Ole Ivar Løvaas (08 May 1927 to 02 August 2010) was a Norwegian-American clinical psychologist and professor at the University of California, Los Angeles. He is most well known for his research on what is now called applied behaviour analysis (ABA) to teach autistic children through prompts, modelling, and positive reinforcement. The therapy is also noted for its use of aversives (punishment) to reduce undesired behaviour.
Løvaas founded the Lovaas Institute and co-founded the Autism Society of America. He is also considered a pioneer of ABA due to his development of discrete trial training and early intensive behavioural intervention for autistic children.
His work influenced how autism is treated, and Løvaas received widespread acclaim and several awards during his lifetime.
Personal Life
Løvaas was born in Lier, Norway on 08 May 1927 to Hildur and Ernst Albert Løvaas. He had two siblings: an older sister named Nora and a younger brother named Hans Erik. Løvaas attended Hegg Elementary School in Lier from 1934 to 1941. He attended junior high school at Drammen Realskole until 1944, and then moved on to Drammen Latin School for high school, graduating in 1947.
Following World War II, Løvaas moved to the United States. There he married Beryl Scoles in 1955, and together they had four children. Lovaas later divorced his wife and remarried Nina Watthen in 1986.
Career
After graduating from high school, Løvaas served in the Norwegian Air Force for 18 months. He was a forced farm worker during the 1940s Nazi occupation of Norway, and often said that observing the Nazis had sparked his interest in human behaviour.
He attended Luther College in Decorah, Iowa, graduating in 1951 after just one year with his B.A. in sociology. Løvaas received his Masters of Science in clinical psychology from the University of Washington in 1955, and his PhD in learning and clinical psychology from the same school 3 years later.
Early in his career, Løvaas worked at the Pinel foundation, which focused on Freudianpsychoanalysis. After earning his PhD, he took a position at the University of Washington’s Child Development Institute, where he first learned of behaviour analysis. Løvaas began teaching at UCLA in 1961 in the Department of Psychology, where he performed research on children with autism spectrum disorder at the school’s Neuropsychiatric Institute. He started an early intervention clinic at UCLA called the UCLA Young Autism Project, which provided intensive intervention inside the children’s homes. He was named professor emeritus in 1994. Løvaas also established the Lovaas Institute for Early Intervention (LIFE) that provides interventions based on his research.
Løvaas taught now prominent behaviourists, such as Robert Koegel, Laura Schreibman, Tristram Smith, Doreen Granpeesheh, John McEachin, Ron Leaf, Jacquie Wynn, and thousands of UCLA students who took his “Behaviour Modification” course during his 50 years of teaching. He also co-founded what is today the Autism Society of America (ASA), published hundreds of research articles and several books, and received many accolades for his research. Due to this research, a number of school districts have adopted his programmes. His work influenced how autism is treated.
Research
Autism Intervention
Early Research
Løvaas established the Young Autism Project clinic at UCLA in 1962, where he began his research, authored training manuals, and recorded tapes of him and his graduate students implementing errorless learning—based on operant conditioning and what was then referred to as behaviour modification—to instruct autistic children. He later coined the term “discrete trial training” to describe the procedure, which was used to teach listener responding, eye contact, fine and gross motor imitation, receptive and expressive language, academic, and a variety of other skills. In an errorless discrete trial, the child sits at a table across from the therapist who provides an instruction (i.e. “do this”, “look at me”, “point to”, etc.), followed by a prompt, then the child’s response, and a stimulus reinforcer. The prompts are later discontinued once the child demonstrates proficiency. During this time, Løvaas and colleagues also employed physical aversives (punishment), such as electric shocks and slaps, to decrease aggressive and self-injurious behaviour, as well as verbal reprimands if the child answered incorrectly or engaged in self-stimulatory behaviour.
1987 Study
In 1987, Løvaas published a study which demonstrated that, following forty hours a week of treatment, 9 of the 19 autistic children developed typical spoken language, increased IQs by 30 points on average, and were placed in regular classrooms. A 1993 follow-up study found that 8 maintained their gains and were “indistinguishable from their typically developing peers”, scoring in the normal range of social and emotional functioning. His studies were limited because Løvaas did not randomise the participants or treatment groups. This produced a quasi-experiment in which he was able to control the assignment of children to treatment groups. His manipulation of the study in this way may have been responsible for the observed effects. The true efficacy of his method cannot be determined since his studies cannot be repeated for ethical reasons. A 1998 study subsequently recommended that EIBI programmes be regarded with scepticism. In 1999, the United States Surgeon General’s office wrote:
“Thirty years of research has demonstrated the efficacy of applied behavioral methods in reducing inappropriate behavior and in increasing communication, learning, and appropriate social behavior”, and he also endorsed the 1987 study.
Literature Reviews
According to a 2007 review study in Paediatrics:
“The effectiveness of [EIBI] in [autism spectrum disorder] has been well-documented through 5 decades of research by using single-subject methodology and in controlled studies… in university and community settings.”
It further stated:
“Children who receive early intensive behavioral treatment have been shown to make substantial, sustained gains in IQ, language, academic performance, and adaptive behavior as well as some measures of social behavior, and their outcomes have been significantly better than those of children in control groups.”
However, the study also recommended to later generalise the child’s skills with more naturalistic ABA-based procedures, such as incidental teaching and pivotal response treatment, so their progress is maintained.
Another review in 2008 described DTT as a “‘well-established’ psychosocial intervention for improving the intellectual performance of young children with autism spectrum disorders…” In 2011, it was found that the intervention is effective for some, but “the literature is limited by methodological concerns” due to there being small sample sizes and very few studies that used random assignment, and a 2018 Cochrane review subsequently indicated low-quality evidence to support this method. Nonetheless, a meta-analysis in the same journal database concludes how some recent research is beginning to suggest that because of the heterology of ASD, there are a wide range of different learning styles and that it is the children with lower receptive language skills who acquire spoken language from Løvaas’ treatment. In 2023, a multi-site randomised control trial study of 164 participants indicated similar findings.
