychology researches aspects of emotional labour. This includes the need to manage emotions so that they are consistent with organisational or occupational display rules, regardless of whether they are discrepant with internal feelings. In regard to emotional contagion, in work settings that require a certain display of emotions, one finds oneself obligated to display, and consequently feel, these emotions. If superficial acting develops into deep acting, emotional contagion is the byproduct of intentional affective impression management.
In Workplaces and Organisations
Intra-Group
Many organisations and workplaces encourage teamwork. Studies conducted by organisational psychologists highlight the benefits of work teams. Emotions come into play and a group emotion is formed.
The group’s emotional state influences factors such as cohesiveness, morale, rapport, and the team’s performance. For this reason, organisations need to take into account the factors that shape the emotional state of the work-teams, in order to harness the beneficial sides and avoid the detrimental sides of the group’s emotion. Managers and team leaders should be cautious with their behaviour, since their emotional influence is greater than that of a “regular” team member: leaders are more emotionally “contagious” than others.
Employee/Customer
The interaction between service employees and customers affects both customers’ assessments of service quality and their relationship with the service provider. Positive affective displays in service interactions are positively associated with important customer outcomes, such as intention to return and to recommend the store to a friend. It is the interest of organisations that their customers be happy, since a happy customer is a satisfied one. Research has shown that the emotional state of the customer is directly influenced by the emotions displayed by the employee/service provider via emotional contagion. But this influence depends on authenticity of the employee’s emotional display, such that if the employee is only surface-acting, the contagion is poor, in which case the beneficial effects will not occur.
Neurological Basis
Vittorio Gallese posits that mirror neurons are responsible for intentional attunement in relation to others. Gallese and colleagues at the University of Parma found a class of neurons in the premotor cortex that discharge either when macaque monkeys execute goal-related hand movements or when they watch others doing the same action. One class of these neurons fires with action execution and observation, and with sound production of the same action. Research in humans shows an activation of the premotor cortex and parietal area of the brain for action perception and execution.
Gallese says humans understand emotions through a simulated shared body state. The observers’ neural activation enables a direct experiential understanding. “Unmediated resonance” is a similar theory by Goldman and Sripada (2004). Empathy can be a product of the functional mechanism in our brain that creates embodied simulation. The other we see or hear becomes the “other self” in our minds. Other researchers have shown that observing someone else’s emotions recruits brain regions involved in:
Experiencing similar emotions; and
Producing similar facial expressions.
This combination indicates that the observer activates:
A representation of the emotional feeling of the other individual which leads to emotional contagion; and
A motor representation of the observed facial expression that could lead to facial mimicry.
In the brain, understanding and sharing other individuals’ emotions would thus be a combination of emotional contagion and facial mimicry. Importantly, more empathic individuals experience more brain activation in emotional regions while witnessing the emotions of other individuals.
Amygdala
The amygdala is one part of the brain that underlies empathy and allows for emotional attunement and creates the pathway for emotional contagion. The basal areas including the brain stem form a tight loop of biological connectedness, re-creating in one person the physiological state of the other. Psychologist Howard Friedman thinks this is why some people can move and inspire others. The use of facial expressions, voices, gestures and body movements transmit emotions to an audience from a speaker.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Emotional_contagion >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Social emotions are emotions that depend upon the thoughts, feelings or actions of other people, “as experienced, recalled, anticipated or imagined at first hand”. Examples are embarrassment, guilt, shame, jealousy, envy, coolness, elevation, empathy, and pride. In contrast, basic emotions such as happiness and sadness only require the awareness of one’s own physical state. Therefore, the development of social emotions is tightly linked with the development of social cognition, the ability to imagine other people’s mental states, which generally develops in adolescence. Studies have found that children as young as 2 to 3 years of age can express emotions resembling guilt and remorse. However, while five-year-old children are able to imagine situations in which basic emotions would be felt, the ability to describe situations in which social emotions might be experienced does not appear until seven years of age.
People may not only share emotions with others, but may also experience similar physiological arousal to others if they feel a sense of social connectedness to the other person. A laboratory-based study by Cwir, Car, Walton, and Spencer (2011) showed that, when a participant felt a sense of social connectedness to a stranger (research confederate), the participant experienced similar emotional states and physiological responses to that of the stranger while observing the stranger perform a stressful task.
Social emotions are sometimes called moral emotions, because they play an important role in morality and moral decision making. In neuroeconomics, the role social emotions play in game theory and economic decision-making is just starting to be investigated.
Behavioural Neuroscience
After functional imaging—functional magnetic resonance imaging (fMRI) in particular—became popular roughly a decade ago, researchers have begun to study economic decision-making with this new technology. This allows researchers to investigate, on a neurological level, the role emotions play in decision-making.
Developmental Picture
The ability to describe situations in which a social emotion will be experienced emerges at around age 7, and, by adolescence, the experience of social emotion permeates everyday social exchange. Studies using fMRI have found that different brain regions are involved in different age groups when performing social-cognitive and social-emotional tasks. While brain areas such as medial prefrontal cortex (MPFC), superior temporal sulcus (STS), temporal poles (TP) and precuneus bordering with posterior cingulate cortex are activated in both adults and adolescents when they reason about intentionality of others, the medial PFC is more activated in adolescents and the right STS more in adults. Similar age effects were found with younger participants, such that, when participants perform tasks that involve theory of mind, increase in age is correlated with an increase in activation in the dorsal part of the MPFC and a decrease in the activity in the ventral part of the MPFC were observed.
Studies that compare adults with adolescents in their processing of basic and social emotions also suggest developmental shifts in brain areas being involved. Comparing with adolescents, the left temporal pole has a stronger activity in adults when they read stories that elicit social emotions. The temporal poles are thought to store abstract social knowledge. This suggests that adult might use social semantic knowledge more often when thinking about social-emotional situations than adolescents.
Neuroeconomics
To investigate the function of social emotions in economic behaviours, researchers are interested in the differences in brain regions involved when participants are playing with, or think that they are playing with, another person as opposed to a computer. A study with fMRI found that, for participants who tend to cooperate on two-person “trust and reciprocity” games, believing that they are playing with another participant activated the prefrontal cortex, while believing that they are playing with a computer did not. This difference was not seen with players who tend not to cooperate. The authors interpret this difference as theory of minds that co-operators employ to anticipate the opponents’ strategies. This is an example of the way social decision making differs from other forms of decision making.
In behavioural economics, a heavy criticism is that people do not always act in a fully rational way, as many economic models assume. For example, in the ultimatum game, two players are asked to divide a certain amount of money, say x. One player, called the proposer, decides ratio by which the money gets divided. The other player, called the responder, decides whether or not to accept this offer. If the responder accepts the offer, say, y amount of money, then the proposer gets x-y amount and the responder gets y. But if the responder refuses to accept the offer, both players get nothing. This game is widely studied in behavioural economics. According to the rational agent model, the most rational way for the proposer to act is to make y as small as possible, and the most rational way for the responder to act is to accept the offer, since little amount of money is better than no money. However, what these experiments tend to find is that the proposers tend to offer 40% of x, and offers below 20% would get rejected by the responders. Using fMRI scans, researchers found that social emotions elicited by the offers may play a role in explaining the result. When offers are unfair as opposed to fair, three regions of the brain are active: the dorsolateral prefrontal cortex (DLPFC), the anterior cingulate cortex (ACC), and the insula. The insula is an area active in registering body discomfort. It is activated when people feel, among other things, social exclusion. The authors interpret activity in the insula as the aversive reaction one feels when faced with unfairness, activity in the DLPFC as processing the future reward from keeping the money, and the ACC is an arbiter that weighs these two conflicting inputs to make a decision. Whether or not the offer gets rejected can be predicted (with a correlation of 0.45) by the level of the responder’s insula activity.
Neuroeconomics and social emotions are also tightly linked in the study of punishment. Research using PET scan has found that, when players punish other players, activity in the nucleus accumbens (part of the striatum), a region known for processing rewards derived from actions gets activated. It shows that we not only feel hurtful when we become victims of unfairness, but we also find it psychologically rewarding to punish the wrongdoer, even at a cost to our own utility.
Social or Moral Aspect
Some social emotions are also referred to as moral emotions because of the fundamental role they play in morality. For example, guilt is the discomfort and regret one feels over one’s wrongdoing. It is a social emotion, because it requires the perception that another person is being hurt by this act; and it also has implication in morality, such that the guilty actor, in virtue of feeling distressed and guilty, accepts responsibility for the wrongdoing, which might cause desire to make amends or punish the self.
Not all social emotions are moral emotions. Pride, for instance, is a social emotion which involves the perceived admiration of other people, but research on the role it plays in moral behaviours yields problematic results.
Empathic Response
Empathy is defined by Eisenberg and colleagues as an affective response that stems from the apprehension or comprehension of another’s emotional state or condition and is similar to what the other person is feeling or would be expected to feel. Guilt, which is a social emotion with strong moral implication, is also strongly correlated with empathic responsiveness; whereas shame, an emotion with less moral flavour, is negatively correlated with empathic responsiveness, when controlling for guilt.
Perceived controllability also plays an important role modulating people’s socio-emotional reactions and empathic responses. For example, participants who are asked to evaluate other people’s academic performances are more likely to assign punishments when the low performance is interpreted as low-effort, as opposed to low-ability. Stigmas also elicit more empathic response when they are perceived as uncontrollable (i.e. having a biological origin, such as having certain disease), as opposed to controllable (i.e. having a behavioural origin, such as obesity).
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Social_emotions >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Emotional labour is the process of managing feelings and expressions to fulfil the emotional requirements of a job. More specifically, workers are expected to regulate their personas during interactions with customers, co-workers, clients, and managers. This includes analysis and decision-making in terms of the expression of emotion, whether actually felt or not, as well as its opposite: the suppression of emotions that are felt but not expressed. This is done so as to produce a certain feeling in the customer or client that will allow the company or organisation to succeed.
