Emotional contagion is a form of social contagion that involves the spontaneous spread of emotions and related behaviours. Such emotional convergence can happen from one person to another, or in a larger group. Emotions can be shared across individuals in many ways, both implicitly or explicitly. For instance, conscious reasoning, analysis, and imagination have all been found to contribute to the phenomenon. The behaviour has been found in humans, other primates, dogs, and chickens.
Plutchik Wheel
Emotional contagion is important to personal relationships because it fosters emotional synchrony between individuals. A broader definition of the phenomenon suggested by Schoenewolf is:
“a process in which a person or group influences the emotions or behavior of another person or group through the conscious or unconscious induction of emotion states and behavioral attitudes.”
One view developed by Elaine Hatfield, et al., is that this can be done through automatic mimicry and synchronisation of one’s expressions, vocalisations, postures, and movements with those of another person. When people unconsciously mirror their companions’ expressions of emotion, they come to feel reflections of those companions’ emotions.
In a 1993 paper, Psychologists Elaine Hatfield, John Cacioppo, and Richard Rapson define emotional contagion as “the tendency to automatically mimic and synchronize expressions, vocalizations, postures, and movements with those of another person’s [sic] and, consequently, to converge emotionally”.
Hatfield, et al., theorise emotional contagion as a two-step process: First, we imitate people (e.g. if someone smiles at you, you smile back). Second, our own emotional experiences change based on the non-verbal signals of emotion that we give off. For example, smiling makes one feel happier, and frowning makes one feel worse. Mimicry seems to be one foundation of emotional movement between people.
Emotional contagion and empathy share similar characteristics, with the exception of the ability to differentiate between personal and pre-personal experiences, a process known as individuation. In The Art of Loving (1956), social psychologist Erich Fromm explores these differences, suggesting that autonomy is necessary for empathy, which is not found in emotional contagion.
Etymology
James Baldwin addressed “emotional contagion” in his 1897 work Social and Ethical Interpretations in Mental Development, though using the term “contagion of feeling”. Various 20th century scholars discussed the phenomena under the heading “social contagion”. The term “emotional contagion” first appeared in Arthur S. Reber’s 1985 The Penguin Dictionary of Psychology.
Influencing Factors
Several factors determine the rate and extent of emotional convergence in a group, including membership stability, mood-regulation norms, task interdependence, and social interdependence. Besides these event-structure properties, there are personal properties of the group’s members, such as openness to receive and transmit feelings, demographic characteristics, and dispositional affect that influence the intensity of emotional contagion.
Research
Research on emotional contagion has been conducted from a variety of perspectives, including organisational, social, familial, developmental, and neurological. While early research suggested that conscious reasoning, analysis, and imagination accounted for emotional contagion, some forms of more primitive emotional contagion are far more subtle, automatic, and universal.
Hatfield, Cacioppo, and Rapson’s 1993 research into emotional contagion reported that people’s conscious assessments of others’ feelings were heavily influenced by what others said. People’s own emotions, however, were more influenced by others’ nonverbal clues as to what they were really feeling. Recognizing emotions and acknowledging their origin can be one way to avoid emotional contagion. Transference of emotions has been studied in a variety of situations and settings, with social and physiological causes being two of the largest areas of research.
In addition to the social contexts discussed above, emotional contagion has been studied within organisations. Schrock, Leaf, and Rohr (2008) say organizations, like societies, have emotion cultures that consist of languages, rituals, and meaning systems, including rules about the feelings workers should, and should not, feel and display. They state that emotion culture is quite similar to “emotion climate”, otherwise known as morale, organisational morale, and corporate morale. Furthermore, Worline, Wrzesniewski, and Rafaeli (2002): 318 mention that organizations have an overall “emotional capability”, while McColl-Kennedy, and Smith (2006) examine “emotional contagion” in customer interactions. These terms arguably all attempt to describe a similar phenomenon; each term differs in subtle and somewhat indistinguishable ways.
Controversy
A controversial experiment demonstrating emotional contagion by using the social media platform Facebook was carried out in 2014 on 689,000 users by filtering positive or negative emotional content from their news feeds. The experiment sparked uproar among people who felt the study violated personal privacy. The 2014 publication of a research paper resulting from this experiment, “Experimental evidence of massive-scale emotional contagion through social networks”, a collaboration between Facebook and Cornell University, is described by Tony D. Sampson, Stephen Maddison, and Darren Ellis (2018) as a “disquieting disclosure that corporate social media and Cornell academics were so readily engaged with unethical experiments of this kind.” Tony D. Sampson et al. criticise the notion that “academic researchers can be insulated from ethical guidelines on the protection for human research subjects because they are working with a social media business that has ‘no obligation to conform’ to the principle of ‘obtaining informed consent and allowing participants to opt out’.” A subsequent study confirmed the presence of emotional contagion on Twitter without manipulating users’ timelines.
Beyond the ethical concerns, some scholars criticised the methods and reporting of the Facebook findings. John Grohol, writing for Psych Central, argued that despite its title and claims of “emotional contagion,” this study did not look at emotions at all. Instead, its authors used an application (called “Linguistic Inquiry and Word Count” or LIWC 2007) that simply counted positive and negative words in order to infer users’ sentiments. A shortcoming of the LIWC tool is that it does not understand negations. Hence, the tweet “I am not happy” would be scored as positive: “Since the LIWC 2007 ignores these subtle realities of informal human communication, so do the researchers.” Grohol concluded that given these subtleties, the effect size of the findings are little more than a “statistical blip.”
Kramer et al. (2014) found a 0.07%—that’s not 7 percent, that’s 1/15th of one percent!!—decrease in negative words in people’s status updates when the number of negative posts on their Facebook news feed decreased. Do you know how many words you’d have to read or write before you’ve written one less negative word due to this effect? Probably thousands.
Types
Emotions can be shared and mimicked in many ways. Taken broadly, emotional contagion can be either: implicit, undertaken by the receiver through automatic or self-evaluating processes; or explicit, undertaken by the transmitter through a purposeful manipulation of emotional states, to achieve a desired result.
Implicit
Unlike cognitive contagion, emotional contagion is less conscious and more automatic. It relies mainly on non-verbal communication, although emotional contagion can and does occur via telecommunication. For example, people interacting through e-mails and chats are affected by the other’s emotions, without being able to perceive the non-verbal cues.
One view, proposed by Hatfield and colleagues, describes emotional contagion as a primitive, automatic, and unconscious behaviour that takes place through a series of steps. When a receiver is interacting with a sender, he perceives the emotional expressions of the sender. The receiver automatically mimics those emotional expressions. Through the process of afferent feedback, these new expressions are translated into feeling the emotions the sender feels, thus leading to emotional convergence.
Another view, emanating from social comparison theories, sees emotional contagion as demanding more cognitive effort and being more conscious. According to this view, people engage in social comparison to see if their emotional reaction is congruent with the persons around them. The recipient uses the emotion as a type of social information to understand how he or she should be feeling. People respond differently to positive and negative stimuli; negative events tend to elicit stronger and quicker emotional, behavioural, and cognitive responses than neutral or positive events. So unpleasant emotions are more likely to lead to mood contagion than are pleasant emotions. Another variable is the energy level at which the emotion is displayed. Higher energy draws more attention to it, so the same emotional valence (pleasant or unpleasant) expressed with high energy is likely to lead to more contagion than if expressed with low energy.
Explicit
Aside from the automatic infection of feelings described above, there are also times when others’ emotions are being manipulated by a person or a group in order to achieve something. This can be a result of intentional affective influence by a leader or team member. Suppose this person wants to convince the others of something, he may do so by sweeping them up in his enthusiasm. In such a case, his positive emotions are an act with the purpose of “contaminating” the others’ feelings. A different kind of intentional mood contagion would be, for instance, giving the group a reward or treat, in order to alleviate their feelings.
The discipline of organisational psychology researches aspects of emotional labour. This includes the need to manage emotions so that they are consistent with organisational or occupational display rules, regardless of whether they are discrepant with internal feelings. In regard to emotional contagion, in work settings that require a certain display of emotions, one finds oneself obligated to display, and consequently feel, these emotions. If superficial acting develops into deep acting, emotional contagion is the byproduct of intentional affective impression management.