UCLA Feminine Boy Project
Løvaas co-authored a study with George Rekers in 1974 where they attempted to modify the behavior of feminine male children through the use of rewards and punishment with the goal of preventing them from becoming adult transsexuals. The subject of the first of these studies, a young boy at the age of 4 at the inception of the experiment, died by suicide as an adult in 2003; his family attribute the suicide to this treatment. Despite the follow-up study (which Løvaas was not involved in) writing that the therapy successfully converted his homosexuality, his sister expressed concerns that it was overly biased as “he was conditioned to say that”, and she read his journal, which described how he feared disclosing his sexual orientation due to his father spanking him as a child as punishment for engaging in feminine behaviour, such as playing with dolls.
In October 2020, the Journal of Applied Behaviour Analysis officially issued an Expression of Concern about the Rekers and Løvaas study. In the editorial accompanying the Expression of Concern, the journal discusses the damage done by the study. It emphasizes that the study inflicted personal harm upon the study’s subject and his family, as well as to the gay community, for inappropriately promoting the study as evidence that conversion therapy is effective. It also argues that the field of behaviour analysis was harmed by the false portrayal that the study and the use of conversion therapy are currently representative of the field.
Awards and Accolades
Løvaas received praise from several organisations during his lifetime. In 2001, he was given the Society of Clinical Child and Adolescent Psychology Distinguished Career Award. He received the Edgar Doll Award from the 33rd Division of the American Psychological Association, the Lifetime Research Achievement Award from the 55th Division of the American Psychological Association, and the Award for Effective Presentation of Behaviour Analysis in the Mass Media by the Association for Behaviour Analysis International. Løvaas also earned a Guggenheim fellowship and the California Senate Award, which is an honorary doctorate. He was named a Fellow by Division 7 of the American Psychological Association and was given the Champion of Mental Health Award by Psychology Today.
Criticism
The goal of making autistic people indistinguishable from their peers has attracted significant backlash from autistic advocates. Julia Bascom of the Autistic Self Advocacy Network (ASAN) has said:
“ASAN’s objection is fundamentally an ethical one. The stated end goal of ABA is an autistic child who is ‘indistinguishable from their peers’ – an autistic child who can pass as neurotypical. We don’t think that’s an acceptable goal. The end goal of all services, supports, interventions, and therapies an autistic child receives should be to support them in growing up into an autistic adult who is happy, healthy, and living a self-determined life.”
Løvaas has also been criticised for his view of autistic people in relation to other people, as he said in a statement during an interview:
“You start pretty much from scratch when you work with an autistic person. You have a person in the physical sense – they have hair, a nose, a mouth – but they are not people in the psychological sense.”
Aversives
Løvaas is credited with popularising the use of aversives in behaviour modification, as shown in a Life magazine photo spread in 1965.
He later admitted that they were only temporarily effective and punishments became less effective over time. Eventually, Løvaas abandoned these tactics, telling CBS in a 1994 interview:
“These people are so used to pain that they can adapt to almost any kind of aversive you give them.”
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Ole_Ivar_Lovaas >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Social exclusion or social marginalisation is the social disadvantage and relegation to the fringe of society. It is a term that has been used widely in Europe and was first used in France in the late 20th century. In the EU context, the European Commission defines it as “a situation whereby a person is prevented (or excluded) from contributing to and benefiting from economic and social progress”. It is used across disciplines including education, sociology, psychology, healthcare, politics and economics.
Social exclusion is the process in which individuals are blocked from (or denied full access to) various rights, opportunities and resources that are normally available to members of a different group, and which are fundamental to social integration and observance of human rights within that particular group] (e.g. due process).
Alienation or disenfranchisement resulting from social exclusion can be connected to a person’s social class, race, skin colour, religious affiliation, ethnic origin, caste, educational status, childhood relationships, living standards, and or political opinions, and appearance. Such exclusionary forms of discrimination may also apply to disabled people, minorities, LGBTQ+ people, drug users, institutional care leavers, the elderly and the young. Anyone who appears to deviate in any way from perceived norms of a population may thereby become subject to coarse or subtle forms of social exclusion.
The outcome of social exclusion is that affected individuals or communities are prevented from participating fully in the economic, social, and political life of the society in which they live. This may result in resistance in the form of demonstrations, protests or lobbying from the excluded people.
The concept of social exclusion has led to the researcher’s conclusion that in many European countries the impact of social disadvantages, that influence the well-being of all people, including with special needs, has an increasingly negative impact.
Most of the characteristics listed in this article are present together in studies of social exclusion, due to exclusion’s multidimensionality.
Another way of articulating the definition of social exclusion is as follows:
Social exclusion is a multidimensional process of progressive social rupture, detaching groups and individuals from social relations and institutions and preventing them from full participation in the normal, normatively prescribed activities of the society in which they live.
In an alternative conceptualization, social exclusion theoretically emerges at the individual or group level on four correlated dimensions:
Insufficient access to social rights;
Material deprivation;
Limited social participation; and
A lack of normative integration.
It is then regarded as the combined result of:
Personal risk factors (age, gender, race);
Macro-societal changes (demographic, economic and labour market developments, technological innovation, the evolution of social norms);
Government legislation and social policy; and
The actual behaviour of businesses, administrative organisations and fellow citizens.
Individual Exclusion
“The marginal man…is one whom fate has condemned to live in two societies and in two, not merely different but antagonistic cultures….his mind is the crucible in which two different and refractory cultures may be said to melt and, either wholly or in part, fuse.”