Plutchik WheelPlutchik Dyads
Roles that have been identified as requiring emotional labour include those involved in education, public administration, law, childcare, health care, social work, hospitality, media, advocacy, aviation and espionage. As particular economies move from a manufacturing to a service-based economy, more workers in a variety of occupational fields are expected to manage their emotions according to employer demands when compared to sixty years ago.
Definition
The sociologist Arlie Hochschild provided the first definition of emotional labour, which is displaying certain emotions to meet the requirements of a job. The related term emotion work (also called “emotion management”) refers to displaying certain emotions for personal purposes, such as within the private sphere of one’s home or interactions with family and friends. Hochschild identified three emotion regulation strategies: cognitive, bodily, and expressive. Within cognitive emotion work, one attempts to change images, ideas, or thoughts in hopes of changing the feelings associated with them. For example, one may associate a family picture with feeling happy and think about said picture whenever attempting to feel happy. Within bodily emotion work, one attempts to change physical symptoms in order to create a desired emotion. For example, one may attempt deep breathing in order to reduce anger. Within expressive emotion work, one attempts to change expressive gestures to change inner feelings, such as smiling when trying to feel happy.
While emotion work happens within the private sphere, emotional labour is emotion management within the workplace according to employer expectations. Jobs involving emotional labour are defined as those that:
Require face-to-face or voice-to-voice contact with the public.
Require the worker to produce an emotional state in another person.
Allow the employer, through training and supervision, to exercise a degree of control over the emotional activities of employees.
Hochschild (1983) argues that within this commodification process, service workers are estranged from their own feelings in the workplace.
Alternative Usage
The term has been applied in modern contexts to refer to household tasks, specifically unpaid labour that is often expected of women, e.g. having to remind their partner of chores. The term can also refer to informal counselling, such as providing advice to a friend or helping someone through a breakup. When Hochschild was interviewed about this shifting usage, she described it having undergone concept creep, expressing that it made the concept blurrier and was sometimes being applied to things that were simply just labour, although how carrying out this labour made a person feel could make it emotional labour as well.
Determinants
Societal, occupational, and organizational norms. For example, empirical evidence indicates that in typically “busy” stores there is more legitimacy to express negative emotions than there is in typically “slow” stores, in which employees are expected to behave in accordance with the display rules. Hence, the emotional culture to which one belongs influences the employee’s commitment to those rules.
Dispositional traits and inner feeling on the job; such as employees’ emotional expressiveness, which refers to the capability to use facial expressions, voice, gestures, and body movements to transmit emotions; or employees’ level of career identity (the importance of the career role to self-identity), which allows them to express the organizationally-desired emotions more easily (because there is less discrepancy between expressed behaviour and emotional experience when engaged in their work).
Supervisory regulation of display rules; Supervisors are likely to be important definers of display rules at the job level, given their direct influence on workers’ beliefs about high-performance expectations. Moreover, supervisors’ impressions of the need to suppress negative emotions on the job influence the employees’ impressions of that display rule.
Surface and Deep Acting
Arlie Hochschild’s foundational text divided emotional labour into two components: surface acting and deep acting. Surface acting occurs when employees display the emotions required for a job without changing how they actually feel. Deep acting is an effortful process through which employees change their internal feelings to align with organisational expectations, producing more natural and genuine emotional displays. Although the underlying processes differ, the objective of both is typically to show positive emotions, which are presumed to impact the feelings of customers and bottom-line outcomes (e.g. sales, positive recommendations, and repeat business). However, research generally has shown surface acting is more harmful to employee health. Without a consideration of ethical values, the consequences of emotional work on employees can easily become negative. Business ethics can be used as a guide for employees on how to present feelings that are consistent with ethical values, and can show them how to regulate their feelings more easily and comfortably while working.
Careers
In the past, emotional labour demands and display rules were viewed as a characteristic of particular occupations, such as restaurant workers, cashiers, hospital workers, bill collectors, counsellors, secretaries, and nurses. However, display rules have been conceptualised not only as role requirements of particular occupational groups, but also as interpersonal job demands, which are shared by many kinds of occupations.
Teachers
Zhang et al. (2019) looked at teachers in China, using questionnaires the researchers asked about their teaching experience and their interaction with the children and their families. According to numerous studies, early childhood education is important to a child’s development, which can have an effect on the teachers emotional labour, along with their emotional labour having an effect on the children. A big focus in this study was the use of surface acting in early childhood teacher. Zhang et al. (2019) found that surface acting was used significantly less than deep and natural acting in kindergarten teachers, along with early childhood teacher are less likely to fake or suppress their feelings. They also found that more experienced teachers had higher levels of emotional labour, because they either have more skills to suppress their emotions, or they are less driven to use surface acting.
Bill Collectors
In 1991, Sutton did an in-depth qualitative study into bill collectors at a collection agency. He found that unlike the other jobs described here where employees need to act cheerful and concerned, bill collectors are selected and socialized to show irritation to most debtors. Specifically, the collection agency hired agents who seemed to be easily aroused. The newly hired agents were then trained on when and how to show varying emotions to different types of debtors. As they worked at the collection agency, they were closely monitored by their supervisors to make sure that they frequently conveyed urgency to debtors.
Bill collectors’ emotional labour consists of not letting angry and hostile debtors make them angry and to not feel guilty about pressuring friendly debtors for money. They coped with angry debtors by publicly showing their anger or making jokes when they got off the phone. They minimised the guilt they felt by staying emotionally detached from the debtors.
Childcare Workers
The skills involved in childcare are often viewed as innate to women, making the components of childcare invisible. However, a number of scholars have not only studied the difficulty and skill required for childcare, but also suggested that the emotional labour of childcare is unique and needs to be studied differently. Performing emotional labour requires the development of emotional capital, and that can only be developed through experience and reflection. Through semi-structured interviews, Edwards (2016) found that there were two components of emotional labour in childcare in addition to Hochschild’s original two: emotional consonance and suppression. Edwards (2016) defined suppression as hiding emotion and emotional consonance as naturally experiencing the same emotion that one is expected to feel for the job.
Food-Industry Workers
Wait Staff
In her 1991 study of waitresses in Philadelphia, Paules examines how these workers assert control and protect their self identity during interactions with customers. In restaurant work, Paules argues, workers’ subordination to customers is reinforced through “cultural symbols that originate from deeply rooted assumptions about service work.” Because the waitresses were not strictly regulated by their employers, waitresses’ interactions with customers were controlled by the waitresses themselves. Although they are stigmatised by the stereotypes and assumptions of servitude surrounding restaurant work, the waitresses studied were not negatively affected by their interactions with customers. To the contrary, they viewed their ability to manage their emotions as a valuable skill that could be used to gain control over customers. Thus, the Philadelphia waitresses took advantage of the lack of employer-regulated emotional labour in order to avoid the potentially negative consequences of emotional labour.
Though Paules highlights the positive consequences of emotional labour for a specific population of waitresses, other scholars have also found negative consequences of emotional labour within the waitressing industry. Through eighteen months of participant observation research, Bayard De Volo (2003) found that casino waitresses are highly monitored and monetarily bribed to perform emotional labour in the workplace. Specifically, Bayard De Volo (2003) argues that through a sexualised environment and a generous tipping system, both casino owners and customers control waitresses’ behaviour and appearance for their own benefit and pleasure. Even though the waitresses have their own forms of individual and collective resistance mechanisms, intense and consistent monitoring of their actions by casino management makes it difficult to change the power dynamics of the casino workplace.
Fast-Food Employees
By using participant observation and interviews, Leidner (1993) examines how employers in fast food restaurants regulate workers’ interactions with customers. According to Leidner (1993), employers attempt to regulate workers’ interactions with customers only under certain conditions. Specifically, when employers attempt to regulate worker–customer interactions, employers believe that “the quality of the interaction is important to the success of the enterprise”, that workers are “unable or unwilling to conduct the interactions appropriately on their own”, and that the “tasks themselves are not too complex or context-dependent.” According to Leidner (1993), regulating employee interactions with customers involves standardizing workers’ personal interactions with customers. At the McDonald’s fast food restaurants in Leidner’s (1993) study, these interactions are strictly scripted, and workers’ compliance with the scripts and regulations are closely monitored.
Along with examining employers’ attempts to regulate employee–customer interactions, Leidner (1993) examines how fast-food workers’ respond to these regulations. According to Leidner (1993), meeting employers’ expectations requires workers to engage in some form of emotional labour. For example, McDonald’s workers are expected to greet customers with a smile and friendly attitude independent of their own mood or temperament at the time. Leidner (1993) suggests that rigid compliance with these expectations is at least potentially damaging to workers’ sense of self and identity. However, Leidner (1993) did not see the negative consequences of emotional labour in the workers she studied. Instead, McDonald’s workers attempted to individualise their responses to customers in small ways. Specifically, they used humour or exaggeration to demonstrate their rebellion against the strict regulation of their employee–customer interactions.
Physicians
According to Larson and Yao (2005), empathy should characterize physicians’ interactions with their patients because, despite advancement in medical technology, the interpersonal relationship between physicians and patients remains essential to quality healthcare. Larson and Yao (2005) argue that physicians consider empathy a form of emotional labour. Specifically, according to Larson and Yao (2005), physicians engage in emotional labour through deep acting by feeling sincere empathy before, during, and after interactions with patients. On the other hand, Larson and Yao (2005) argue that physicians engage in surface acting when they fake empathic behaviours toward the patient. Although Larson and Yao (2005) argue that deep acting is preferred, physicians may rely on surface acting when sincere empathy for patients is impossible. Overall, Larson and Yao (2005) argue that physicians are more effective and enjoy more professional satisfaction when they engage in empathy through deep acting due to emotional labour.