In Workplaces and Organisations
Intra-Group
Many organisations and workplaces encourage teamwork. Studies conducted by organisational psychologists highlight the benefits of work teams. Emotions come into play and a group emotion is formed.
The group’s emotional state influences factors such as cohesiveness, morale, rapport, and the team’s performance. For this reason, organisations need to take into account the factors that shape the emotional state of the work-teams, in order to harness the beneficial sides and avoid the detrimental sides of the group’s emotion. Managers and team leaders should be cautious with their behaviour, since their emotional influence is greater than that of a “regular” team member: leaders are more emotionally “contagious” than others.
Employee/Customer
The interaction between service employees and customers affects both customers’ assessments of service quality and their relationship with the service provider. Positive affective displays in service interactions are positively associated with important customer outcomes, such as intention to return and to recommend the store to a friend. It is the interest of organisations that their customers be happy, since a happy customer is a satisfied one. Research has shown that the emotional state of the customer is directly influenced by the emotions displayed by the employee/service provider via emotional contagion. But this influence depends on authenticity of the employee’s emotional display, such that if the employee is only surface-acting, the contagion is poor, in which case the beneficial effects will not occur.
Neurological Basis
Vittorio Gallese posits that mirror neurons are responsible for intentional attunement in relation to others. Gallese and colleagues at the University of Parma found a class of neurons in the premotor cortex that discharge either when macaque monkeys execute goal-related hand movements or when they watch others doing the same action. One class of these neurons fires with action execution and observation, and with sound production of the same action. Research in humans shows an activation of the premotor cortex and parietal area of the brain for action perception and execution.
Gallese says humans understand emotions through a simulated shared body state. The observers’ neural activation enables a direct experiential understanding. “Unmediated resonance” is a similar theory by Goldman and Sripada (2004). Empathy can be a product of the functional mechanism in our brain that creates embodied simulation. The other we see or hear becomes the “other self” in our minds. Other researchers have shown that observing someone else’s emotions recruits brain regions involved in:
Experiencing similar emotions; and
Producing similar facial expressions.
This combination indicates that the observer activates:
A representation of the emotional feeling of the other individual which leads to emotional contagion; and
A motor representation of the observed facial expression that could lead to facial mimicry.
In the brain, understanding and sharing other individuals’ emotions would thus be a combination of emotional contagion and facial mimicry. Importantly, more empathic individuals experience more brain activation in emotional regions while witnessing the emotions of other individuals.
Amygdala
The amygdala is one part of the brain that underlies empathy and allows for emotional attunement and creates the pathway for emotional contagion. The basal areas including the brain stem form a tight loop of biological connectedness, re-creating in one person the physiological state of the other. Psychologist Howard Friedman thinks this is why some people can move and inspire others. The use of facial expressions, voices, gestures and body movements transmit emotions to an audience from a speaker.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Emotional_contagion >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Social emotions are emotions that depend upon the thoughts, feelings or actions of other people, “as experienced, recalled, anticipated or imagined at first hand”. Examples are embarrassment, guilt, shame, jealousy, envy, coolness, elevation, empathy, and pride. In contrast, basic emotions such as happiness and sadness only require the awareness of one’s own physical state. Therefore, the development of social emotions is tightly linked with the development of social cognition, the ability to imagine other people’s mental states, which generally develops in adolescence. Studies have found that children as young as 2 to 3 years of age can express emotions resembling guilt and remorse. However, while five-year-old children are able to imagine situations in which basic emotions would be felt, the ability to describe situations in which social emotions might be experienced does not appear until seven years of age.
People may not only share emotions with others, but may also experience similar physiological arousal to others if they feel a sense of social connectedness to the other person. A laboratory-based study by Cwir, Car, Walton, and Spencer (2011) showed that, when a participant felt a sense of social connectedness to a stranger (research confederate), the participant experienced similar emotional states and physiological responses to that of the stranger while observing the stranger perform a stressful task.
Social emotions are sometimes called moral emotions, because they play an important role in morality and moral decision making. In neuroeconomics, the role social emotions play in game theory and economic decision-making is just starting to be investigated.
Behavioural Neuroscience
After functional imaging—functional magnetic resonance imaging (fMRI) in particular—became popular roughly a decade ago, researchers have begun to study economic decision-making with this new technology. This allows researchers to investigate, on a neurological level, the role emotions play in decision-making.
Developmental Picture
The ability to describe situations in which a social emotion will be experienced emerges at around age 7, and, by adolescence, the experience of social emotion permeates everyday social exchange. Studies using fMRI have found that different brain regions are involved in different age groups when performing social-cognitive and social-emotional tasks. While brain areas such as medial prefrontal cortex (MPFC), superior temporal sulcus (STS), temporal poles (TP) and precuneus bordering with posterior cingulate cortex are activated in both adults and adolescents when they reason about intentionality of others, the medial PFC is more activated in adolescents and the right STS more in adults. Similar age effects were found with younger participants, such that, when participants perform tasks that involve theory of mind, increase in age is correlated with an increase in activation in the dorsal part of the MPFC and a decrease in the activity in the ventral part of the MPFC were observed.
Studies that compare adults with adolescents in their processing of basic and social emotions also suggest developmental shifts in brain areas being involved. Comparing with adolescents, the left temporal pole has a stronger activity in adults when they read stories that elicit social emotions. The temporal poles are thought to store abstract social knowledge. This suggests that adult might use social semantic knowledge more often when thinking about social-emotional situations than adolescents.
Neuroeconomics
To investigate the function of social emotions in economic behaviours, researchers are interested in the differences in brain regions involved when participants are playing with, or think that they are playing with, another person as opposed to a computer. A study with fMRI found that, for participants who tend to cooperate on two-person “trust and reciprocity” games, believing that they are playing with another participant activated the prefrontal cortex, while believing that they are playing with a computer did not. This difference was not seen with players who tend not to cooperate. The authors interpret this difference as theory of minds that co-operators employ to anticipate the opponents’ strategies. This is an example of the way social decision making differs from other forms of decision making.
In behavioural economics, a heavy criticism is that people do not always act in a fully rational way, as many economic models assume. For example, in the ultimatum game, two players are asked to divide a certain amount of money, say x. One player, called the proposer, decides ratio by which the money gets divided. The other player, called the responder, decides whether or not to accept this offer. If the responder accepts the offer, say, y amount of money, then the proposer gets x-y amount and the responder gets y. But if the responder refuses to accept the offer, both players get nothing. This game is widely studied in behavioural economics. According to the rational agent model, the most rational way for the proposer to act is to make y as small as possible, and the most rational way for the responder to act is to accept the offer, since little amount of money is better than no money. However, what these experiments tend to find is that the proposers tend to offer 40% of x, and offers below 20% would get rejected by the responders. Using fMRI scans, researchers found that social emotions elicited by the offers may play a role in explaining the result. When offers are unfair as opposed to fair, three regions of the brain are active: the dorsolateral prefrontal cortex (DLPFC), the anterior cingulate cortex (ACC), and the insula. The insula is an area active in registering body discomfort. It is activated when people feel, among other things, social exclusion. The authors interpret activity in the insula as the aversive reaction one feels when faced with unfairness, activity in the DLPFC as processing the future reward from keeping the money, and the ACC is an arbiter that weighs these two conflicting inputs to make a decision. Whether or not the offer gets rejected can be predicted (with a correlation of 0.45) by the level of the responder’s insula activity.
Neuroeconomics and social emotions are also tightly linked in the study of punishment. Research using PET scan has found that, when players punish other players, activity in the nucleus accumbens (part of the striatum), a region known for processing rewards derived from actions gets activated. It shows that we not only feel hurtful when we become victims of unfairness, but we also find it psychologically rewarding to punish the wrongdoer, even at a cost to our own utility.
Social or Moral Aspect
Some social emotions are also referred to as moral emotions because of the fundamental role they play in morality. For example, guilt is the discomfort and regret one feels over one’s wrongdoing. It is a social emotion, because it requires the perception that another person is being hurt by this act; and it also has implication in morality, such that the guilty actor, in virtue of feeling distressed and guilty, accepts responsibility for the wrongdoing, which might cause desire to make amends or punish the self.