Social exclusion at the individual level results in an individual’s exclusion from meaningful participation in society. An example is the exclusion of single mothers from the welfare system prior to welfare reforms of the 1900s. The modern welfare system is based on the concept of entitlement to the basic means of being a productive member of society both as an organic function of society and as compensation for the socially useful labour provided. A single mother’s contribution to society is not based on formal employment, but on the notion that provision of welfare for children is a necessary social expense. In some career contexts, caring work is devalued and motherhood is seen as a barrier to employment. Single mothers were previously marginalised in spite of their significant role in the socializing of children due to views that an individual can only contribute meaningfully to society through “gainful” employment as well as a cultural bias against unwed mothers. When the father’s sole task was seen as the breadwinner, his marginalisation was primarily a function of class condition. Solo fatherhood brings additional trials due to society being less accepting of males ‘getting away with’ not working and the general invisibility/lack of acknowledgment of single fathers in society. Acknowledgment of the needs participatory fathers may have can be found by examining the changes from the original clinical report on the father’s role published by the American Academy of Paediatrics in May 2004. Eight week paternity leave is a good example of one social change. Child health care providers have an opportunity to have a greater influence on the child and family structure by supporting fathers and enhancing a father’s involvement.
More broadly, many women face social exclusion. Moosa-Mitha discusses the Western feminist movement as a direct reaction to the marginalisation of white women in society. Women were excluded from the labour force and their work in the home was not valued. Feminists argued that men and women should equally participate in the labour force, in the public and private sector, and in the home. They also focused on labour laws to increase access to employment as well as to recognise child-rearing as a valuable form of labour. In some places today, women are still marginalised from executive positions and continue to earn less than men in upper management positions.
Another example of individual marginalisation is the exclusion of individuals with disabilities from the labour force. Grandz discusses an employer’s viewpoint about hiring individuals living with disabilities as jeopardising productivity, increasing the rate of absenteeism, and creating more accidents in the workplace. Cantor also discusses employer concern about the excessively high cost of accommodating people with disabilities. The marginalisation of individuals with disabilities is prevalent today, despite the legislation intended to prevent it in most western countries, and the academic achievements, skills and training of many disabled people.
There are also exclusions of sexual minorities because of their sexual orientation, gender identity, and/or sexual characteristics. The Yogyakarta Principles require that the states and communities abolish any stereotypes about LGBT people as well as stereotyped gender roles.
“Isolation is common to almost every vocational, religious or cultural group of a large city. Each develops its own sentiments, attitudes, codes, even its own words, which are at best only partially intelligible to others.”
Community Exclusion
Many communities experience social exclusion, such as racial (e.g. black), caste (e.g. untouchables or dalits in some regions in India), and economic (e.g. Romani) communities.
One example is the Aboriginal community in Australia. The marginalisation of Aboriginal communities is a product of colonisation. As a result of colonialism, Aboriginal communities lost their land, were forced into destitute areas, lost their sources of livelihood, were excluded from the labour market and were subjected to widespread unpunished massacres. Additionally, Aboriginal communities lost their culture and values through forced assimilation and lost their rights in society. Today, various Aboriginal communities continue to be marginalised from society due to the development of practices, policies and programs that, according to J. Yee, “met the needs of white people and not the needs of the marginalized groups themselves”. Yee also connects marginalisation to minority communities, when describing the concept of whiteness as maintaining and enforcing dominant norms and discourse. Poor people living in run-down council estates and areas with high crime can be locked into social deprivation
Contributors
Social exclusion has many contributors. Major contributors include race, income, employment status, social class, geographic location; personal habits, appearance, or interests (i.e. a favourite hobby, sports team, or music genre); education, religion, and political affiliation.
Global and Structural
Globalisation (global capitalism), immigration, social welfare, and policy are broader social structures that have the potential to contribute negatively to one’s access to resources and services, resulting in the social exclusion of individuals and groups. Similarly, increasing use of information technology and the company outsourcing have contributed to job insecurity and a widening gap between the rich and the poor. Flobalisation sets forth a decrease in the role of the state with an increase in support from various “corporate sectors resulting in gross inequalities, injustices and marginalization of various vulnerable groups”. Companies are outsourcing, jobs are lost, the cost of living continues to rise, and the land is being expropriated by large companies. Material goods are made in large abundances and sold at cheaper costs, while in India for example, the poverty line is lowered in order to mask the number of individuals who are actually living in poverty as a result of globalization. Globalization and structural forces aggravate poverty and continue to push individuals to the margins of society, while governments and large corporations do not address the issues (George, P, SK8101, lecture, 09 October 2007).
Certain language and the meaning attached to language can cause universalising discourses that are influenced by the Western world, which is what Sewpaul (2006) describes as the “potential to dilute or even annihilate local cultures and traditions and to deny context-specific realities” (p. 421). What Sewpaul (2006) is implying is that the effect of dominant global discourses can cause individual and cultural displacement, as well as sex safety are jeopardised (p. 422). Insecurity and fear of an unknown future and instability can result in displacement, exclusion, and forced assimilation into the dominant group. For many, it further pushes them to the margins of society or enlists new members to the outskirts because of global-capitalism and dominant discourses (Sewpaul, 2006).
With the prevailing notion of globalisation, we now see the rise of immigration as the world gets smaller and smaller with millions of individuals relocating each year. This is not without hardship and struggle of what a newcomer thought was going to be a new life with new opportunities. Immigration has had a strong link to the access of welfare support programmes. Newcomers are constantly bombarded with the inability to access a country’s resources because they are seen as “undeserving foreigners” (p. 132). With this comes a denial of access to public housing, health care benefits, employment support services, and social security benefits. Newcomers are seen as undeserving, or that they must prove their entitlement in order to gain access to basic support necessities. It is clear that individuals are exploited and marginalised within the country they have emigrated.
Welfare states and social policies can also exclude individuals from basic necessities and support programmes. Welfare payments were proposed to assist individuals in accessing a small amount of material wealth (Young, 2000). Young (2000) further discusses how “the provision of the welfare itself produces new injustice by depriving those dependent on it of rights and freedoms that others have…marginalization is unjust because it blocks the opportunity to exercise capacities in socially defined and recognized way” (p. 41). There is the notion that by providing a minimal amount of welfare support, an individual will be free from marginalisation. In fact, welfare support programmes further lead to injustices by restricting certain behaviour, as well the individual is mandated to other agencies. The individual is forced into a new system of rules while facing social stigma and stereotypes from the dominant group in society, further marginalising and excluding individuals (Young, 2000). Thus, social policy and welfare provisions reflect the dominant notions in society by constructing and reinforcing categories of people and their needs. It ignores the unique-subjective human essence, further continuing the cycle of dominance.