Police Work
According to Martin (1999), police work involves substantial amounts of emotional labour by officers, who must control their own facial and bodily displays of emotion in the presence of other officers and citizens. Although policing is often viewed as stereotypically masculine work that focuses on fighting crime, policing also requires officers to maintain order and provide a variety of interpersonal services. For example, police must have a commanding presence that allows them to act decisively and maintain control in unpredictable situations while having the ability to actively listen and talk to citizens. According to Martin (1999), a police officer who displays too much anger, sympathy, or other emotion while dealing with danger on the job will be viewed by other officers as someone unable to withstand the pressures of police work, due to the sexist views of many police officers. While being able to balance this self-management of emotions in front of other officers, police must also assertively restore order and use effective interpersonal skills to gain citizen trust and compliance. Ultimately, the ability of police officers to effectively engage in emotional labour affects how other officers and citizens view them.
Public Administration
Many scholars argue that the amount of emotional work required between all levels of government is greatest on the local level. It is at the level of cities and counties that the responsibility lies for day to day emergency preparedness, firefighters, law enforcement, public education, public health, and family and children’s services. Citizens in a community expect the same level of satisfaction from their government, as they receive in a customer service-oriented job. This takes a considerate amount of work for both employees and employers in the field of public administration. Mastracci and Adams (2017) looks at public servants and how they may be at risk of being alienated because of their unsupported emotional labour demands from their jobs. This can cause surface acting and distrust in management. There are two comparisons that represent emotional labour within public administration, “Rational Work versus Emotion Work”, and “Emotional Labour versus Emotional Intelligence.”
Performance
Many scholars argue that when public administrators perform emotional labour, they are dealing with significantly more sensitive situations than employees in the service industry. The reason for this is because they are on the front lines of the government, and are expected by citizens to serve them quickly and efficiently. When confronted by a citizen or a co-worker, public administrators use emotional sensing to size up the emotional state of the citizen in need. Workers then take stock of their own emotional state in order to make sure that the emotion they are expressing is appropriate to their roles. Simultaneously, they have to determine how to act in order to elicit the desired response from the citizen as well as from co-workers. Public Administrators perform emotional labour through five different strategies: Psychological First Aid, Compartments and Closets, Crazy Calm, Humour, and Common Sense.
Definition: Rational Work vs. Emotion Work
According to Mary Guy, Public administration does not only focus on the business side of administration but on the personal side as well. It is not just about collecting the water bill or land ordinances to construct a new property, it is also about the quality of life and sense of community that is allotted to individuals by their city officials. Rational work is the ability to think cognitively and analytically, while emotional work means to think more practically and with more reason.
Definition: Intelligence vs. Emotional Intelligence
Knowing how to suppress and manage one’s own feelings is known as emotional intelligence. The ability to control one’s emotions and to be able to do this at a high level guarantees one’s own ability to serve those in need. Emotional intelligence is performed while performing emotional labour, and without one the other can not be there.
Sex Work
Emotional labour is an essential part of many service jobs, including many types of sex work. Through emotional labour sex workers engage in different levels of acting known as surface acting and deep acting. These levels reflect a sex worker’s engagement with the emotional labour. Surface acting occurs when the sex worker is aware of the dissonance between their authentic experience of emotion and their managed emotional display. In contrast deep acting occurs when the sex worker can no longer differentiate between what is authentic and what is acting; acting becomes authentic.
Sex workers engage in emotional labour for many different reasons. First, sex workers often engage in emotional labour to construct performances of gender and sexuality. These performances frequently reflect the desires of a clientele which is mostly composed of heterosexual men. In the majority of cases, clients value women who they perceive as normatively feminine. For women sex workers, achieving this perception necessitates a performance of gender and sexuality that involves deference to clients and affirmation of their masculinity, as well as physical embodiment of traditional femininity. The emotional labour involved in sex work may be of a greater significance when race differences are involved. For instance Mistress Velvet, a black, femme dominatrix, advertises herself using her most fetishised attributes. She makes her clients, who are mostly white heterosexual men, read Black feminist theory before their sessions. This allows the clients to see why their participation, as white heterosexual men, contributes to the fetishization of black women.
Both within sex work and in other types of work, emotional labour is gendered in that women are expected to use it to construct performances of normative femininity, whereas men are expected to use it to construct performances of normative masculinity. In both cases, these expectations are often met because this labour is necessary to maximising monetary gain and potentially to job retention. Indeed, emotional labour is often used as a means to maximise income. It fosters a better experience for the client and protects the worker thus enabling the worker to make the most profit.
In addition, sex workers often engage in emotional labour as a self-protection strategy, distancing themselves from the sometimes emotionally volatile work. Finally, clients often value perceived authenticity in their transactions with sex workers; thus, sex workers may attempt to foster a sense of authentic intimacy.
Gender
Macdonald and Sirianni (1996) use the term “emotional proletariat” to describe service jobs in which “workers exercise emotional labor wherein they are required to display friendliness and deference to customers.” Because of deference, these occupations tend to be stereotyped as female jobs, independent of the actual number of women working the job. According to Macdonald and Sirianni (1996), because deference is a characteristic demanded of all those in disadvantaged structural positions, especially women, when deference is made a job requirement, women are likely to be overrepresented in these jobs. Macdonald and Sirianni (1996) claim that “[i]n no other area of wage labor are the personal characteristics of the workers so strongly associated with the nature of the work.” Thus, according to Macdonald and Sirianna (1996), although all workers employed within the service economy may have a difficult time maintaining their dignity and self-identity due to the demands of emotional labour, such an issue may be especially problematic for women workers.
Emotional labour also affects women by perpetuating occupational segregation and the gender wage gap. Job segregation, which is the systematic tendency for men and women to work in different occupations, is often cited as the reason why women lack equal pay when compared to men. According to Guy and Newman (2004), occupational segregation and ultimately the gender wage gap can at least be partially attributed to emotional labour. Specifically, work-related tasks that require emotional work thought to be natural for women, such as caring and empathizing are requirements of many female-dominated occupations. However, according to Guy and Newman (2004), these feminised work tasks are not a part of formal job descriptions and performance evaluations:
“Excluded from job descriptions and performance evaluations, the work is invisible and uncompensated. Public service relies heavily on such skills, yet civil service systems, which are designed on the assumptions of a bygone era, fail to acknowledge and compensate emotional labor.”
According to Guy and Newman (2004), women working in positions that require emotional labour in addition to regular work are not compensated for this additional labour because of the sexist notion that the additional labour is to be expected of them by the fact of being a woman. Guy and Azhar (2018) found that emotive expressions between sexes is affected by culture. This study found that there is variability to how women and men interpret emotive words, and specifically results showed that culture played a huge role in these gender differences.
Disability
People with disability are increasingly part of the labour force, due to societal attitudes about inclusion and neoliberal pressures around reducing welfare. Roles that require emotional labour may be more difficult for people with certain kinds of disabilities to perform. People with disabilities also may have to use more of their own time and energy to perform a task than a non-disabled person. For instance when they routinely encounter prejudice and stigma (as would be the case for many groups experiencing prejudice), including disability-unfriendly structures (Accessibility, administrative or social). On the other hand due to routine experience of navigating unhelpful structures and prejudice, disabled people can have dual advantages of: better skills in finding ways round problems without expending emotional energy being surprised for example, and easier sympathetic or empathetic understanding of other individuals and groups experiences with these problems. Inclusive or unfriendly organizational culture also has an impact, and workplaces may require workers with disability to downplay their impairments in order to ‘fit in’, an extra burden of emotional labour. Most individuals will experience complex affects of how their disability influences their emotional labour in a given job role at a specified organisation.
Implications
Positive affective display in service interactions, such as smiling and conveying friendliness, are positively associated with customer positive feelings, and important outcomes, such as intention to return, intention to recommend a store to others, and perception of overall service quality. There is evidence that emotional labour may lead to employees’ emotional exhaustion and burnout over time, and may also reduce employees’ job satisfaction. That is, higher degree of using emotion regulation on the job is related to higher levels of employees’ emotional exhaustion, and lower levels of employees’ job satisfaction.
There is empirical evidence that higher levels of emotional labour demands are not uniformly rewarded with higher wages. Rather, the reward is dependent on the level of general cognitive demands required by the job. That is, occupations with high cognitive demands evidence wage returns with increasing emotional labour demands; whereas occupations low in cognitive demands evidence a wage “penalty” with increasing emotional labour demands. Additionally, innovations that increase employee empowerment — such as conversion into worker cooperatives, co-managing schemes, or flattened workplace structures — have been found to increase workers’ levels of emotional labour as they take on more workplace responsibilities.
Coping Skills
Coping occurs in response to psychological stress—usually triggered by changes—in an effort to maintain mental health and emotional well-being. Life stressors are often described as negative events (loss of a job). However, positive changes in life (a new job) can also constitute life stressors, thus requiring the use of coping skills to adapt. Coping strategies are the behaviours, thoughts, and emotions that you use to adjust to the changes that occur in your life. The use of coping skills will help a person better themselves in the work place and perform to the best of their ability to achieve success. There are many ways to cope and adapt to changes. Some ways include: sharing emotions with peers, having a healthy social life outside of work, being humorous, and adjusting expectations of self and work. These coping skills will help turn negative emotion to positive and allow for more focus on the public in contrast to oneself.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Emotional_labor >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
The self-regulation of emotion or emotion regulation is the ability to respond to the ongoing demands of experience with the range of emotions in a manner that is socially tolerable and sufficiently flexible to permit spontaneous reactions as well as the ability to delay spontaneous reactions as needed. It can also be defined as extrinsic and intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions. The self-regulation of emotion belongs to the broader set of emotion regulation processes, which includes both the regulation of one’s own feelings and the regulation of other people’s feelings.
Plutchik WheelPlutchik Dyads
Emotion regulation is a complex process that involves initiating, inhibiting, or modulating one’s state or behaviour in a given situation — for example, the subjective experience (feelings), cognitive responses (thoughts), emotion-related physiological responses (for example heart rate or hormonal activity), and emotion-related behaviour (bodily actions or expressions). Functionally, emotion regulation can also refer to processes such as the tendency to focus one’s attention to a task and the ability to suppress inappropriate behaviour under instruction. Emotion regulation is a highly significant function in human life.