Not all social emotions are moral emotions. Pride, for instance, is a social emotion which involves the perceived admiration of other people, but research on the role it plays in moral behaviours yields problematic results.
Empathic Response
Empathy is defined by Eisenberg and colleagues as an affective response that stems from the apprehension or comprehension of another’s emotional state or condition and is similar to what the other person is feeling or would be expected to feel. Guilt, which is a social emotion with strong moral implication, is also strongly correlated with empathic responsiveness; whereas shame, an emotion with less moral flavour, is negatively correlated with empathic responsiveness, when controlling for guilt.
Perceived controllability also plays an important role modulating people’s socio-emotional reactions and empathic responses. For example, participants who are asked to evaluate other people’s academic performances are more likely to assign punishments when the low performance is interpreted as low-effort, as opposed to low-ability. Stigmas also elicit more empathic response when they are perceived as uncontrollable (i.e. having a biological origin, such as having certain disease), as opposed to controllable (i.e. having a behavioural origin, such as obesity).
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Social_emotions >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
The self-regulation of emotion or emotion regulation is the ability to respond to the ongoing demands of experience with the range of emotions in a manner that is socially tolerable and sufficiently flexible to permit spontaneous reactions as well as the ability to delay spontaneous reactions as needed. It can also be defined as extrinsic and intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions. The self-regulation of emotion belongs to the broader set of emotion regulation processes, which includes both the regulation of one’s own feelings and the regulation of other people’s feelings.
Plutchik WheelPlutchik Dyads
Emotion regulation is a complex process that involves initiating, inhibiting, or modulating one’s state or behaviour in a given situation — for example, the subjective experience (feelings), cognitive responses (thoughts), emotion-related physiological responses (for example heart rate or hormonal activity), and emotion-related behaviour (bodily actions or expressions). Functionally, emotion regulation can also refer to processes such as the tendency to focus one’s attention to a task and the ability to suppress inappropriate behaviour under instruction. Emotion regulation is a highly significant function in human life.
Every day, people are continually exposed to a wide variety of potentially arousing stimuli. Inappropriate, extreme or unchecked emotional reactions to such stimuli could impede functional fit within society; therefore, people must engage in some form of emotion regulation almost all of the time. Generally speaking, emotion dysregulation has been defined as difficulties in controlling the influence of emotional arousal on the organisation and quality of thoughts, actions, and interactions. Individuals who are emotionally dysregulated exhibit patterns of responding in which there is a mismatch between their goals, responses, and/or modes of expression, and the demands of the social environment. For example, there is a significant association between emotion dysregulation and symptoms of depression, anxiety, eating pathology, and substance abuse. Higher levels of emotion regulation are likely to be related to both high levels of social competence and the expression of socially appropriate emotions.
Theory
Process Model
The process model of emotion regulation is based upon the modal model of emotion. The modal model of emotion suggests that the emotion generation process occurs in a particular sequence over time. This sequence occurs as follows:
Situation: the sequence begins with a situation (real or imagined) that is emotionally relevant.
Attention: attention is directed towards the emotional situation.
Appraisal: the emotional situation is evaluated and interpreted.
Response: an emotional response is generated, giving rise to loosely coordinated changes in experiential, behavioural, and physiological response systems.
Because an emotional response (4.) can cause changes to a situation (1.), this model involves a feedback loop from (4.) Response to (1.) Situation. This feedback loop suggests that the emotion generation process can occur recursively, is ongoing, and dynamic.
The process model contends that each of these four points in the emotion generation process can be subjected to regulation. From this conceptualization, the process model posits five different families of emotion regulation that correspond to the regulation of a particular point in the emotion generation process. They occur in the following order:
Situation selection
Situation modification
Attentional deployment
Cognitive change
Response modulation
The process model also divides these emotion regulation strategies into two categories: antecedent-focused and response-focused. Antecedent-focused strategies (i.e. situation selection, situation modification, attentional deployment, and cognitive change) occur before an emotional response is fully generated. Response-focused strategies (i.e. response modulation) occur after an emotional response is fully generated.
Strategies
Situation Selection
Situation selection is an emotional regulation strategy that involves choosing to avoid or approach a future emotional situation. If a person selects to avoid or disengage from an emotionally relevant situation, they are decreasing the likelihood of experiencing an emotion. Alternatively, if a person selects to approach or engage with an emotionally relevant situation, they are increasing the likelihood of experiencing an emotion.
Typical examples of situation selection may be seen interpersonally, such as when a parent removes his or her child from an emotionally unpleasant situation. Use of situation selection may also be seen in psychopathology. For example, avoidance of social situations to regulate emotions is particularly pronounced for those with social anxiety disorder and avoidant personality disorder.
Effective situation selection is not always an easy task. For instance, humans display difficulties predicting their emotional responses to future events. Therefore, they may have trouble making accurate and appropriate decisions about which emotionally relevant situations to approach or to avoid.
Situation Modification
Situation modification involves efforts to modify a situation so as to change its emotional impact. Situation modification refers specifically to altering one’s external, physical environment. Altering one’s “internal” environment to regulate emotion is called cognitive change.
Examples of situation modification may include injecting humour into a speech to elicit laughter or extending the physical distance between oneself and another person.
Attentional Deployment
Attentional deployment involves directing one’s attention towards or away from an emotional situation.
Distraction
Distraction, an example of attentional deployment, is an early selection strategy, which involves diverting one’s attention away from an emotional stimulus and towards other content. Distraction has been shown to reduce the intensity of painful and emotional experiences, to decrease facial responding and neural activation in the amygdala associated with emotion, as well as to alleviate emotional distress. As opposed to reappraisal, individuals show a relative preference to engage in distraction when facing stimuli of high negative emotional intensity. This is because distraction easily filters out high-intensity emotional content, which would otherwise be relatively difficult to appraise and process.
Rumination
Rumination, an example of attentional deployment, is defined as the passive and repetitive focusing of one’s attention on one’s symptoms of distress and the causes and consequences of these symptoms. Rumination is generally considered a maladaptive emotion regulation strategy, as it tends to exacerbate emotional distress. It has also been implicated in a host of disorders including major depression.
Worry
Worry, an example of attentional deployment, involves directing attention to thoughts and images concerned with potentially negative events in the future. By focusing on these events, worrying serves to aid in the down-regulation of intense negative emotion and physiological activity. While worry may sometimes involve problem solving, incessant worry is generally considered maladaptive, being a common feature of anxiety disorders, particularly generalised anxiety disorder.
Thought Suppression
Thought suppression, an example of attentional deployment, involves efforts to redirect one’s attention from specific thoughts and mental images to other content so as to modify one’s emotional state. Although thought suppression may provide temporary relief from undesirable thoughts, it may ironically end up spurring the production of even more unwanted thoughts. This strategy is generally considered maladaptive, being most associated with obsessive-compulsive disorder.
Cognitive Change
Cognitive change involves changing how one appraises a situation so as to alter its emotional meaning.
Reappraisal
Reappraisal, an example of cognitive change, is a late selection strategy, which involves a change of the meaning of an event that alters its emotional impact. It encompasses different sub-strategies, such as positive reappraisal (creating and focusing on a positive aspect of the stimulus), decentring (reinterpreting an event by broadening one’s perspective to see “the bigger picture”), or fictional reappraisal (adopting or emphasizing the belief that event is not real, that it is for instance “just a movie” or “just my imagination”). Reappraisal has been shown to effectively reduce physiological, subjective, and neural emotional responding. As opposed to distraction, individuals show a relative preference to engage in reappraisal when facing stimuli of low negative emotional intensity because these stimuli are relatively easy to appraise and process.
Reappraisal is generally considered to be an adaptive emotion regulation strategy. Compared to suppression (including both thought suppression and expressive suppression), which is positively correlated with many psychological disorders, reappraisal can be associated with better interpersonal outcomes, and can be positively related to well-being. However, some researchers argue that context is important when evaluating the adaptiveness of a strategy, suggesting that in some contexts reappraisal may be maladaptive. Furthermore, some research has shown reappraisal does not influence or affect physiological responses to recurrent stress.