Unemployment
Whilst recognising the multi-dimensionality of exclusion, policy work undertaken in the EU focused on unemployment as a key cause of, or at least correlating with, social exclusion. This is because, in modern societies, paid work is not only the principal source of income with which to buy services but is also the fount of individuals’ identity and feeling of self-worth. Most people’s social networks and a sense of embeddedness in society also revolve around their work. Many of the indicators of extreme social exclusion, such as poverty and homelessness, depend on monetary income which is normally derived from work. Social exclusion can be a possible result of long-term unemployment, especially in countries with weak welfare safety nets. Much policy to reduce exclusion thus focuses on the labour market:
On the one hand, to make individuals at risk of exclusion more attractive to employers, i.e. more “employable”.
On the other hand, to encourage (and/or oblige) employers to be more inclusive in their employment policies.
The EU’s EQUAL Community Initiative investigated ways to increase the inclusiveness of the labour market. Work on social exclusion more broadly is carried out through the Open Method of Coordination (OMC) among the Member State governments. The United Nations Sustainable Development Goal 10 is also an example of global initiatives aimed at promoting social inclusion for all by 2030.
Religion
Some religious traditions recommend excommunication of individuals said to deviate from religious teaching, and in some instances shunning by family members. Some religious organisations permit the censure of critics.
Across societies, individuals and communities can be socially excluded on the basis of their religious beliefs. Social hostility against religious minorities and communal violence occur in areas where governments do not have policies restricting the religious practise of minorities. A study by the Pew Research Centre on international religious freedom found that 61% of countries have social hostilities that tend to target religious minorities. The five highest social hostility scores were for Pakistan, India, Sri Lanka, Iraq, and Bangladesh. In 2015, Pew published that social hostilities declined in 2013, but harassment of Jews increased.
Sport
Parts of 2024 Summer Olympics opening ceremony have been criticised by some as divisive due to singling out one particular religion (Christianity).
Consequences
Health
In gay men, results of psycho-emotional damage from marginalisation from a heteronormative society include suicide and drug addiction.
Scientists have been studying the impact of racism on health. Amani Nuru-Jeter, a social epidemiologist at the University of California, Berkeley and other doctors have been hypothesizing that exposure to chronic stress may be one way racism contributes to health disparities between racial groups. Arline Geronimus, a research professor at the University of Michigan Institute for Social Research and a professor at the School of Public Health, and her colleagues found that psychosocial stress associated with living in extreme poverty can cause early onset of age-related diseases. The 2015 study titled, “Race-Ethnicity, Poverty, Urban Stressors, and Telomere Length in a Detroit Community-based Sample” was conducted in order to determine the impact of living conditions on health and was performed by a multi-university team of social scientists, cellular biologists and community partners, including the Healthy Environments Partnership (HEP) to measure the telomere length of poor and moderate-income people of White, African-American and Mexican race.
In 2006, there was research focused on possible connections between exclusion and brain function. Studies published by both the University of Georgia and San Diego State University found that exclusion can lead to diminished brain functioning and poor decision making. Such studies corroborate with earlier beliefs of sociologists. The effect of social exclusion have been hypothesized in various past research studies to correlate with such things as substance abuse and addiction, and crime.
Economics
The problem of social exclusion is usually tied to that of equal opportunity, as some people are more subject to such exclusion than others. Marginalisation of certain groups is a problem in many economically more developed countries where the majority of the population enjoys considerable economic and social opportunities.
In Philosophy
The marginal, the processes of marginalisation, etc. bring specific interest in postmodern and post-colonial philosophy and social studies. Postmodernism question the “centre” about its authenticity and postmodern sociology and cultural studies research marginal cultures, behaviours, societies, the situation of the marginalised individual, etc.
Social Inclusion
Social inclusion is the converse of social exclusion. As the World Bank states, social inclusion is the process of improving the ability, opportunity, and worthiness of people, disadvantaged on the basis of their identity, to take part in society. The World Bank’s 2019 World Development Report on The Changing Nature of Work suggests that enhanced social protection and better investments in human capital improve equality of opportunity and social inclusion. Social inclusion can be measured individually.
Social Inclusion ministers have been appointed, and special units established, in a number of jurisdictions around the world. The first Minister for Social Inclusion was Premier of South Australia Mike Rann, who took the portfolio in 2004. Based on the UK’s Social Exclusion Unit, established by Prime Minister Tony Blair in 1997, Rann established the Social Inclusion Initiative in 2002. It was headed by Monsignor David Cappo and was serviced by a unit within the department of Premier and Cabinet. Cappo sat on the executive committee of the South Australian Cabinet and was later appointed Social Inclusion Commissioner with wide powers to address social disadvantage. Cappo was allowed to roam across agencies given that most social disadvantage has multiple causes necessitating a “joined up” rather than a single agency response.[48] The Initiative drove a big investment by the South Australian Government in strategies to combat homelessness, including establishing Common Ground, building high quality inner city apartments for “rough sleeping” homeless people, the Street to Home initiative and the ICAN flexible learning program designed to improve school retention rates. It also included major funding to revamp mental health services following Cappo’s “Stepping Up” report, which focused on the need for community and intermediate levels of care and an overhaul of disability services. In 2007, the then Australian Prime Minister Kevin Rudd appointed Julia Gillard as the nation’s first Social Inclusion Minister.
In Japan, the concept and term “social inclusion” went through a number of changes over time and eventually became incorporated in community-based activities under the names hōsetsu (包摂) and hōkatsu (包括), such as in the “Community General Support Centres” (chiiki hōkatsu shien sentā 地域包括支援センター) and “Community-based Integrated Care System” (chiiki hōkatsu kea shisutemu 地域包括ケアシステム).[53]
One may explore its implications for social work practice. Mullaly (2007) describes how “the personal is political” and the need for recognising that social problems are indeed connected with larger structures in society, causing various forms of oppression amongst individuals resulting in marginalisation. It is also important for the social worker to recognise the intersecting nature of oppression. A non-judgmental and unbiased attitude is necessary on the part of the social worker. The worker may begin to understand oppression and marginalisation as a systemic problem, not the fault of the individual.