Every day, people are continually exposed to a wide variety of potentially arousing stimuli. Inappropriate, extreme or unchecked emotional reactions to such stimuli could impede functional fit within society; therefore, people must engage in some form of emotion regulation almost all of the time. Generally speaking, emotion dysregulation has been defined as difficulties in controlling the influence of emotional arousal on the organisation and quality of thoughts, actions, and interactions. Individuals who are emotionally dysregulated exhibit patterns of responding in which there is a mismatch between their goals, responses, and/or modes of expression, and the demands of the social environment. For example, there is a significant association between emotion dysregulation and symptoms of depression, anxiety, eating pathology, and substance abuse. Higher levels of emotion regulation are likely to be related to both high levels of social competence and the expression of socially appropriate emotions.
Theory
Process Model
The process model of emotion regulation is based upon the modal model of emotion. The modal model of emotion suggests that the emotion generation process occurs in a particular sequence over time. This sequence occurs as follows:
Situation: the sequence begins with a situation (real or imagined) that is emotionally relevant.
Attention: attention is directed towards the emotional situation.
Appraisal: the emotional situation is evaluated and interpreted.
Response: an emotional response is generated, giving rise to loosely coordinated changes in experiential, behavioural, and physiological response systems.
Because an emotional response (4.) can cause changes to a situation (1.), this model involves a feedback loop from (4.) Response to (1.) Situation. This feedback loop suggests that the emotion generation process can occur recursively, is ongoing, and dynamic.
The process model contends that each of these four points in the emotion generation process can be subjected to regulation. From this conceptualization, the process model posits five different families of emotion regulation that correspond to the regulation of a particular point in the emotion generation process. They occur in the following order:
Situation selection
Situation modification
Attentional deployment
Cognitive change
Response modulation
The process model also divides these emotion regulation strategies into two categories: antecedent-focused and response-focused. Antecedent-focused strategies (i.e. situation selection, situation modification, attentional deployment, and cognitive change) occur before an emotional response is fully generated. Response-focused strategies (i.e. response modulation) occur after an emotional response is fully generated.
Strategies
Situation Selection
Situation selection is an emotional regulation strategy that involves choosing to avoid or approach a future emotional situation. If a person selects to avoid or disengage from an emotionally relevant situation, they are decreasing the likelihood of experiencing an emotion. Alternatively, if a person selects to approach or engage with an emotionally relevant situation, they are increasing the likelihood of experiencing an emotion.
Typical examples of situation selection may be seen interpersonally, such as when a parent removes his or her child from an emotionally unpleasant situation. Use of situation selection may also be seen in psychopathology. For example, avoidance of social situations to regulate emotions is particularly pronounced for those with social anxiety disorder and avoidant personality disorder.
Effective situation selection is not always an easy task. For instance, humans display difficulties predicting their emotional responses to future events. Therefore, they may have trouble making accurate and appropriate decisions about which emotionally relevant situations to approach or to avoid.
Situation Modification
Situation modification involves efforts to modify a situation so as to change its emotional impact. Situation modification refers specifically to altering one’s external, physical environment. Altering one’s “internal” environment to regulate emotion is called cognitive change.
Examples of situation modification may include injecting humour into a speech to elicit laughter or extending the physical distance between oneself and another person.
Attentional Deployment
Attentional deployment involves directing one’s attention towards or away from an emotional situation.
Distraction
Distraction, an example of attentional deployment, is an early selection strategy, which involves diverting one’s attention away from an emotional stimulus and towards other content. Distraction has been shown to reduce the intensity of painful and emotional experiences, to decrease facial responding and neural activation in the amygdala associated with emotion, as well as to alleviate emotional distress. As opposed to reappraisal, individuals show a relative preference to engage in distraction when facing stimuli of high negative emotional intensity. This is because distraction easily filters out high-intensity emotional content, which would otherwise be relatively difficult to appraise and process.
Rumination
Rumination, an example of attentional deployment, is defined as the passive and repetitive focusing of one’s attention on one’s symptoms of distress and the causes and consequences of these symptoms. Rumination is generally considered a maladaptive emotion regulation strategy, as it tends to exacerbate emotional distress. It has also been implicated in a host of disorders including major depression.
Worry
Worry, an example of attentional deployment, involves directing attention to thoughts and images concerned with potentially negative events in the future. By focusing on these events, worrying serves to aid in the down-regulation of intense negative emotion and physiological activity. While worry may sometimes involve problem solving, incessant worry is generally considered maladaptive, being a common feature of anxiety disorders, particularly generalised anxiety disorder.
Thought Suppression
Thought suppression, an example of attentional deployment, involves efforts to redirect one’s attention from specific thoughts and mental images to other content so as to modify one’s emotional state. Although thought suppression may provide temporary relief from undesirable thoughts, it may ironically end up spurring the production of even more unwanted thoughts. This strategy is generally considered maladaptive, being most associated with obsessive-compulsive disorder.
Cognitive Change
Cognitive change involves changing how one appraises a situation so as to alter its emotional meaning.
Reappraisal
Reappraisal, an example of cognitive change, is a late selection strategy, which involves a change of the meaning of an event that alters its emotional impact. It encompasses different sub-strategies, such as positive reappraisal (creating and focusing on a positive aspect of the stimulus), decentring (reinterpreting an event by broadening one’s perspective to see “the bigger picture”), or fictional reappraisal (adopting or emphasizing the belief that event is not real, that it is for instance “just a movie” or “just my imagination”). Reappraisal has been shown to effectively reduce physiological, subjective, and neural emotional responding. As opposed to distraction, individuals show a relative preference to engage in reappraisal when facing stimuli of low negative emotional intensity because these stimuli are relatively easy to appraise and process.
Reappraisal is generally considered to be an adaptive emotion regulation strategy. Compared to suppression (including both thought suppression and expressive suppression), which is positively correlated with many psychological disorders, reappraisal can be associated with better interpersonal outcomes, and can be positively related to well-being. However, some researchers argue that context is important when evaluating the adaptiveness of a strategy, suggesting that in some contexts reappraisal may be maladaptive. Furthermore, some research has shown reappraisal does not influence or affect physiological responses to recurrent stress.
Distancing
Distancing, an example of cognitive change, involves taking on an independent, third-person perspective when evaluating an emotional event. Distancing has been shown to be an adaptive form of self-reflection, facilitating the emotional processing of negatively valenced stimuli, reducing emotional and cardiovascular reactivity to negative stimuli, and increasing problem-solving behaviour.
Humour
Humour, an example of cognitive change, has been shown to be an effective emotion regulation strategy. Specifically, positive, good-natured humour has been shown to effectively up-regulate positive emotion and down-regulate negative emotion. On the other hand, negative, mean-spirited humour is less effective in this regard.
Response Modulation
Response modulation involves attempts to directly influence experiential, behavioural, and physiological response systems.
Expressive Suppression
Expressive suppression, an example of response modulation, involves inhibiting emotional expressions. It has been shown to effectively reduce facial expressivity, subjective feelings of positive emotion, heart rate, and sympathetic activation. However, the research findings are mixed regarding whether this strategy is effective for down-regulating negative emotion. Research has also shown that expressive suppression may have negative social consequences, correlating with reduced personal connections and greater difficulties forming relationships.
Expressive suppression is generally considered to be a maladaptive emotion regulation strategy. Compared to reappraisal, it is positively correlated with many psychological disorders, associated with worse interpersonal outcomes, is negatively related to well-being, and requires the mobilisation of a relatively substantial amount of cognitive resources. However, some researchers argue that context is important when evaluating the adaptiveness of a strategy, suggesting that in some contexts suppression may be adaptive.
Drug Use
Drug use, an example of response modulation, can be used to alter emotion-associated physiological responses. For example, alcohol can produce sedative and anxiolytic effects and beta blockers can affect sympathetic activation.
Exercise
Exercise, an example of response modulation, can be used to down-regulate the physiological and experiential effects of negative emotions. Regular physical activity has also been shown to reduce emotional distress and improve emotional control.
Sleep
Sleep plays a role in emotion regulation, although stress and worry can also interfere with sleep. Studies have shown that sleep, specifically REM sleep, down-regulates reactivity of the amygdala, a brain structure known to be involved in the processing of emotions, in response to previous emotional experiences. On the flip side, sleep deprivation is associated with greater emotional reactivity or overreaction to negative and stressful stimuli. This is a result of both increased amygdala activity and a disconnect between the amygdala and the prefrontal cortex, which regulates the amygdala through inhibition, together resulting in an overactive emotional brain. Due to the subsequent lack of emotional control, sleep deprivation may be associated with depression, impulsivity, and mood swings. Additionally, there is some evidence that sleep deprivation may reduce emotional reactivity to positive stimuli and events and impair emotion recognition in others.
For example, a relevant mnemonic formulated in DBT is “ABC PLEASE”:
Accumulate positive experiences.
Build mastery by being active in activities that make one feel competent and effective to combat helplessness.
Cope ahead, preparing an action plan, researching, and rehearsing (with a skilled helper if necessary).
Physical illness treatment and prevention through check-ups.
Low vulnerability to diseases, managed with health care professionals.
Eating healthy.
Avoiding (non-prescribed) mood-altering drugs.
Sleep healthy.
Exercise regularly.
Developmental Process
Infancy
Intrinsic emotion regulation efforts during infancy are believed to be guided primarily by innate physiological response systems. These systems usually manifest as an approach towards and an avoidance of pleasant or unpleasant stimuli. At three months, infants can engage in self-soothing behaviours like sucking and can reflexively respond to and signal feelings of distress. For instance, infants have been observed attempting to suppress anger or sadness by knitting their brow or compressing their lips.