Distancing
Distancing, an example of cognitive change, involves taking on an independent, third-person perspective when evaluating an emotional event. Distancing has been shown to be an adaptive form of self-reflection, facilitating the emotional processing of negatively valenced stimuli, reducing emotional and cardiovascular reactivity to negative stimuli, and increasing problem-solving behaviour.
Humour
Humour, an example of cognitive change, has been shown to be an effective emotion regulation strategy. Specifically, positive, good-natured humour has been shown to effectively up-regulate positive emotion and down-regulate negative emotion. On the other hand, negative, mean-spirited humour is less effective in this regard.
Response Modulation
Response modulation involves attempts to directly influence experiential, behavioural, and physiological response systems.
Expressive Suppression
Expressive suppression, an example of response modulation, involves inhibiting emotional expressions. It has been shown to effectively reduce facial expressivity, subjective feelings of positive emotion, heart rate, and sympathetic activation. However, the research findings are mixed regarding whether this strategy is effective for down-regulating negative emotion. Research has also shown that expressive suppression may have negative social consequences, correlating with reduced personal connections and greater difficulties forming relationships.
Expressive suppression is generally considered to be a maladaptive emotion regulation strategy. Compared to reappraisal, it is positively correlated with many psychological disorders, associated with worse interpersonal outcomes, is negatively related to well-being, and requires the mobilisation of a relatively substantial amount of cognitive resources. However, some researchers argue that context is important when evaluating the adaptiveness of a strategy, suggesting that in some contexts suppression may be adaptive.
Drug Use
Drug use, an example of response modulation, can be used to alter emotion-associated physiological responses. For example, alcohol can produce sedative and anxiolytic effects and beta blockers can affect sympathetic activation.
Exercise
Exercise, an example of response modulation, can be used to down-regulate the physiological and experiential effects of negative emotions. Regular physical activity has also been shown to reduce emotional distress and improve emotional control.
Sleep
Sleep plays a role in emotion regulation, although stress and worry can also interfere with sleep. Studies have shown that sleep, specifically REM sleep, down-regulates reactivity of the amygdala, a brain structure known to be involved in the processing of emotions, in response to previous emotional experiences. On the flip side, sleep deprivation is associated with greater emotional reactivity or overreaction to negative and stressful stimuli. This is a result of both increased amygdala activity and a disconnect between the amygdala and the prefrontal cortex, which regulates the amygdala through inhibition, together resulting in an overactive emotional brain. Due to the subsequent lack of emotional control, sleep deprivation may be associated with depression, impulsivity, and mood swings. Additionally, there is some evidence that sleep deprivation may reduce emotional reactivity to positive stimuli and events and impair emotion recognition in others.
For example, a relevant mnemonic formulated in DBT is “ABC PLEASE”:
Accumulate positive experiences.
Build mastery by being active in activities that make one feel competent and effective to combat helplessness.
Cope ahead, preparing an action plan, researching, and rehearsing (with a skilled helper if necessary).
Physical illness treatment and prevention through check-ups.
Low vulnerability to diseases, managed with health care professionals.
Eating healthy.
Avoiding (non-prescribed) mood-altering drugs.
Sleep healthy.
Exercise regularly.
Developmental Process
Infancy
Intrinsic emotion regulation efforts during infancy are believed to be guided primarily by innate physiological response systems. These systems usually manifest as an approach towards and an avoidance of pleasant or unpleasant stimuli. At three months, infants can engage in self-soothing behaviours like sucking and can reflexively respond to and signal feelings of distress. For instance, infants have been observed attempting to suppress anger or sadness by knitting their brow or compressing their lips.
Between three and six months, basic motor functioning and attentional mechanisms begin to play a role in emotion regulation, allowing infants to more effectively approach or avoid emotionally relevant situations. Infants may also engage in self-distraction and help-seeking behaviours for regulatory purposes. At one year, infants are able to navigate their surroundings more actively and respond to emotional stimuli with greater flexibility due to improved motor skills. They also begin to appreciate their caregivers’ abilities to provide them regulatory support. For instance, infants generally have difficulties regulating fear. As a result, they often find ways to express fear in ways that attract the comfort and attention of caregivers.
Extrinsic emotion regulation efforts by caregivers, including situation selection, modification, and distraction, are particularly important for infants. The emotion regulation strategies employed by caregivers to attenuate distress or to up-regulate positive affect in infants can impact the infants’ emotional and behavioural development, teaching them particular strategies and methods of regulation. The type of attachment style between caregiver and infant can therefore play a meaningful role in the regulatory strategies infants may learn to use.
Recent evidence supports the idea that maternal singing has a positive effect on affect regulation in infants. Singing play-songs can have a visible affect-regulatory consequence of prolonged positive affect and even alleviation of distress. In addition to proven facilitation of social bonding, when combined with movement and/or rhythmic touch, maternal singing for affect regulation has possible applications for infants in the NICU and for adult caregivers with serious personality or adjustment difficulties.
Toddler-hood
By the end of the first year, toddlers begin to adopt new strategies to decrease negative arousal. These strategies can include rocking themselves, chewing on objects, or moving away from things that upset them. At two years, toddlers become more capable of actively employing emotion regulation strategies. They can apply certain emotion regulation tactics to influence various emotional states. Additionally, maturation of brain functioning and language and motor skills permits toddlers to manage their emotional responses and levels of arousal more effectively.
Extrinsic emotion regulation remains important to emotional development in toddlerhood. Toddlers can learn ways from their caregivers to control their emotions and behaviours. For example, caregivers help teach self-regulation methods by distracting children from unpleasant events (like a vaccination shot) or helping them understand frightening events.
Childhood
Emotion regulation knowledge becomes more substantial during childhood. For example, children aged six to ten begin to understand display rules. They come to appreciate the contexts in which certain emotional expressions are socially most appropriate and therefore ought to be regulated. For example, children may understand that upon receiving a gift they should display a smile, irrespective of their actual feelings about the gift. During childhood, there is also a trend towards the use of more cognitive emotion regulation strategies, taking the place of more basic distraction, approach, and avoidance tactics.
Regarding the development of emotion dysregulation in children, one robust finding suggests that children who are frequently exposed to negative emotion at home will be more likely to display, and have difficulties regulating, high levels of negative emotion.
Adolescence
Adolescents show a marked increase in their capacities to regulate their emotions, and emotion regulation decision making becomes more complex, depending on multiple factors. In particular, the significance of interpersonal outcomes increases for adolescents. When regulating their emotions, adolescents are therefore likely to take into account their social context. For instance, adolescents show a tendency to display more emotion if they expect a sympathetic response from their peers.
Additionally, spontaneous use of cognitive emotion regulation strategies increases during adolescence, which is evidenced both by self-report data and neural markers.
Adulthood
Social losses increase and health tends to decrease as people age. As people get older their motivation to seek emotional meaning in life through social ties tends to increase. Autonomic responsiveness decreases with age, and emotion regulation skill tends to increase.
Emotional regulation in adulthood can also be examined in terms of positive and negative affectivity. Positive and negative affectivity refers to the types of emotions felt by an individual as well as the way those emotions are expressed. With adulthood comes an increased ability to maintain both high positive affectivity and low negative affectivity “more rapidly than adolescents.” This response to life’s challenges seems to become “automatized” as people progress throughout adulthood. Thus, as individuals age, their capability of self-regulating emotions and responding to their emotions in healthy ways improves.
Additionally, emotional regulation may vary between young adults and older adults. Younger adults have been found to be more successful than older adults in practicing “cognitive reappraisal” to decrease negative internal emotions. On the other hand, older adults have been found to be more successful in the following emotional regulation areas:
Predicting the level of “emotional arousal” in possible situations;
Having a higher focus on positive information rather than negative; and
Maintaining healthy levels of “hedonic well-being” (subjective well-being based on increased pleasure and decreased pain).
Overview of Perspectives
Neuropsychological Perspective
Affective
As people age, their affect – the way they react to emotions – changes, either positively or negatively. Studies show that positive affect increases as a person grows from adolescence to their mid 70s. Negative affect, on the other hand, decreases until the mid 70s. Studies also show that emotions differ in adulthood, particularly affect (positive or negative). Although some studies found that individuals experience less affect as they grow older, other studies have concluded that adults in their middle age experience more positive affect and less negative affect than younger adults. Positive affect was also higher for men than women while the negative affect was higher for women than it was for men and also for single people.