Working under an anti-oppression perspective would then allow the social worker to understand the lived, subjective experiences of the individual, as well as their cultural, historical and social background. The worker should recognize the individual as political in the process of becoming a valuable member of society and the structural factors that contribute to oppression and marginalisation (Mullaly, 2007). Social workers must take a firm stance on naming and labelling global forces that impact individuals and communities who are then left with no support, leading to marginalisation or further marginalisation from the society they once knew (George, P, SK8101, lecture, 09 October 2007).
The social worker should be constantly reflexive, work to raise the consciousness, empower, and understand the lived subjective realities of individuals living in a fast-paced world, where fear and insecurity constantly subjugate the individual from the collective whole, perpetuating the dominant forces, while silencing the oppressed.
Some individuals and groups who are not professional social workers build relationships with marginalised persons by providing relational care and support, for example, through homeless ministry. These relationships validate the individuals who are marginalised and provide them a meaningful contact with the mainstream.
In Law
There are countries, Italy for example, that have a legal concept of social exclusion. In Italy, “esclusione sociale” is defined as poverty combined with social alienation, by the statute n. 328 (11-8-2000), that instituted a state investigation commission named “Commissione di indagine sull’Esclusione Sociale” (CIES) to make an annual report to the government on legally expected issues of social exclusion.
The Vienna Declaration and Programme of Action, a document on international human rights instruments affirms that:
“extreme poverty and social exclusion constitute a violation of human dignity and that urgent steps are necessary to achieve better knowledge of extreme poverty and its causes, including those related to the program of development, in order to promote the human rights of the poorest, and to put an end to extreme poverty and social exclusion and promote the enjoyment of the fruits of social progress. It is essential for States to foster participation by the poorest people in the decision making process by the community in which they live, the promotion of human rights and efforts to combat extreme poverty.”
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Social_exclusion >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
The self-regulation of emotion or emotion regulation is the ability to respond to the ongoing demands of experience with the range of emotions in a manner that is socially tolerable and sufficiently flexible to permit spontaneous reactions as well as the ability to delay spontaneous reactions as needed. It can also be defined as extrinsic and intrinsic processes responsible for monitoring, evaluating, and modifying emotional reactions. The self-regulation of emotion belongs to the broader set of emotion regulation processes, which includes both the regulation of one’s own feelings and the regulation of other people’s feelings.
Plutchik WheelPlutchik Dyads
Emotion regulation is a complex process that involves initiating, inhibiting, or modulating one’s state or behaviour in a given situation — for example, the subjective experience (feelings), cognitive responses (thoughts), emotion-related physiological responses (for example heart rate or hormonal activity), and emotion-related behaviour (bodily actions or expressions). Functionally, emotion regulation can also refer to processes such as the tendency to focus one’s attention to a task and the ability to suppress inappropriate behaviour under instruction. Emotion regulation is a highly significant function in human life.
Every day, people are continually exposed to a wide variety of potentially arousing stimuli. Inappropriate, extreme or unchecked emotional reactions to such stimuli could impede functional fit within society; therefore, people must engage in some form of emotion regulation almost all of the time. Generally speaking, emotion dysregulation has been defined as difficulties in controlling the influence of emotional arousal on the organisation and quality of thoughts, actions, and interactions. Individuals who are emotionally dysregulated exhibit patterns of responding in which there is a mismatch between their goals, responses, and/or modes of expression, and the demands of the social environment. For example, there is a significant association between emotion dysregulation and symptoms of depression, anxiety, eating pathology, and substance abuse. Higher levels of emotion regulation are likely to be related to both high levels of social competence and the expression of socially appropriate emotions.
Theory
Process Model
The process model of emotion regulation is based upon the modal model of emotion. The modal model of emotion suggests that the emotion generation process occurs in a particular sequence over time. This sequence occurs as follows:
Situation: the sequence begins with a situation (real or imagined) that is emotionally relevant.
Attention: attention is directed towards the emotional situation.
Appraisal: the emotional situation is evaluated and interpreted.
Response: an emotional response is generated, giving rise to loosely coordinated changes in experiential, behavioural, and physiological response systems.
Because an emotional response (4.) can cause changes to a situation (1.), this model involves a feedback loop from (4.) Response to (1.) Situation. This feedback loop suggests that the emotion generation process can occur recursively, is ongoing, and dynamic.
The process model contends that each of these four points in the emotion generation process can be subjected to regulation. From this conceptualization, the process model posits five different families of emotion regulation that correspond to the regulation of a particular point in the emotion generation process. They occur in the following order:
Situation selection
Situation modification
Attentional deployment
Cognitive change
Response modulation
The process model also divides these emotion regulation strategies into two categories: antecedent-focused and response-focused. Antecedent-focused strategies (i.e. situation selection, situation modification, attentional deployment, and cognitive change) occur before an emotional response is fully generated. Response-focused strategies (i.e. response modulation) occur after an emotional response is fully generated.
Strategies
Situation Selection
Situation selection is an emotional regulation strategy that involves choosing to avoid or approach a future emotional situation. If a person selects to avoid or disengage from an emotionally relevant situation, they are decreasing the likelihood of experiencing an emotion. Alternatively, if a person selects to approach or engage with an emotionally relevant situation, they are increasing the likelihood of experiencing an emotion.
Typical examples of situation selection may be seen interpersonally, such as when a parent removes his or her child from an emotionally unpleasant situation. Use of situation selection may also be seen in psychopathology. For example, avoidance of social situations to regulate emotions is particularly pronounced for those with social anxiety disorder and avoidant personality disorder.
Effective situation selection is not always an easy task. For instance, humans display difficulties predicting their emotional responses to future events. Therefore, they may have trouble making accurate and appropriate decisions about which emotionally relevant situations to approach or to avoid.
Situation Modification
Situation modification involves efforts to modify a situation so as to change its emotional impact. Situation modification refers specifically to altering one’s external, physical environment. Altering one’s “internal” environment to regulate emotion is called cognitive change.