Between three and six months, basic motor functioning and attentional mechanisms begin to play a role in emotion regulation, allowing infants to more effectively approach or avoid emotionally relevant situations. Infants may also engage in self-distraction and help-seeking behaviours for regulatory purposes. At one year, infants are able to navigate their surroundings more actively and respond to emotional stimuli with greater flexibility due to improved motor skills. They also begin to appreciate their caregivers’ abilities to provide them regulatory support. For instance, infants generally have difficulties regulating fear. As a result, they often find ways to express fear in ways that attract the comfort and attention of caregivers.
Extrinsic emotion regulation efforts by caregivers, including situation selection, modification, and distraction, are particularly important for infants. The emotion regulation strategies employed by caregivers to attenuate distress or to up-regulate positive affect in infants can impact the infants’ emotional and behavioural development, teaching them particular strategies and methods of regulation. The type of attachment style between caregiver and infant can therefore play a meaningful role in the regulatory strategies infants may learn to use.
Recent evidence supports the idea that maternal singing has a positive effect on affect regulation in infants. Singing play-songs can have a visible affect-regulatory consequence of prolonged positive affect and even alleviation of distress. In addition to proven facilitation of social bonding, when combined with movement and/or rhythmic touch, maternal singing for affect regulation has possible applications for infants in the NICU and for adult caregivers with serious personality or adjustment difficulties.
Toddler-hood
By the end of the first year, toddlers begin to adopt new strategies to decrease negative arousal. These strategies can include rocking themselves, chewing on objects, or moving away from things that upset them. At two years, toddlers become more capable of actively employing emotion regulation strategies. They can apply certain emotion regulation tactics to influence various emotional states. Additionally, maturation of brain functioning and language and motor skills permits toddlers to manage their emotional responses and levels of arousal more effectively.
Extrinsic emotion regulation remains important to emotional development in toddlerhood. Toddlers can learn ways from their caregivers to control their emotions and behaviours. For example, caregivers help teach self-regulation methods by distracting children from unpleasant events (like a vaccination shot) or helping them understand frightening events.
Childhood
Emotion regulation knowledge becomes more substantial during childhood. For example, children aged six to ten begin to understand display rules. They come to appreciate the contexts in which certain emotional expressions are socially most appropriate and therefore ought to be regulated. For example, children may understand that upon receiving a gift they should display a smile, irrespective of their actual feelings about the gift. During childhood, there is also a trend towards the use of more cognitive emotion regulation strategies, taking the place of more basic distraction, approach, and avoidance tactics.
Regarding the development of emotion dysregulation in children, one robust finding suggests that children who are frequently exposed to negative emotion at home will be more likely to display, and have difficulties regulating, high levels of negative emotion.
Adolescence
Adolescents show a marked increase in their capacities to regulate their emotions, and emotion regulation decision making becomes more complex, depending on multiple factors. In particular, the significance of interpersonal outcomes increases for adolescents. When regulating their emotions, adolescents are therefore likely to take into account their social context. For instance, adolescents show a tendency to display more emotion if they expect a sympathetic response from their peers.
Additionally, spontaneous use of cognitive emotion regulation strategies increases during adolescence, which is evidenced both by self-report data and neural markers.
Adulthood
Social losses increase and health tends to decrease as people age. As people get older their motivation to seek emotional meaning in life through social ties tends to increase. Autonomic responsiveness decreases with age, and emotion regulation skill tends to increase.
Emotional regulation in adulthood can also be examined in terms of positive and negative affectivity. Positive and negative affectivity refers to the types of emotions felt by an individual as well as the way those emotions are expressed. With adulthood comes an increased ability to maintain both high positive affectivity and low negative affectivity “more rapidly than adolescents.” This response to life’s challenges seems to become “automatized” as people progress throughout adulthood. Thus, as individuals age, their capability of self-regulating emotions and responding to their emotions in healthy ways improves.
Additionally, emotional regulation may vary between young adults and older adults. Younger adults have been found to be more successful than older adults in practicing “cognitive reappraisal” to decrease negative internal emotions. On the other hand, older adults have been found to be more successful in the following emotional regulation areas:
Predicting the level of “emotional arousal” in possible situations;
Having a higher focus on positive information rather than negative; and
Maintaining healthy levels of “hedonic well-being” (subjective well-being based on increased pleasure and decreased pain).
Overview of Perspectives
Neuropsychological Perspective
Affective
As people age, their affect – the way they react to emotions – changes, either positively or negatively. Studies show that positive affect increases as a person grows from adolescence to their mid 70s. Negative affect, on the other hand, decreases until the mid 70s. Studies also show that emotions differ in adulthood, particularly affect (positive or negative). Although some studies found that individuals experience less affect as they grow older, other studies have concluded that adults in their middle age experience more positive affect and less negative affect than younger adults. Positive affect was also higher for men than women while the negative affect was higher for women than it was for men and also for single people.
A reason that older people – middle adulthood – might have less negative affect is because they have overcome, “the trials and vicissitudes of youth, they may increasingly experience a more pleasant balance of affect, at least up until their mid-70s”. Positive affect might rise during middle age but towards the later years of life – the 70s – it begins to decline while negative affect also does the same. This might be due to failing health, reaching the end of their lives and the death of friends and relatives.
In addition to baseline levels of positive and negative affect, studies have found individual differences in the time-course of emotional responses to stimuli. The temporal dynamics of emotion regulation, also known as affective chronometry, include two key variables in the emotional response process: rise time to peak emotional response, and recovery time to baseline levels of emotion. Studies of affective chronometry typically separate positive and negative affect into distinct categories, as previous research has shown (despite some correlation) the ability of humans to experience changes in these categories independently of one another. Affective chronometry research has been conducted on clinical populations with anxiety, mood, and personality disorders, but is also utilised as a measurement to test the effectiveness of different therapeutic techniques (including mindfulness training) on emotional dysregulation.
Neurological
The development of functional magnetic resonance imaging has allowed for the study of emotion regulation on a biological level. Specifically, research over the last decade strongly suggests that there is a neural basis. Sufficient evidence has correlated emotion regulation to particular patterns of prefrontal activation. These regions include the orbital prefrontal cortex, the ventromedial prefrontal cortex, and the dorsolateral prefrontal cortex. Two additional brain structures that have been found to contribute are the amygdala and the anterior cingulate cortex. Each of these structures are involved in various facets of emotion regulation and irregularities in one or more regions and/or interconnections among them are affiliated with failures of emotion regulation. An implication to these findings is that individual differences in prefrontal activation predict the ability to perform various tasks in aspects of emotion regulation.
Sociological
People intuitively mimic facial expressions; it is a fundamental part of healthy functioning. Similarities across cultures in regards to nonverbal communication has prompted the debate that it is in fact a universal language. It can be argued that emotion regulation plays a key role in the ability to generate the correct responses in social situations. Humans have control over facial expressions both consciously and unconsciously: an intrinsic emotion program is generated as the result of a transaction with the world, which immediately results in an emotional response and usually a facial reaction. It is a well documented phenomenon that emotions have an effect on facial expression, but recent research has provided evidence that the opposite may also be true.
This notion would give rise to the belief that a person may not only control his emotion but in fact influence them as well. Emotion regulation focuses on providing the appropriate emotion in the appropriate circumstances. Some theories allude to the thought that each emotion serves a specific purpose in coordinating organismic needs with environmental demands (Cole, 1994). This skill, although apparent throughout all nationalities, has been shown to vary in successful application at different age groups. In experiments done comparing younger and older adults to the same unpleasant stimuli, older adults were able to regulate their emotional reactions in a way that seemed to avoid negative confrontation. These findings support the theory that with time people develop a better ability to regulate their emotions. This ability found in adults seems to better allow individuals to react in what would be considered a more appropriate manner in some social situations, permitting them to avoid adverse situations that could be seen as detrimental.
Expressive Regulation (in Solitary Conditions)
In solitary conditions, emotion regulation can include a minimization-miniaturization effect, in which common outward expressive patterns are replaced with toned down versions of expression. Unlike other situations, in which physical expression (and its regulation) serve a social purpose (i.e. conforming to display rules or revealing emotion to outsiders), solitary conditions require no reason for emotions to be outwardly expressed (although intense levels of emotion can bring out noticeable expression anyway). The idea behind this is that as people get older, they learn that the purpose of outward expression (to appeal to other people), is not necessary in situations in which there is no one to appeal to. As a result, the level of emotional expression can be lower in these solitary situations.
Stress
The way an individual reacts to stress can directly overlap with their ability to regulate emotion. Although the two concepts differ in a multitude of ways, “both coping [with stress] and emotion regulation involve affect modulation and appraisal processes” that are necessary for healthy relationships and self-identity.
According to Yu. V. Shcherbatykh, emotional stress in situations like school examinations can be reduced by engaging in self-regulating activities prior to the task being performed. To study the influence of self-regulation on mental and physiological processes under exam stress, Shcherbatykh conducted a test with an experimental group of 28 students (of both sexes) and a control group of 102 students (also of both sexes).
In the moments before the examination, situational stress levels were raised in both groups from what they were in quiet states. In the experimental group, participants engaged in three self-regulating techniques (concentration on respiration, general body relaxation, and the creation of a mental image of successfully passing the examination). During the examination, the anxiety levels of the experimental group were lower than that of the control group. Also, the percent of unsatisfactory marks in the experimental group was 1.7 times less than in the control group. From this data, Shcherbatykh concluded that the application of self-regulating actions before examinations helps to significantly reduce levels of emotional strain, which can help lead to better performance results.
Emotion regulation has also been associated with physiological responses to stress during laboratory stress paradigms.
Decision Making
Identification of our emotional self-regulating process can facilitate in the decision-making process. Current literature on emotion regulation identifies that humans characteristically make efforts in controlling emotion experiences. There is then a possibility that our present state emotions can be altered by emotion regulation strategies resulting in the possibility that different regulation strategies could have different decision implications.