A reason that older people – middle adulthood – might have less negative affect is because they have overcome, “the trials and vicissitudes of youth, they may increasingly experience a more pleasant balance of affect, at least up until their mid-70s”. Positive affect might rise during middle age but towards the later years of life – the 70s – it begins to decline while negative affect also does the same. This might be due to failing health, reaching the end of their lives and the death of friends and relatives.
In addition to baseline levels of positive and negative affect, studies have found individual differences in the time-course of emotional responses to stimuli. The temporal dynamics of emotion regulation, also known as affective chronometry, include two key variables in the emotional response process: rise time to peak emotional response, and recovery time to baseline levels of emotion. Studies of affective chronometry typically separate positive and negative affect into distinct categories, as previous research has shown (despite some correlation) the ability of humans to experience changes in these categories independently of one another. Affective chronometry research has been conducted on clinical populations with anxiety, mood, and personality disorders, but is also utilised as a measurement to test the effectiveness of different therapeutic techniques (including mindfulness training) on emotional dysregulation.
Neurological
The development of functional magnetic resonance imaging has allowed for the study of emotion regulation on a biological level. Specifically, research over the last decade strongly suggests that there is a neural basis. Sufficient evidence has correlated emotion regulation to particular patterns of prefrontal activation. These regions include the orbital prefrontal cortex, the ventromedial prefrontal cortex, and the dorsolateral prefrontal cortex. Two additional brain structures that have been found to contribute are the amygdala and the anterior cingulate cortex. Each of these structures are involved in various facets of emotion regulation and irregularities in one or more regions and/or interconnections among them are affiliated with failures of emotion regulation. An implication to these findings is that individual differences in prefrontal activation predict the ability to perform various tasks in aspects of emotion regulation.
Sociological
People intuitively mimic facial expressions; it is a fundamental part of healthy functioning. Similarities across cultures in regards to nonverbal communication has prompted the debate that it is in fact a universal language. It can be argued that emotion regulation plays a key role in the ability to generate the correct responses in social situations. Humans have control over facial expressions both consciously and unconsciously: an intrinsic emotion program is generated as the result of a transaction with the world, which immediately results in an emotional response and usually a facial reaction. It is a well documented phenomenon that emotions have an effect on facial expression, but recent research has provided evidence that the opposite may also be true.
This notion would give rise to the belief that a person may not only control his emotion but in fact influence them as well. Emotion regulation focuses on providing the appropriate emotion in the appropriate circumstances. Some theories allude to the thought that each emotion serves a specific purpose in coordinating organismic needs with environmental demands (Cole, 1994). This skill, although apparent throughout all nationalities, has been shown to vary in successful application at different age groups. In experiments done comparing younger and older adults to the same unpleasant stimuli, older adults were able to regulate their emotional reactions in a way that seemed to avoid negative confrontation. These findings support the theory that with time people develop a better ability to regulate their emotions. This ability found in adults seems to better allow individuals to react in what would be considered a more appropriate manner in some social situations, permitting them to avoid adverse situations that could be seen as detrimental.
Expressive Regulation (in Solitary Conditions)
In solitary conditions, emotion regulation can include a minimization-miniaturization effect, in which common outward expressive patterns are replaced with toned down versions of expression. Unlike other situations, in which physical expression (and its regulation) serve a social purpose (i.e. conforming to display rules or revealing emotion to outsiders), solitary conditions require no reason for emotions to be outwardly expressed (although intense levels of emotion can bring out noticeable expression anyway). The idea behind this is that as people get older, they learn that the purpose of outward expression (to appeal to other people), is not necessary in situations in which there is no one to appeal to. As a result, the level of emotional expression can be lower in these solitary situations.
Stress
The way an individual reacts to stress can directly overlap with their ability to regulate emotion. Although the two concepts differ in a multitude of ways, “both coping [with stress] and emotion regulation involve affect modulation and appraisal processes” that are necessary for healthy relationships and self-identity.
According to Yu. V. Shcherbatykh, emotional stress in situations like school examinations can be reduced by engaging in self-regulating activities prior to the task being performed. To study the influence of self-regulation on mental and physiological processes under exam stress, Shcherbatykh conducted a test with an experimental group of 28 students (of both sexes) and a control group of 102 students (also of both sexes).
In the moments before the examination, situational stress levels were raised in both groups from what they were in quiet states. In the experimental group, participants engaged in three self-regulating techniques (concentration on respiration, general body relaxation, and the creation of a mental image of successfully passing the examination). During the examination, the anxiety levels of the experimental group were lower than that of the control group. Also, the percent of unsatisfactory marks in the experimental group was 1.7 times less than in the control group. From this data, Shcherbatykh concluded that the application of self-regulating actions before examinations helps to significantly reduce levels of emotional strain, which can help lead to better performance results.
Emotion regulation has also been associated with physiological responses to stress during laboratory stress paradigms.
Decision Making
Identification of our emotional self-regulating process can facilitate in the decision-making process. Current literature on emotion regulation identifies that humans characteristically make efforts in controlling emotion experiences. There is then a possibility that our present state emotions can be altered by emotion regulation strategies resulting in the possibility that different regulation strategies could have different decision implications.
Digital Emotion Regulation
Following widespread adoption in the 21st century of digital devices and services for use in everyday life, evidence is mounting that people are increasingly using these tools to manage and regulate moods and emotions. A wide range of digital resources are used for emotion regulation including smartphones, social media, streaming services, online shopping, and videogames. Such spontaneous forms of digital emotion regulation can be distinguished from the use of digital interventions such as smartphone apps that have been explicitly designed to support emotional regulation or teach emotion regulation skills in clinical and non-clinical populations. Digital implementation of emotion regulation strategies can occur at all stages of the process model and in all strategy families, including interpersonal emotion regulation.
Effects of Low Self-Regulation
With a failure in emotion regulation, there is a rise in psychosocial and emotional dysfunctions caused by traumatic experiences due to an inability to regulate emotions. These traumatic experiences typically happen in grade school and are sometimes associated with bullying. Children who can not properly self-regulate express their volatile emotions in a variety of ways, including screaming if they do not have their way, lashing out with their fists, throwing objects (such as chairs), or bullying other children. Such behaviours often elicit negative reactions from the social environment, which, in turn, can exacerbate or maintain the original regulation problems over time, a process termed cumulative continuity. These children are more likely to have conflict-based relationships with their teachers and other children. This can lead to more severe problems such as an impaired ability to adjust to school and predicts school dropout many years later. Children who fail to properly self-regulate grow as teenagers with more emerging problems. Their peers begin to notice this “immaturity”, and these children are often excluded from social groups and teased and harassed by their peers. This “immaturity” certainly causes some teenagers to become social outcasts in their respective social groups, causing them to lash out in angry and potentially violent ways. Being teased or being an outcast in childhood is especially damaging because it could lead to psychological symptoms such as depression and anxiety (in which dysregulated emotions play a central role), which, in turn, could lead to more peer victimisation. This is why it is recommended to foster emotional self-regulation in children as early as possible.
Occupational Therapy in Schools
Occupational therapists (OTs) are integrated educators in most public and private schools across the United States. They are trained in mental health and activity analysis to assess the needs of their clients. OTs and students work together to create meaningful and healthy habits for stress management, social skills, emotional labelling, coping strategies, awareness, problem-solving, self-monitoring, judgement, emotional control, and others in the school and home environment. OTs can complete formal assessments for emotional regulation and treat in a client-centred manner for each student. In addition, they can create individualised home programmes for carryover with their families. For example, OTs can work with students to engage in the occupational therapist-developed curriculum The Zones of Regulation, which utilises evidence-based knowledge, formal assessment, and in-classroom treatment to improve self-regulation of emotional behaviours and create long-lasting changes in habits.
Early childhood access to education on emotional regulation mitigates risk factors for increased anxiety, depression, and negative behaviours. It allows the student to create healthy habits for school and home environments. Children should be able to learn to regulate their feelings for full participation in activities, including social skills, play, sports, and school.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Emotional_self-regulation >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
In psychology, emotional detachment, also known as emotional blunting, is a condition or state in which a person lacks emotional connectivity to others, whether due to an unwanted circumstance or as a positive means to cope with anxiety.