Examples of situation modification may include injecting humour into a speech to elicit laughter or extending the physical distance between oneself and another person.
Attentional Deployment
Attentional deployment involves directing one’s attention towards or away from an emotional situation.
Distraction
Distraction, an example of attentional deployment, is an early selection strategy, which involves diverting one’s attention away from an emotional stimulus and towards other content. Distraction has been shown to reduce the intensity of painful and emotional experiences, to decrease facial responding and neural activation in the amygdala associated with emotion, as well as to alleviate emotional distress. As opposed to reappraisal, individuals show a relative preference to engage in distraction when facing stimuli of high negative emotional intensity. This is because distraction easily filters out high-intensity emotional content, which would otherwise be relatively difficult to appraise and process.
Rumination
Rumination, an example of attentional deployment, is defined as the passive and repetitive focusing of one’s attention on one’s symptoms of distress and the causes and consequences of these symptoms. Rumination is generally considered a maladaptive emotion regulation strategy, as it tends to exacerbate emotional distress. It has also been implicated in a host of disorders including major depression.
Worry
Worry, an example of attentional deployment, involves directing attention to thoughts and images concerned with potentially negative events in the future. By focusing on these events, worrying serves to aid in the down-regulation of intense negative emotion and physiological activity. While worry may sometimes involve problem solving, incessant worry is generally considered maladaptive, being a common feature of anxiety disorders, particularly generalised anxiety disorder.
Thought Suppression
Thought suppression, an example of attentional deployment, involves efforts to redirect one’s attention from specific thoughts and mental images to other content so as to modify one’s emotional state. Although thought suppression may provide temporary relief from undesirable thoughts, it may ironically end up spurring the production of even more unwanted thoughts. This strategy is generally considered maladaptive, being most associated with obsessive-compulsive disorder.
Cognitive Change
Cognitive change involves changing how one appraises a situation so as to alter its emotional meaning.
Reappraisal
Reappraisal, an example of cognitive change, is a late selection strategy, which involves a change of the meaning of an event that alters its emotional impact. It encompasses different sub-strategies, such as positive reappraisal (creating and focusing on a positive aspect of the stimulus), decentring (reinterpreting an event by broadening one’s perspective to see “the bigger picture”), or fictional reappraisal (adopting or emphasizing the belief that event is not real, that it is for instance “just a movie” or “just my imagination”). Reappraisal has been shown to effectively reduce physiological, subjective, and neural emotional responding. As opposed to distraction, individuals show a relative preference to engage in reappraisal when facing stimuli of low negative emotional intensity because these stimuli are relatively easy to appraise and process.
Reappraisal is generally considered to be an adaptive emotion regulation strategy. Compared to suppression (including both thought suppression and expressive suppression), which is positively correlated with many psychological disorders, reappraisal can be associated with better interpersonal outcomes, and can be positively related to well-being. However, some researchers argue that context is important when evaluating the adaptiveness of a strategy, suggesting that in some contexts reappraisal may be maladaptive. Furthermore, some research has shown reappraisal does not influence or affect physiological responses to recurrent stress.
Distancing
Distancing, an example of cognitive change, involves taking on an independent, third-person perspective when evaluating an emotional event. Distancing has been shown to be an adaptive form of self-reflection, facilitating the emotional processing of negatively valenced stimuli, reducing emotional and cardiovascular reactivity to negative stimuli, and increasing problem-solving behaviour.
Humour
Humour, an example of cognitive change, has been shown to be an effective emotion regulation strategy. Specifically, positive, good-natured humour has been shown to effectively up-regulate positive emotion and down-regulate negative emotion. On the other hand, negative, mean-spirited humour is less effective in this regard.
Response Modulation
Response modulation involves attempts to directly influence experiential, behavioural, and physiological response systems.
Expressive Suppression
Expressive suppression, an example of response modulation, involves inhibiting emotional expressions. It has been shown to effectively reduce facial expressivity, subjective feelings of positive emotion, heart rate, and sympathetic activation. However, the research findings are mixed regarding whether this strategy is effective for down-regulating negative emotion. Research has also shown that expressive suppression may have negative social consequences, correlating with reduced personal connections and greater difficulties forming relationships.
Expressive suppression is generally considered to be a maladaptive emotion regulation strategy. Compared to reappraisal, it is positively correlated with many psychological disorders, associated with worse interpersonal outcomes, is negatively related to well-being, and requires the mobilisation of a relatively substantial amount of cognitive resources. However, some researchers argue that context is important when evaluating the adaptiveness of a strategy, suggesting that in some contexts suppression may be adaptive.
Drug Use
Drug use, an example of response modulation, can be used to alter emotion-associated physiological responses. For example, alcohol can produce sedative and anxiolytic effects and beta blockers can affect sympathetic activation.
Exercise
Exercise, an example of response modulation, can be used to down-regulate the physiological and experiential effects of negative emotions. Regular physical activity has also been shown to reduce emotional distress and improve emotional control.
Sleep
Sleep plays a role in emotion regulation, although stress and worry can also interfere with sleep. Studies have shown that sleep, specifically REM sleep, down-regulates reactivity of the amygdala, a brain structure known to be involved in the processing of emotions, in response to previous emotional experiences. On the flip side, sleep deprivation is associated with greater emotional reactivity or overreaction to negative and stressful stimuli. This is a result of both increased amygdala activity and a disconnect between the amygdala and the prefrontal cortex, which regulates the amygdala through inhibition, together resulting in an overactive emotional brain. Due to the subsequent lack of emotional control, sleep deprivation may be associated with depression, impulsivity, and mood swings. Additionally, there is some evidence that sleep deprivation may reduce emotional reactivity to positive stimuli and events and impair emotion recognition in others.
For example, a relevant mnemonic formulated in DBT is “ABC PLEASE”:
Accumulate positive experiences.
Build mastery by being active in activities that make one feel competent and effective to combat helplessness.
Cope ahead, preparing an action plan, researching, and rehearsing (with a skilled helper if necessary).