Digital Emotion Regulation
Following widespread adoption in the 21st century of digital devices and services for use in everyday life, evidence is mounting that people are increasingly using these tools to manage and regulate moods and emotions. A wide range of digital resources are used for emotion regulation including smartphones, social media, streaming services, online shopping, and videogames. Such spontaneous forms of digital emotion regulation can be distinguished from the use of digital interventions such as smartphone apps that have been explicitly designed to support emotional regulation or teach emotion regulation skills in clinical and non-clinical populations. Digital implementation of emotion regulation strategies can occur at all stages of the process model and in all strategy families, including interpersonal emotion regulation.
Effects of Low Self-Regulation
With a failure in emotion regulation, there is a rise in psychosocial and emotional dysfunctions caused by traumatic experiences due to an inability to regulate emotions. These traumatic experiences typically happen in grade school and are sometimes associated with bullying. Children who can not properly self-regulate express their volatile emotions in a variety of ways, including screaming if they do not have their way, lashing out with their fists, throwing objects (such as chairs), or bullying other children. Such behaviours often elicit negative reactions from the social environment, which, in turn, can exacerbate or maintain the original regulation problems over time, a process termed cumulative continuity. These children are more likely to have conflict-based relationships with their teachers and other children. This can lead to more severe problems such as an impaired ability to adjust to school and predicts school dropout many years later. Children who fail to properly self-regulate grow as teenagers with more emerging problems. Their peers begin to notice this “immaturity”, and these children are often excluded from social groups and teased and harassed by their peers. This “immaturity” certainly causes some teenagers to become social outcasts in their respective social groups, causing them to lash out in angry and potentially violent ways. Being teased or being an outcast in childhood is especially damaging because it could lead to psychological symptoms such as depression and anxiety (in which dysregulated emotions play a central role), which, in turn, could lead to more peer victimisation. This is why it is recommended to foster emotional self-regulation in children as early as possible.
Occupational Therapy in Schools
Occupational therapists (OTs) are integrated educators in most public and private schools across the United States. They are trained in mental health and activity analysis to assess the needs of their clients. OTs and students work together to create meaningful and healthy habits for stress management, social skills, emotional labelling, coping strategies, awareness, problem-solving, self-monitoring, judgement, emotional control, and others in the school and home environment. OTs can complete formal assessments for emotional regulation and treat in a client-centred manner for each student. In addition, they can create individualised home programmes for carryover with their families. For example, OTs can work with students to engage in the occupational therapist-developed curriculum The Zones of Regulation, which utilises evidence-based knowledge, formal assessment, and in-classroom treatment to improve self-regulation of emotional behaviours and create long-lasting changes in habits.
Early childhood access to education on emotional regulation mitigates risk factors for increased anxiety, depression, and negative behaviours. It allows the student to create healthy habits for school and home environments. Children should be able to learn to regulate their feelings for full participation in activities, including social skills, play, sports, and school.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Emotional_self-regulation >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
“Fake it till you make it” (or “Fake it until you make it”) is an aphorism that suggests that by imitating confidence, competence, and an optimistic mindset, a person can realise those qualities in their real life and achieve the results they seek.
The phrase is first attested some time before 1973. The earliest reference to a similar phrase occurs in the Simon & Garfunkel song “Fakin’ It”, released in 1968 as a single and also on their Bookends album. Simon sings, “And I know I’m fakin’ it, I’m not really makin’ it.”
Similar advice has been offered by a number of writers over time:
Action seems to follow feeling, but really action and feeling go together; and by regulating the action, which is under the more direct control of the will, we can indirectly regulate the feeling, which is not. Thus the sovereign voluntary path to cheerfulness, if our spontaneous cheerfulness be lost, is to sit up cheerfully, to look round cheerfully, and to act and speak as if cheerfulness were already there. If such conduct does not make you soon feel cheerful, nothing else on that occasion can. So to feel brave, act as if we were brave, use all our will to that end, and a courage-fit will very likely replace the fit of fear. ( William James, “The Gospel of Relaxation”, On Vital Reserves, 1922).
In the law of attraction movement, “act as if you already have it”, or simply “act as if”, is a central concept:
How do you get yourself to a point of believing? Start make-believing. Be like a child, and make-believe. Act as if you have it already. As you make-believe, you will begin to believe you have received. ( Rhonda Byrne, The Secret, 2006).
In Psychology
In the 1920s, Alfred Adler developed a therapeutic technique that he called “acting as if”, asserting that “if you want a quality, act as if you already have it”. This strategy gave his clients an opportunity to practice alternatives to dysfunctional behaviours. Adler’s method is still used today and is often described as role play.
“Faking it till you make it” is a psychological tool discussed in neuroscientific research. A 1988 experiment by Fritz Strack claimed to show that mood can be improved by holding a pen between the user’s teeth to force a smile, but a posterior experiment failed to replicate it, due to which Strack was awarded the Ig Nobel Prize for psychology in 2019. A later 2022 study about strategies to counter emotional distress found forced smiling not more effective than forced neutral expressions and other strategies of emotional regulation.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Fake_it_till_you_make_it >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Emotion work is understood as the art of trying to change in degree or quality an emotion or feeling.
Emotion work may be defined as the management of one’s own feelings, or work done in an effort to maintain a relationship; there is dispute as to whether emotion work is only work done regulating one’s own emotion, or extends to performing the emotional work for others.
Hochschild
Arlie Russell Hochschild, who introduced the term in 1979, distinguished emotion work – unpaid emotional work that a person undertakes in private life – from emotional labour: emotional work done in a paid work setting. Emotion work has use value and occurs in situations in which people choose to regulate their emotions for their own non-compensated benefit (e.g. in their interactions with family and friends). By contrast, emotional labour has exchange value because it is traded and performed for a wage.
In a later development, Hochschild distinguished between two broad types of emotion work, and among three techniques of emotion work. The two broad types involve evocation and suppression of emotion, while the three techniques of emotion work that Hochschild describes are cognitive, bodily and expressive.
However, the concept (if not the term) has been traced back as far as Aristotle: as Aristotle saw, the problem is not with emotionality, but with the appropriateness of emotion and its expression.
Examples
Examples of emotion work include showing affection, apologizing after an argument, bringing up problems that need to be addressed in an intimate relationship or any kind of interpersonal relationship, and making sure the household runs smoothly.
Emotion work also involves the orientation of self/others to accord with accepted norms of emotional expression: emotion work is often performed by family members and friends, who put pressure on individuals to conform to emotional norms. Arguably, then, an individual’s ultimate obeisance and/or resistance to aspects of emotion regimes are made visible in their emotion work.
Cultural norms often imply that emotion work is reserved for females. There is certainly evidence to the effect that the emotional management that women and men do is asymmetric; and that in general, women come into a marriage groomed for the role of emotional manager.
Criticism
The social theorist Victor Jeleniewski Seidler argues that women’s emotion work is merely another demonstration of false consciousness under patriarchy, and that emotion work, as a concept, has been adopted, adapted or criticised to such an extent that it is in danger of becoming a “catch-all-cliché”.
More broadly, the concept of emotion work has itself been criticised as a wide over-simplification of mental processes such as repression and denial which continually occur in everyday life.
Literary Analogues
Rousseau in The New Heloise suggests that the attempt to master instrumentally one’s affective life always results in a weakening and eventually the fragmentation of one’s identity, even if the emotion work is performed at the demand of ethical principles.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Emotion_work >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
An amygdala hijack is an emotional response that is immediate, overwhelming, and out of measure with the actual stimulus because it has triggered a much more significant emotional threat.
The term, coined by Daniel Goleman in his 1996 book Emotional Intelligence: Why It Can Matter More Than IQ, is used by affective neuroscientists and is considered a formal academic term. The amygdala is made up of two small, round structures located closer to the forehead than (anterior to) the hippocampi, near the temporal lobes. The amygdalae are involved in detecting and learning which parts of our surroundings are important and have emotional significance. They are critical for the production of emotion. They are known to be very important for negative emotions, especially fear. Amygdala activation often happens when we see a potential threat. The amygdala uses our past, related memories to help us make decisions about what is currently happening.
Definition
The output of sense organs is first received by the thalamus. Part of the thalamus’ stimuli goes directly to the amygdala or “emotional/irrational brain”, while other parts are sent to the neocortex or “thinking/rational brain”. If the amygdala perceives a match to the stimulus, i.e. if the record of experiences in the hippocampus tells the amygdala that it is a fight, flight or freeze situation, then the amygdala triggers the HPA (hypothalmic–pituitary–adrenal) axis and “hijacks” or overtakes rational brain function.
This emotional brain activity processes information milliseconds earlier than the rational brain, so in case of a match, the amygdala acts before any possible direction from the neocortex can be received. If, however, the amygdala does not find any match to the stimulus received with its recorded threatening situations, then it acts according to the directions received from the neocortex. When the amygdala perceives a threat, it can lead that person to react irrationally and destructively.
Goleman states that emotions “make us pay attention right now—this is urgent—and gives us an immediate action plan without having to think twice. The emotional component evolved very early: Do I eat it, or does it eat me?” The emotional response “can take over the rest of the brain in a millisecond if threatened”. An amygdala hijack exhibits three signs: strong emotional reaction, sudden onset, and post-episode realization if the reaction was inappropriate.
Goleman later emphasized that “self-control is crucial … when facing someone who is in the throes of an amygdala hijack” so as to avoid a complementary hijacking—whether in work situations, or in private life. Thus for example “one key marital competence is for partners to learn to soothe their own distressed feelings … nothing gets resolved positively when husband or wife is in the midst of an emotional hijacking”. The danger is that:
“when our partner becomes, in effect, our enemy, we are in the grip of an ‘amygdala hijack’ in which our emotional memory, lodged in the limbic center of our brain, rules our reactions without the benefit of logic or reason … which causes our bodies to go into a ‘fight or flight’ response.”
Non-Distressing Hijack
Goleman points out that:
“not all limbic hijackings are distressing. When a joke strikes someone as so uproarious that their laughter is almost explosive, that, too, is a limbic response. It is at work also in moments of intense joy.”