Such a coping strategy, also known as emotion-focused coping, is used when avoiding certain situations that might trigger anxiety. It refers to the evasion of emotional connections. Emotional detachment may be a temporary reaction to a stressful situation, or a chronic condition such as depersonalisation–derealisation disorder. It may also be caused by certain antidepressants. Emotional blunting, also known as reduced affect display, is one of the negative symptoms of schizophrenia.
Signs and Symptoms
Emotional detachment may not be as outwardly obvious as other psychiatric symptoms. Patients diagnosed with emotional detachment have reduced ability to express emotion, to empathize with others or to form powerful emotional connections. Patients are also at an increased risk for many anxiety and stress disorders. This can lead to difficulties in creating and maintaining personal relationships. The person may move elsewhere in their mind and appear preoccupied or “not entirely present”, or they may seem fully present but exhibit purely intellectual behaviour when emotional behaviour would be appropriate. They may have a hard time being a loving family member, or they may avoid activities, places, and people associated with past traumas. Their dissociation can lead to lack of attention and, hence, to memory problems and in extreme cases, amnesia. In some cases, they present an extreme difficulty in giving or receiving empathy which can be related to the spectrum of narcissistic personality disorder. Additionally, emotional blunting is negatively correlated with remission quality. The negative symptoms are far less likely to disappear when a patient is experiencing emotional blunting.
In a study of children ages 4–12, traits of aggression and antisocial behaviours were found to be correlated with emotional detachment. Researchers determined that these could be early signs of emotional detachment, suggesting parents and clinicians to evaluate children with these traits for a higher behavioural problem in order to avoid bigger problems (such as emotional detachment) in the future.
A correlation was found of higher emotional blunting among patients treated with depression who scored higher on the Hospital Anxiety and Depression Scale (HADS) and were male (though the frequency difference was slight).
Emotional detachment in small amounts is normal. For example, being able to emotionally and psychologically detach from work when one is not in the workplace is a normal behaviour. Emotional detachment becomes an issue when it impairs a person’s ability to function on a day-to-day level.
Scales
While some depression severity scales provide insight to emotional blunting levels, many symptoms are not adequately covered. An attempt to resolve this issue is the Oxford Depression Questionnaire (ODQ), a scale specifically designed for full assessment of emotional blunting symptoms. The ODQ is designed specifically for patients with Major Depressive Disorder (MDD) in order to assess individual levels of emotional blunting.
Another scale, known as the Oxford Questionnaire on the Emotional Side-Effects of Antidepressants (OQESA), was developed using qualitative methods.
Causes
Emotional detachment and/or emotional blunting have multiple causes, as the cause can vary from person to person. Emotional detachment or emotional blunting often arises due to adverse childhood experiences, for example physical, sexual or emotional abuse. Emotional detachment is a maladaptive coping mechanism for trauma, especially in young children who have not developed coping mechanisms. Emotional detachments can also be due to psychological trauma in adulthood, like abuse, or traumatic experiences like war, automobile accidents etc.
Emotional blunting is often caused by antidepressants, in particular selective serotonin reuptake inhibitors (SSRIs) used in MDD and often as an add-on treatment in other psychiatric disorders. Individuals with MDD usually experience emotional blunting as well. Emotional blunting is a symptom of MDD, as depression is negatively correlated with emotional (both positive and negative) experiences.
Schizophrenia often occurs with negative symptoms, extrapyramidal signs (EPS), and depression. The latter overlaps with emotional blunting and is shown to be a core part of the present effects. Schizophrenia in general causes abnormalities in emotional understanding of individuals, all of which are clinically considered as an emotional blunting symptom. Individuals with schizophrenia show less emotional experiences, display less emotional expressions, and fail to recognize the emotional experiences and/or expressions of other individuals.
The changes in fronto-limbic activity in conjunction with depression succeeding a left hemisphere basal ganglia stroke (LBG stroke) may contribute to emotional blunting. LBG strokes are associated with depression and often caused by disorders of the basal ganglia (BG). Such disorders alter the emotional perception and experiences of the patient.
In many cases people with eating disorders (ED) show signs of emotional detachment. This is due to the fact that many of the circumstances that often lead to an ED are the same as the circumstances that lead to emotional detachment. For example, people with ED often have experienced childhood abuse. Eating disorders on their own are a maladaptive coping mechanism and to cope with the effects of an eating disorder, people may turn to emotional detachment.
Bereavement or losing a loved one can also be causes of emotional detachment.
Unfortunately, the prevalence of emotional blunting is not fully known.
Behavioural Mechanism
Emotional detachment is a maladaptive coping mechanism, which allows a person to react calmly to highly emotional circumstances. Emotional detachment in this sense is a decision to avoid engaging emotional connections, rather than an inability or difficulty in doing so, typically for personal, social, or other reasons. In this sense it can allow people to maintain boundaries, and avoid undesired impact by or upon others, related to emotional demands. As such it is a deliberate mental attitude which avoids engaging the emotions of others.
This detachment does not necessarily mean avoiding empathy; rather, it allows the person to rationally choose whether or not to be overwhelmed or manipulated by such feelings. Examples where this is used in a positive sense might include emotional boundary management, where a person avoids emotional levels of engagement related to people who are in some way emotionally overly demanding, such as difficult co-workers or relatives, or is adopted to aid the person in helping others.
Emotional detachment can also be “emotional numbing”, “emotional blunting”, i.e. dissociation, depersonalisation or in its chronic form depersonalisation disorder. This type of emotional numbing or blunting is a disconnection from emotion, it is frequently used as a coping survival skill during traumatic childhood events such as abuse or severe neglect. After continually using this coping mechanism, it can become a response to daily stresses.
Emotional detachment may allow acts of extreme cruelty and abuse, supported by the decision to not connect empathically with the person concerned. Social ostracism, such as shunning and parental alienation, are other examples where decisions to shut out a person creates a psychological trauma for the shunned party.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Emotional_detachment >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
The Brief Psychiatric Rating Scale (BPRS) is a rating scale which a clinician or researcher may use to measure psychiatric symptoms such as depression, anxiety, hallucinations and unusual behaviour.
The scale is one of the oldest, most widely used scales to measure psychotic symptoms and was first published in 1962.
Brief History
The BPRS was initially developed by John E. Overall and Donald R. Gorham. It was created for the purpose of being able to quickly assess the patient’s psychiatric symptoms prior, during, or following a treatment. The items of the test were generated from conducting factor analysis on the Multidimensional Scale for Rating Psychiatric Patients and the Inpatient Multidimensional Psychiatric Scale. Sixteen factors were found from the analysis, which served as the building blocks for the BPRS. Later research in 1968 added two more factors to the BPRS, which were excitement and disorientation.
Test Format
The BPRS consists of 18 items measuring the following factors:
It uses a seven-item Likert scale with the following values:
1 = “not present”.
2 = “very mild”.
3 = “mild”.
4 = “moderate”.
5 = “moderately severe”.
6 = “severe”.
7 = “extremely severe”.
The test is administered in tandem with a series of interviews conducted by at least two clinicians to ensure interrater reliability of the assessment.
Usage
The BPRS is intended for use on adult psychiatric patients and has been validated for use in elderly populations. A version designed for children called the Brief Psychiatric Rating Scale Children was also developed by Overall and Betty Pfeifferbaum, with different scale structures and factors.
Further Development
An expanded version of the test was created in 1993 by D. Lukoff, Keith H. Nuechterlein, and Joseph Ventura.
This page is based on the copyrighted Wikipedia article <https://en.wikipedia.org/wiki/Brief_Psychiatric_Rating_Scale>; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
In psychology, emotional detachment, also known as emotional blunting, has two meanings:
One is the inability to connect to others on an emotional level; and
The other is as a positive means of coping with anxiety.
This coping strategy, also known as emotion focused-coping, is used by avoiding certain situations that might trigger anxiety. It refers to the evasion of emotional connections. Emotional detachment may be a temporary reaction to a stressful situation, or a chronic condition such as depersonalisation-derealisation disorder. It may also be caused by certain antidepressants. Emotional blunting as reduced affect display is one of the negative symptoms of schizophrenia.