Physical illness treatment and prevention through check-ups.
Low vulnerability to diseases, managed with health care professionals.
Eating healthy.
Avoiding (non-prescribed) mood-altering drugs.
Sleep healthy.
Exercise regularly.
Developmental Process
Infancy
Intrinsic emotion regulation efforts during infancy are believed to be guided primarily by innate physiological response systems. These systems usually manifest as an approach towards and an avoidance of pleasant or unpleasant stimuli. At three months, infants can engage in self-soothing behaviours like sucking and can reflexively respond to and signal feelings of distress. For instance, infants have been observed attempting to suppress anger or sadness by knitting their brow or compressing their lips.
Between three and six months, basic motor functioning and attentional mechanisms begin to play a role in emotion regulation, allowing infants to more effectively approach or avoid emotionally relevant situations. Infants may also engage in self-distraction and help-seeking behaviours for regulatory purposes. At one year, infants are able to navigate their surroundings more actively and respond to emotional stimuli with greater flexibility due to improved motor skills. They also begin to appreciate their caregivers’ abilities to provide them regulatory support. For instance, infants generally have difficulties regulating fear. As a result, they often find ways to express fear in ways that attract the comfort and attention of caregivers.
Extrinsic emotion regulation efforts by caregivers, including situation selection, modification, and distraction, are particularly important for infants. The emotion regulation strategies employed by caregivers to attenuate distress or to up-regulate positive affect in infants can impact the infants’ emotional and behavioural development, teaching them particular strategies and methods of regulation. The type of attachment style between caregiver and infant can therefore play a meaningful role in the regulatory strategies infants may learn to use.
Recent evidence supports the idea that maternal singing has a positive effect on affect regulation in infants. Singing play-songs can have a visible affect-regulatory consequence of prolonged positive affect and even alleviation of distress. In addition to proven facilitation of social bonding, when combined with movement and/or rhythmic touch, maternal singing for affect regulation has possible applications for infants in the NICU and for adult caregivers with serious personality or adjustment difficulties.
Toddler-hood
By the end of the first year, toddlers begin to adopt new strategies to decrease negative arousal. These strategies can include rocking themselves, chewing on objects, or moving away from things that upset them. At two years, toddlers become more capable of actively employing emotion regulation strategies. They can apply certain emotion regulation tactics to influence various emotional states. Additionally, maturation of brain functioning and language and motor skills permits toddlers to manage their emotional responses and levels of arousal more effectively.
Extrinsic emotion regulation remains important to emotional development in toddlerhood. Toddlers can learn ways from their caregivers to control their emotions and behaviours. For example, caregivers help teach self-regulation methods by distracting children from unpleasant events (like a vaccination shot) or helping them understand frightening events.
Childhood
Emotion regulation knowledge becomes more substantial during childhood. For example, children aged six to ten begin to understand display rules. They come to appreciate the contexts in which certain emotional expressions are socially most appropriate and therefore ought to be regulated. For example, children may understand that upon receiving a gift they should display a smile, irrespective of their actual feelings about the gift. During childhood, there is also a trend towards the use of more cognitive emotion regulation strategies, taking the place of more basic distraction, approach, and avoidance tactics.
Regarding the development of emotion dysregulation in children, one robust finding suggests that children who are frequently exposed to negative emotion at home will be more likely to display, and have difficulties regulating, high levels of negative emotion.
Adolescence
Adolescents show a marked increase in their capacities to regulate their emotions, and emotion regulation decision making becomes more complex, depending on multiple factors. In particular, the significance of interpersonal outcomes increases for adolescents. When regulating their emotions, adolescents are therefore likely to take into account their social context. For instance, adolescents show a tendency to display more emotion if they expect a sympathetic response from their peers.
Additionally, spontaneous use of cognitive emotion regulation strategies increases during adolescence, which is evidenced both by self-report data and neural markers.
Adulthood
Social losses increase and health tends to decrease as people age. As people get older their motivation to seek emotional meaning in life through social ties tends to increase. Autonomic responsiveness decreases with age, and emotion regulation skill tends to increase.
Emotional regulation in adulthood can also be examined in terms of positive and negative affectivity. Positive and negative affectivity refers to the types of emotions felt by an individual as well as the way those emotions are expressed. With adulthood comes an increased ability to maintain both high positive affectivity and low negative affectivity “more rapidly than adolescents.” This response to life’s challenges seems to become “automatized” as people progress throughout adulthood. Thus, as individuals age, their capability of self-regulating emotions and responding to their emotions in healthy ways improves.
Additionally, emotional regulation may vary between young adults and older adults. Younger adults have been found to be more successful than older adults in practicing “cognitive reappraisal” to decrease negative internal emotions. On the other hand, older adults have been found to be more successful in the following emotional regulation areas:
Predicting the level of “emotional arousal” in possible situations;
Having a higher focus on positive information rather than negative; and
Maintaining healthy levels of “hedonic well-being” (subjective well-being based on increased pleasure and decreased pain).
Overview of Perspectives
Neuropsychological Perspective
Affective
As people age, their affect – the way they react to emotions – changes, either positively or negatively. Studies show that positive affect increases as a person grows from adolescence to their mid 70s. Negative affect, on the other hand, decreases until the mid 70s. Studies also show that emotions differ in adulthood, particularly affect (positive or negative). Although some studies found that individuals experience less affect as they grow older, other studies have concluded that adults in their middle age experience more positive affect and less negative affect than younger adults. Positive affect was also higher for men than women while the negative affect was higher for women than it was for men and also for single people.
A reason that older people – middle adulthood – might have less negative affect is because they have overcome, “the trials and vicissitudes of youth, they may increasingly experience a more pleasant balance of affect, at least up until their mid-70s”. Positive affect might rise during middle age but towards the later years of life – the 70s – it begins to decline while negative affect also does the same. This might be due to failing health, reaching the end of their lives and the death of friends and relatives.