He also cites the case of a man strolling by a canal when he saw a girl staring petrified at the water.
“[B]efore he knew quite why, he had jumped into the water—in his coat and tie. Only once he was in the water did he realize that the girl was staring in shock at a toddler who had fallen in—whom he was able to rescue.”
Emotional Relearning
Joseph E. LeDoux was positive about the possibility of learning to control the amygdala’s hair-trigger role in emotional outbursts.
“Once your emotional system learns something, it seems you never let it go. What therapy does is teach you how to control it—it teaches your neocortex how to inhibit your amygdala. The propensity to act is suppressed, while your basic emotion about it remains in a subdued form.”
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Amygdala_hijack >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Aversion to happiness, also called fear of happiness, is an attitude towards happiness in which individuals may deliberately avoid experiences that invoke positive emotions or happiness. Aversion to happiness is not a recognised mental health disorder on its own, but it can contribute to and/or exacerbate existing mental health issues.
Mohsen Joshanloo and Dan Weijers identify four reasons for an aversion to happiness:
A belief that happiness will cause bad things to happen
That happiness will cause you to become a bad person
That expressing happiness is somehow bad for you and others
That pursuing happiness is bad for you and others.
For example, “some people—in Western and Eastern cultures—are wary of happiness because they believe that bad things, such as unhappiness, suffering, and death, tend to happen to happy people.” Empirical studies show that fear of happiness is associated with fragility of happiness beliefs, suggesting that one of the causes of aversion to happiness may be the belief that happiness is unstable and fragile. Research shows that fear of happiness is associated with avoidant and anxious attachment styles. A study found that perfectionistic tendencies, loneliness, a childhood perceived as unhappy, belief in paranormal phenomena, and holding a collectivistic understanding of happiness are positively associated with aversion to happiness.
Cultural Factors
One of several reasons why fear of happiness may develop is the belief that when one becomes happy, a negative event will soon occur that will taint that happiness, as if punishing that individual for satisfaction. This belief is thought to be more prevalent in non-Western cultures. In Western cultures, such as American culture, “it is almost taken for granted that happiness is one of the most important values guiding people’s lives”. Western cultures are more driven by an urge to maximise happiness and to minimize sadness. Failing to appear happy often gives cause for concern. The value placed on happiness echoes through Western positive psychology and through research on subjective well-being.
These findings “call into question the notion that happiness is the ultimate goal, a belief echoed in any number of articles and self-help publications about whether certain choices are likely to make you happy”. Also, “in cultures that believe worldly happiness to be associated with sin, shallowness, and moral decline will actually feel less satisfied when their lives are (by other standards) going well”, so measures of personal happiness cannot simply be considered a yardstick for satisfaction with one’s life, and attitudes such as aversion to happiness have important implications for measuring happiness across cultures and ranking nations on happiness scores.
Aversion to happiness can be thought of as a specific example of ideal affect (described by affect valuation theory), whereby cultures vary in the extent to which they value the experience of different emotions.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Aversion_to_happiness >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Emotional eating, also known as stress eating and emotional overeating, is defined as the “propensity to eat in response to positive and negative emotions”. While the term often refers to eating as a means of coping with negative emotions, it also includes eating for positive emotions, such as eating foods when celebrating an event or eating to enhance an already good mood. In these situations, emotions are still driving the eating but not in a negative way.
Background
Emotional eating includes eating in response to any emotion, whether that be positive or negative. Most frequently, people refer to emotional eating as “eating to cope with negative emotions.” In these situations, emotional eating can be considered a form of disordered eating, which is defined as “an increase in food intake in response to negative emotions” and can be considered a maladaptive strategy. More specifically, emotional eating in order to relieve negative emotions would qualify as a form of emotion-focused coping, which attempts to minimise, regulate, and prevent emotional distress.
One study found that emotional eating sometimes does not reduce emotional distress, but instead it enhances emotional distress by sparking feelings of intense guilt after an emotional eating session. Those who eat as a coping strategy are at an especially high risk of developing binge-eating disorder, and those with eating disorders are at a higher risk to engage in emotional eating as a means to cope. In a clinical setting, emotional eating can be assessed by the Dutch Eating Behaviour Questionnaire, which contains a scale for restrained, emotional, and external eating. Other questionnaires, such as the Palatable Eating Motives Scale, can determine reasons why a person eats tasty foods when they are not hungry; sub-scales include eating for reward enhancement, coping, social, and conformity.
Characteristics
Emotional eating usually occurs when one is attempting to satisfy his or her hedonic drive, or the drive to eat palatable food to obtain pleasure in the absence of an energy deficit but can also occur when one is seeking food as a reward, eating for social reasons (such as eating at a party), or eating to conform (which involves eating because friends or family wants the individual to). When one is engaging in emotional eating, they are usually seeking out palatable foods (such as sweets) rather than just food in general. In some cases, emotional eating can lead to something called “mindless eating” during which the individual is eating without being mindful of what or how much they are consuming; this can occur during both positive and negative settings.
Emotional hunger does not originate from the stomach, such as with a rumbling or growling stomach, but tends to start when a person thinks about a craving or wants something specific to eat. Emotional responses are also different. Giving in to a craving or eating because of stress can cause feelings of regret, shame, or guilt, and these responses tend to be associated with emotional hunger. On the other hand, satisfying a physical hunger is giving the body the nutrients or calories it needs to function and is not associated with negative feelings.
Major Theories behind Eating to Cope
Current research suggests that certain individual factors may increase one’s likelihood of using emotional eating as a coping strategy. The inadequate affect regulation theory posits that individuals engage in emotional eating because they believe overeating alleviates negative feelings. Escape theory builds upon inadequate affect regulation theory by suggesting that people not only overeat to cope with negative emotions, but they find that overeating diverts their attention away from a stimulus that is threatening self-esteem to focus on a pleasurable stimulus like food. Restraint theory suggests that overeating as a result of negative emotions occurs among individuals who already restrain their eating. While these individuals typically limit what they eat, when they are faced with negative emotions they cope by engaging in emotional eating. Restraint theory supports the idea that individuals with other eating disorders are more likely to engage in emotional eating. Together these three theories suggest that an individual’s aversion to negative emotions, particularly negative feelings that arise in response to a threat to the ego or intense self-awareness, increase the propensity for the individual to utilise emotional eating as a means of coping with this aversion.
The biological stress response may also contribute to the development of emotional eating tendencies. In a crisis, corticotropin-releasing hormone (CRH) is secreted by the hypothalamus, suppressing appetite and triggering the release of glucocorticoids from the adrenal gland. These steroid hormones increase appetite and, unlike CRH, remain in the bloodstream for a prolonged period of time, often resulting in hyperphagia. Those who experience this biologically instigated increase in appetite during times of stress are therefore primed to rely on emotional eating as a coping mechanism.
Contributing Factors
Negative Affect
Overall, high levels of the negative affect trait are related to emotional eating. Negative affectivity is a personality trait involving negative emotions and poor self-concept. Negative emotions experienced within negative affect include anger, guilt, and nervousness. It has been found that certain negative affect regulation scales predicted emotional eating. An inability to articulate and identify one’s emotions made the individual feel inadequate at regulating negative affect and thus more likely to engage in emotional eating as a means for coping with those negative emotions. Further scientific studies regarding the relationship between negative affect and eating find that, after experiencing a stressful event, food consumption is associated with reduced feelings of negative affect (i.e. feeling less bad) for those enduring high levels of chronic stress. This relationship between eating and feeling better suggests a self-reinforcing cyclical pattern between high levels of chronic stress and consumption of highly palatable foods as a coping mechanism. Contrarily, a study conducted by Spoor et al. found that negative affect is not significantly related to emotional eating, but the two are indirectly associated through emotion-focused coping and avoidance-distraction behaviours. While the scientific results differed somewhat, they both suggest that negative affect does play a role in emotional eating but it may be accounted for by other variables.
Childhood Development
For some people, emotional eating is a learned behaviour. During childhood, their parents give them treats to help them deal with a tough day or situation, or as a reward for something good. Over time, the child who reaches for a cookie after getting a bad grade on a test may become an adult who grabs a box of cookies after a rough day at work. In an example such as this, the roots of emotional eating are deep, which can make breaking the habit extremely challenging. In some cases, individuals may eat in order to conform; for example, individuals may be told “you have to finish your plate” and the individual may eat past the point in which they feel satisfied.
Related Disorders
Emotional eating as a means to cope may be a precursor to developing eating disorders such as binge eating or bulimia nervosa. The relationship between emotional eating and other disorders is largely due to the fact that emotional eating and these disorders share key characteristics. More specifically, they are both related to emotion focused coping, maladaptive coping strategies, and a strong aversion to negative feelings and stimuli. It is important to note that the causal direction has not been definitively established, meaning that while emotional eating is considered a precursor to these eating disorders, it also may be the consequence of these disorders. The latter hypothesis that emotional eating happens in response to another eating disorder is supported by research that has shown emotional eating to be more common among individuals already suffering from bulimia nervosa.
Biological and Environmental Factors
Stress affects food preferences. Numerous studies – granted, many of them in animals – have shown that physical or emotional distress increases the intake of food high in fat, sugar, or both, even in the absence of caloric deficits. Once ingested, fat- and sugar-filled foods seem to have a feedback effect that damps stress-related responses and emotions, as these foods trigger dopamine and opioid releases, which protect against the negative consequences of stress. These foods really are “comfort” foods in that they seem to counteract stress, but rat studies demonstrate that intermittent access to and consumption of these highly palatable foods creates symptoms that resemble opioid withdrawal, suggesting that high-fat and high-sugar foods can become neurologically addictive. A few examples from the American diet would include: hamburgers, pizza, French fries, sausages and savoury pasties. The most common food preferences are in decreasing order from: sweet energy-dense food, non-sweet energy-dense food then, fruits and vegetables. This may contribute to people’s stress-induced craving for those foods.