Signs and Symptoms
Emotional detachment may not be as outwardly obvious as other psychiatric symptoms. Patients diagnosed with emotional detachment have reduced ability to express emotion, to empathise with others or to form powerful emotional connections. Patients are also at an increased risk for many anxiety and stress disorders. This can lead to difficulties in creating and maintaining personal relationships. The person may move elsewhere in their mind and appear preoccupied or “not entirely present”, or they may seem fully present but exhibit purely intellectual behaviour when emotional behaviour would be appropriate. They may have a hard time being a loving family member, or they may avoid activities, places, and people associated with past traumas. Their dissociation can lead to lack of attention and, hence, to memory problems and in extreme cases, amnesia. In some cases, they present an extreme difficulty in giving or receiving empathy which can be related to the spectrum of narcissistic personality disorder.
In children (ages 4-12 were studied), traits of aggression and antisocial behaviours were found to be correlated with emotional detachment. Researchers determined that these could be early signs of emotional detachment, suggesting parents and clinicians to evaluate children with these traits for a higher behavioural problem in order to avoid bigger problems (such as emotional detachment) in the future.
Causes
Emotional detachment and/or emotional blunting have multiple causes, as the cause can vary from person to person. Emotional detachment or emotional blunting often arises due to adverse childhood experiences, or to psychological trauma in adulthood.
Emotional blunting is often caused by antidepressants in particular selective serotonin reuptake inhibitors (SSRIs) used in major depressive disorder, and often as an add-on treatment in other psychiatric disorders.
Behavioural Mechanism
Emotional detachment is a behaviour which allows a person to react calmly to highly emotional circumstances. Emotional detachment in this sense is a decision to avoid engaging emotional connections, rather than an inability or difficulty in doing so, typically for personal, social, or other reasons. In this sense it can allow people to maintain boundaries, psychic integrity and avoid undesired impact by or upon others, related to emotional demands. As such it is a deliberate mental attitude which avoids engaging the emotions of others.
This detachment does not necessarily mean avoiding empathy; rather, it allows the person to rationally choose whether or not to be overwhelmed or manipulated by such feelings. Examples where this is used in a positive sense might include emotional boundary management, where a person avoids emotional levels of engagement related to people who are in some way emotionally overly demanding, such as difficult co-workers or relatives, or is adopted to aid the person in helping others.
Emotional detachment can also be “emotional numbing”, “emotional blunting”, i.e., dissociation, depersonalisation or in its chronic form depersonalisation disorder. This type of emotional numbing or blunting is a disconnection from emotion, it is frequently used as a coping survival skill during traumatic childhood events such as abuse or severe neglect. Over time and with much use, this can become second nature when dealing with day to day stressors.
Emotional detachment may allow acts of extreme cruelty and abuse, supported by the decision to not connect empathically with the person concerned. Social ostracism, such as shunning and parental alienation, are other examples where decisions to shut out a person creates a psychological trauma for the shunned party.
Reduced affect display, sometimes referred to as emotional blunting, is a condition of reduced emotional reactivity in an individual.
It manifests as a failure to express feelings (affect display) either verbally or nonverbally, especially when talking about issues that would normally be expected to engage the emotions. Expressive gestures are rare and there is little animation in facial expression or vocal inflection. Reduced affect can be symptomatic of autism, schizophrenia, depression, posttraumatic stress disorder, depersonalisation disorder, schizoid personality disorder or brain damage. It may also be a side effect of certain medications (e.g. antipsychotics and antidepressants).
Reduced affect should be distinguished from apathy and anhedonia, which explicitly refer to a lack of emotion, whereas reduced affect is a lack of emotional expression (affect display) regardless of whether emotion (underlying affect) is actually reduced or not.
Types
Constricted Affect
A restricted or constricted affect is a reduction in an individual’s expressive range and the intensity of emotional responses.
Blunted and Flat Affect
Blunted affect is a lack of affect more severe than restricted or constricted affect, but less severe than flat or flattened affect. “The difference between flat and blunted affect is in degree. A person with flat affect has no or nearly no emotional expression. He or she may not react at all to circumstances that usually evoke strong emotions in others. A person with blunted affect, on the other hand, has a significantly reduced intensity in emotional expression”.
Shallow Affect
Shallow affect has equivalent meaning to blunted affect. Factor 1 of the Psychopathy Checklist identifies shallow affect as a common attribute of psychopathy.
Brain Structures
Individuals with schizophrenia with blunted affect show different regional brain activity in fMRI scans when presented with emotional stimuli compared to individuals with schizophrenia without blunted affect. Individuals with schizophrenia without blunted affect show activation in the following brain areas when shown emotionally negative pictures: midbrain, pons, anterior cingulate cortex, insula, ventrolateral orbitofrontal cortex, anterior temporal pole, amygdala, medial prefrontal cortex, and extrastriate visual cortex. Individuals with schizophrenia with blunted affect show activation in the following brain regions when shown emotionally negative pictures: midbrain, pons, anterior temporal pole, and extrastriate visual cortex.
Limbic Structures
Individuals with schizophrenia with flat affect show decreased activation in the limbic system when viewing emotional stimuli. In individuals with schizophrenia with blunted affect neural processes begin in the occipitotemporal region of the brain and go through the ventral visual pathway and the limbic structures until they reach the inferior frontal areas. Damage to the amygdala of adult rhesus macaques early in life can permanently alter affective processing. Lesioning the amygdala causes blunted affect responses to both positive and negative stimuli. This effect is irreversible in the rhesus macaques; neonatal damage produces the same effect as damage that occurs later in life. The macaques’ brain cannot compensate for early amygdala damage even though significant neuronal growth may occur. There is some evidence that blunted affect symptoms in schizophrenia patients are not a result of just amygdala responsiveness, but a result of the amygdala not being integrated with other areas of the brain associated with emotional processing, particularly in amygdala-prefrontal cortex coupling. Damage in the limbic region prevents the amygdala from correctly interpreting emotional stimuli in individuals with schizophrenia by compromising the link between the amygdala and other brain regions associated with emotion.
Brainstem
Parts of the brainstem are responsible for passive emotional coping strategies that are characterized by disengagement or withdrawal from the external environment (quiescence, immobility, hyporeactivity), similar to what is seen in blunted affect. Individuals with schizophrenia with blunted affect show activation of the brainstem during fMRI scans, particularly the right medulla and the left pons, when shown “sad” film excerpts. The bilateral midbrain is also activated in individuals with schizophrenia diagnosed with blunted affect. Activation of the midbrain is thought to be related to autonomic responses associated with perceptual processing of emotional stimuli. This region usually becomes activated in diverse emotional states. When the connectivity between the midbrain and the medial prefrontal cortex is compromised in individuals with schizophrenia with blunted affect an absence of emotional reaction to external stimuli results.
Prefrontal Cortex
Individuals with schizophrenia, as well as patients being successfully reconditioned with quetiapine for blunted affect, show activation of the prefrontal cortex (PFC). Failure to activate the PFC is possibly involved in impaired emotional processing in individuals with schizophrenia with blunted affect. The mesial PFC is activated in aver individuals in response to external emotional stimuli. This structure possibly receives information from the limbic structures to regulate emotional experiences and behaviour. Individuals being reconditioned with quetiapine, who show reduced symptoms, show activation in other areas of the PFC as well, including the right medial prefrontal gyrus and the left orbitofrontal gyrus.
Anterior Cingulate Cortex
A positive correlation has been found between activation of the anterior cingulate cortex and the reported magnitude of sad feelings evoked by viewing sad film excerpts. The rostral subdivision of this region is possibly involved in detecting emotional signals. This region is different in individuals with schizophrenia with blunted affect.
Diagnoses
Schizophrenia
Patients with schizophrenia have long been recognized as showing “flat or inappropriate affect, with splitting of feelings from events … feelings seem flat instead of being in contact with what is going on”. One study of flat affect in schizophrenia found that “flat affect was more common in men, and was associated with worse current quality of life” as well as having “an adverse effect on course of illness”.
The study also reported a “dissociation between reported experience of emotion and its display” – supporting the suggestion made elsewhere that “blunted affect, including flattened facial expressiveness and lack of vocal inflection … often disguises an individual’s true feelings.” Thus, feelings may merely be unexpressed, rather than totally lacking. On the other hand, “a lack of emotions which is due not to mere repression but to a real loss of contact with the objective world gives the observer a specific impression of ‘queerness’ … the remainders of emotions or the substitutes for emotions usually refer to rage and aggressiveness”. In the most extreme cases, there is a complete “dissociation from affective states”.
Another study found that when speaking, individuals with schizophrenia with flat affect demonstrate less inflection than normal controls and appear to be less fluent. Normal subjects appear to express themselves using more complex syntax, whereas flat affect subjects speak with fewer words, and fewer words per sentence. Flat affect individuals’ use of context-appropriate words in both sad and happy narratives are similar to that of controls. It is very likely that flat affect is a result of deficits in motor expression as opposed to emotional processing. The moods of display are compromised, but subjective, autonomic, and contextual aspects of emotion are left intact.
Post-Traumatic Stress Disorder
Post-traumatic stress disorder (PTSD) was previously known to cause negative feelings, such as depressed mood, re-experiencing and hyperarousal. However, recently, psychologists have started to focus their attention on the blunted affects and also the decrease in feeling and expressing positive emotions in PTSD patients. Blunted affect, or emotional numbness, is considered one of the consequences of PTSD because it causes a diminished interest in activities that produce pleasure (anhedonia) and produces feelings of detachment from others, restricted emotional expression and a reduced tendency to express emotions behaviourally. Blunted affect is often seen in veterans as a consequence of the psychological stressful experiences that caused PTSD. Blunted affect is a response to PTSD, it is considered one of the central symptoms in post-traumatic stress disorders and it is often seen in veterans who served in combat zones. In PTSD, blunted affect can be considered a psychological response to PTSD as a way to combat overwhelming anxiety that the patients feel. In blunted affect, there are abnormalities in circuits that also include the prefrontal cortex.
Assessment
In making assessments of mood and affect the clinician is cautioned that “it is important to keep in mind that demonstrative expression can be influenced by cultural differences, medication, or situational factors”; while the layperson is warned to beware of applying the criterion lightly to “friends, otherwise [he or she] is likely to make false judgments, in view of the prevalence of schizoid and cyclothymic personalities in our ‘normal’ population, and our [US] tendency to psychological hypochondriasis”.
R.D. Laing in particular stressed that “such ‘clinical’ categories as schizoid, autistic, ‘impoverished’ affect … all presuppose that there are reliable, valid impersonal criteria for making attributions about the other person’s relation to [his or her] actions. There are no such reliable or valid criteria”.
Differential Diagnosis
Blunted affect is very similar to anhedonia, which is the decrease or cessation of all feelings of pleasure (which thus affects enjoyment, happiness, fun, interest, and satisfaction). In the case of anhedonia, emotions relating to pleasure will not be expressed as much or at all because they are literally not experienced or are decreased. Both blunted affect and anhedonia are considered negative symptoms of schizophrenia, meaning that they are indicative of a lack of something. There are some other negative symptoms of schizophrenia which include avolition, alogia and catatonic behaviour.
Closely related is alexithymia – a condition describing people who “lack words for their feelings. They seem to lack feelings altogether, although this may actually be because of their inability to express emotion rather than from an absence of emotion altogether”. Alexithymic patients however can provide clues via assessment presentation which may be indicative of emotional arousal.
“If the amygdala is severed from the rest of the brain, the result is a striking inability to gauge the emotional significance of events; this condition is sometimes called ‘affective blindness'”. In some cases, blunted affect can fade, but there is no conclusive evidence of why this can occur.
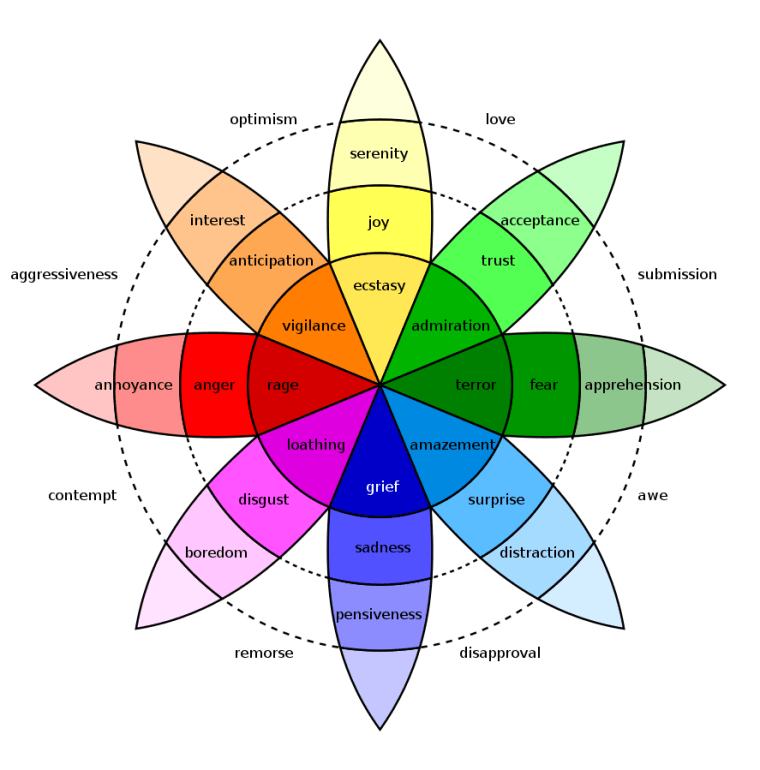



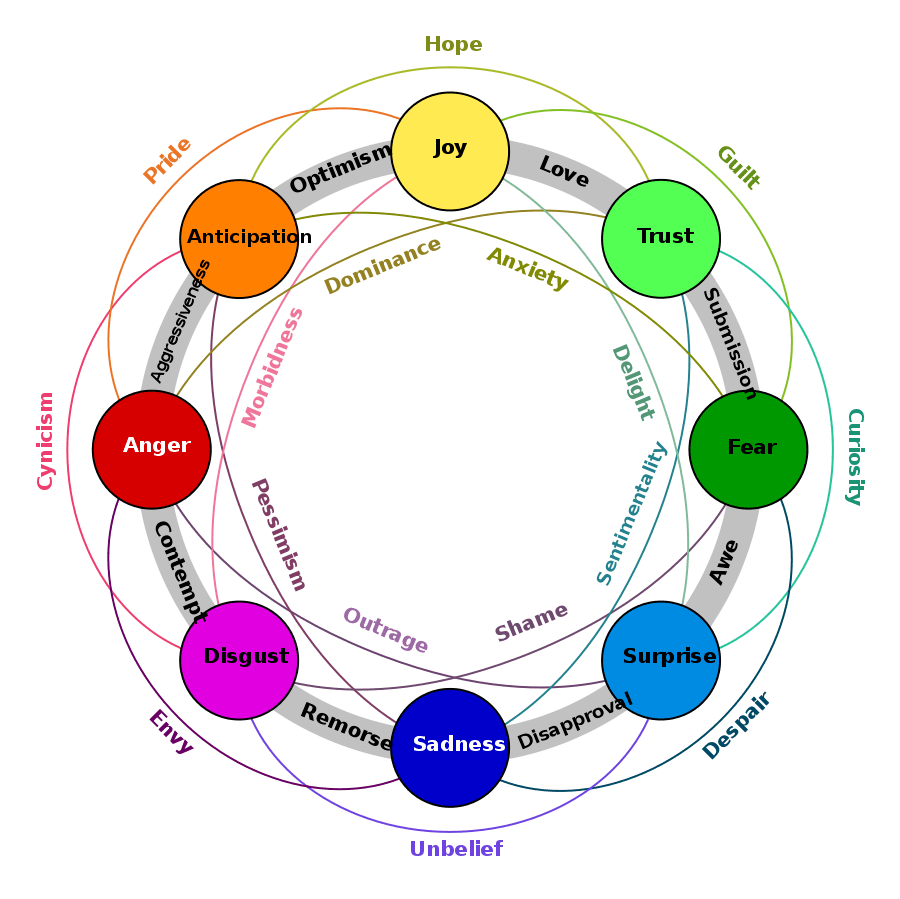

You must be logged in to post a comment.