The stress response is a highly-individualised reaction and personal differences in physiological reactivity may also contribute to the development of emotional eating habits. Women are more likely than men to resort to eating as a coping mechanism for stress, as are obese individuals and those with histories of dietary restraint. In one study, women were exposed to an hour-long social stressor task or a neutral control condition. The women were exposed to each condition on different days. After the tasks, the women were invited to a buffet with both healthy and unhealthy snacks. Those who had high chronic stress levels and a low cortisol reactivity to the acute stress task consumed significantly more calories from chocolate cake than women with low chronic stress levels after both control and stress conditions. High cortisol levels, in combination with high insulin levels, may be responsible for stress-induced eating, as research shows high cortisol reactivity is associated with hyperphagia, an abnormally increased appetite for food, during stress. Furthermore, since glucocorticoids trigger hunger and specifically increase one’s appetite for high-fat and high-sugar foods, those whose adrenal glands naturally secrete larger quantities of glucocorticoids in response to a stressor are more inclined toward hyperphagia. Additionally, those whose bodies require more time to clear the bloodstream of excess glucocorticoids are similarly predisposed.
These biological factors can interact with environmental elements to further trigger hyperphagia. Frequent intermittent stressors trigger repeated, sporadic releases of glucocorticoids in intervals too short to allow for a complete return to baseline levels, leading to sustained and elevated levels of appetite. Therefore, those whose lifestyles or careers entail frequent intermittent stressors over prolonged periods of time thus have greater biological incentive to develop patterns of emotional eating, which puts them at risk for long-term adverse health consequences such as weight gain or cardiovascular disease.
Macht (2008) described a five-way model to explain the reasoning behind stressful eating:
Emotional control of food choice;
Emotional suppression of food intake;
Impairment of cognitive eating controls;
Eating to regulate emotions; and
Emotion-congruent modulation of eating.
These break down into subgroups of: Coping, reward enhancement, social and conformity motive. Thus, providing an individual with are stronger understanding of personal emotional eating.
Positive Affect
Geliebter and Aversa (2003) conducted a study comparing individuals of three weight groups: underweight, normal weight and overweight. Both positive and negative emotions were evaluated. When individuals were experiencing positive emotional states or situations, the underweight group reporting eating more than the other two groups. As an explanation, the typical nature of underweight individuals is to eat less and during times of stress to eat even less. However, when positive emotional states or situations arise, individuals are more likely to indulge themselves with food.
Impact
Emotional eating may qualify as avoidant coping and/or emotion-focused coping. As coping methods that fall under these broad categories focus on temporary reprieve rather than practical resolution of stressors, they can initiate a vicious cycle of maladaptive behaviour reinforced by fleeting relief from stress. Additionally, in the presence of high insulin levels characteristic of the recovery phase of the stress-response, glucocorticoids trigger the creation of an enzyme that stores away the nutrients circulating in the bloodstream after an episode of emotional eating as visceral fat, or fat located in the abdominal area. Therefore, those who struggle with emotional eating are at greater risk for abdominal obesity, which is in turn linked to a greater risk for metabolic and cardiovascular disease.
Treatment
There are numerous ways in which individuals can reduce emotional distress without engaging in emotional eating as a means to cope. The most salient choice is to minimise maladaptive coping strategies and to maximise adaptive strategies. A study conducted by Corstorphine et al. in 2007 investigated the relationship between distress tolerance and disordered eating. These researchers specifically focused on how different coping strategies impact distress tolerance and disordered eating. They found that individuals who engage in disordered eating often employ emotional avoidance strategies. If an individual is faced with strong negative emotions, they may choose to avoid the situation by distracting themselves through overeating. Discouraging emotional avoidance is thus an important facet to emotional eating treatment. The most obvious way to limit emotional avoidance is to confront the issue through techniques like problem solving. Corstorphine et al. showed that individuals who engaged in problem solving strategies enhance one’s ability to tolerate emotional distress. Since emotional distress is correlated to emotional eating, the ability to better manage one’s negative affect should allow an individual to cope with a situation without resorting to overeating.
One way to combat emotional eating is to employ mindfulness techniques. For example, approaching cravings with a non-judgemental inquisitiveness can help differentiate between hunger and emotionally-driven cravings. An individual may ask his or herself if the craving developed rapidly, as emotional eating tends to be triggered spontaneously. An individual may also take the time to note his or her bodily sensations, such as hunger pangs, and coinciding emotions, like guilt or shame, in order to make conscious decisions to avoid emotional eating.
Emotional eating can also be improved by evaluating physical facets like hormone balance. Female hormones, in particular, can alter cravings and even self-perception of one’s body. Additionally, emotional eating can be exacerbated by social pressure to be thin. The focus on thinness and dieting in our culture can make young girls, especially, vulnerable to falling into food restriction and subsequent emotional eating behaviour.
Emotional eating disorder predisposes individuals to more serious eating disorders and physiological complications. Therefore, combatting disordered eating before such progression takes place has become the focus of many clinical psychologists.
Stress Fasting
In a lesser percentage of individuals, emotional eating may conversely consist of reduced food intake, or stress fasting. This is believed to result from the fight-or-flight response. In some individuals, depression and other psychological disorders can also lead to emotional fasting or starvation.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Emotional_eating >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.

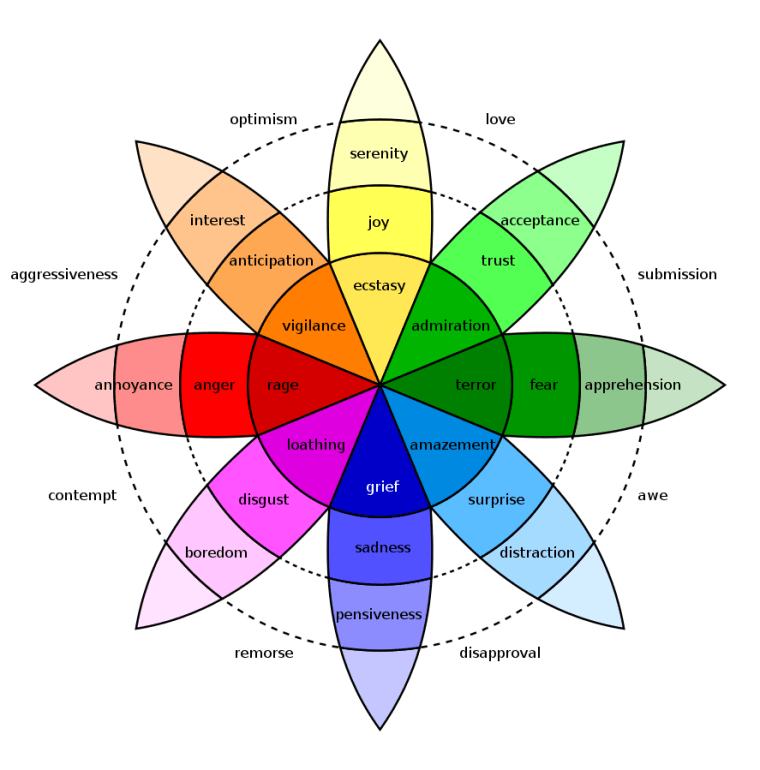


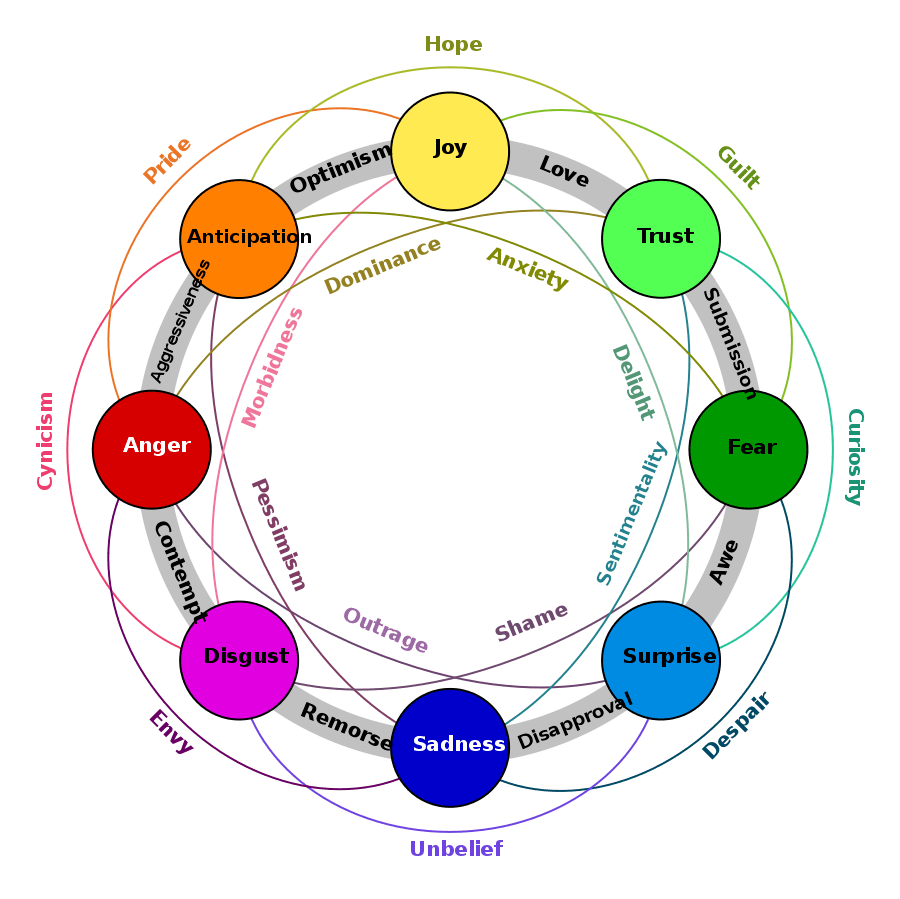







You must be logged in to post a comment.