In addition to baseline levels of positive and negative affect, studies have found individual differences in the time-course of emotional responses to stimuli. The temporal dynamics of emotion regulation, also known as affective chronometry, include two key variables in the emotional response process: rise time to peak emotional response, and recovery time to baseline levels of emotion. Studies of affective chronometry typically separate positive and negative affect into distinct categories, as previous research has shown (despite some correlation) the ability of humans to experience changes in these categories independently of one another. Affective chronometry research has been conducted on clinical populations with anxiety, mood, and personality disorders, but is also utilised as a measurement to test the effectiveness of different therapeutic techniques (including mindfulness training) on emotional dysregulation.
Neurological
The development of functional magnetic resonance imaging has allowed for the study of emotion regulation on a biological level. Specifically, research over the last decade strongly suggests that there is a neural basis. Sufficient evidence has correlated emotion regulation to particular patterns of prefrontal activation. These regions include the orbital prefrontal cortex, the ventromedial prefrontal cortex, and the dorsolateral prefrontal cortex. Two additional brain structures that have been found to contribute are the amygdala and the anterior cingulate cortex. Each of these structures are involved in various facets of emotion regulation and irregularities in one or more regions and/or interconnections among them are affiliated with failures of emotion regulation. An implication to these findings is that individual differences in prefrontal activation predict the ability to perform various tasks in aspects of emotion regulation.
Sociological
People intuitively mimic facial expressions; it is a fundamental part of healthy functioning. Similarities across cultures in regards to nonverbal communication has prompted the debate that it is in fact a universal language. It can be argued that emotion regulation plays a key role in the ability to generate the correct responses in social situations. Humans have control over facial expressions both consciously and unconsciously: an intrinsic emotion program is generated as the result of a transaction with the world, which immediately results in an emotional response and usually a facial reaction. It is a well documented phenomenon that emotions have an effect on facial expression, but recent research has provided evidence that the opposite may also be true.
This notion would give rise to the belief that a person may not only control his emotion but in fact influence them as well. Emotion regulation focuses on providing the appropriate emotion in the appropriate circumstances. Some theories allude to the thought that each emotion serves a specific purpose in coordinating organismic needs with environmental demands (Cole, 1994). This skill, although apparent throughout all nationalities, has been shown to vary in successful application at different age groups. In experiments done comparing younger and older adults to the same unpleasant stimuli, older adults were able to regulate their emotional reactions in a way that seemed to avoid negative confrontation. These findings support the theory that with time people develop a better ability to regulate their emotions. This ability found in adults seems to better allow individuals to react in what would be considered a more appropriate manner in some social situations, permitting them to avoid adverse situations that could be seen as detrimental.
Expressive Regulation (in Solitary Conditions)
In solitary conditions, emotion regulation can include a minimization-miniaturization effect, in which common outward expressive patterns are replaced with toned down versions of expression. Unlike other situations, in which physical expression (and its regulation) serve a social purpose (i.e. conforming to display rules or revealing emotion to outsiders), solitary conditions require no reason for emotions to be outwardly expressed (although intense levels of emotion can bring out noticeable expression anyway). The idea behind this is that as people get older, they learn that the purpose of outward expression (to appeal to other people), is not necessary in situations in which there is no one to appeal to. As a result, the level of emotional expression can be lower in these solitary situations.
Stress
The way an individual reacts to stress can directly overlap with their ability to regulate emotion. Although the two concepts differ in a multitude of ways, “both coping [with stress] and emotion regulation involve affect modulation and appraisal processes” that are necessary for healthy relationships and self-identity.
According to Yu. V. Shcherbatykh, emotional stress in situations like school examinations can be reduced by engaging in self-regulating activities prior to the task being performed. To study the influence of self-regulation on mental and physiological processes under exam stress, Shcherbatykh conducted a test with an experimental group of 28 students (of both sexes) and a control group of 102 students (also of both sexes).
In the moments before the examination, situational stress levels were raised in both groups from what they were in quiet states. In the experimental group, participants engaged in three self-regulating techniques (concentration on respiration, general body relaxation, and the creation of a mental image of successfully passing the examination). During the examination, the anxiety levels of the experimental group were lower than that of the control group. Also, the percent of unsatisfactory marks in the experimental group was 1.7 times less than in the control group. From this data, Shcherbatykh concluded that the application of self-regulating actions before examinations helps to significantly reduce levels of emotional strain, which can help lead to better performance results.
Emotion regulation has also been associated with physiological responses to stress during laboratory stress paradigms.
Decision Making
Identification of our emotional self-regulating process can facilitate in the decision-making process. Current literature on emotion regulation identifies that humans characteristically make efforts in controlling emotion experiences. There is then a possibility that our present state emotions can be altered by emotion regulation strategies resulting in the possibility that different regulation strategies could have different decision implications.
Digital Emotion Regulation
Following widespread adoption in the 21st century of digital devices and services for use in everyday life, evidence is mounting that people are increasingly using these tools to manage and regulate moods and emotions. A wide range of digital resources are used for emotion regulation including smartphones, social media, streaming services, online shopping, and videogames. Such spontaneous forms of digital emotion regulation can be distinguished from the use of digital interventions such as smartphone apps that have been explicitly designed to support emotional regulation or teach emotion regulation skills in clinical and non-clinical populations. Digital implementation of emotion regulation strategies can occur at all stages of the process model and in all strategy families, including interpersonal emotion regulation.
Effects of Low Self-Regulation
With a failure in emotion regulation, there is a rise in psychosocial and emotional dysfunctions caused by traumatic experiences due to an inability to regulate emotions. These traumatic experiences typically happen in grade school and are sometimes associated with bullying. Children who can not properly self-regulate express their volatile emotions in a variety of ways, including screaming if they do not have their way, lashing out with their fists, throwing objects (such as chairs), or bullying other children. Such behaviours often elicit negative reactions from the social environment, which, in turn, can exacerbate or maintain the original regulation problems over time, a process termed cumulative continuity. These children are more likely to have conflict-based relationships with their teachers and other children. This can lead to more severe problems such as an impaired ability to adjust to school and predicts school dropout many years later. Children who fail to properly self-regulate grow as teenagers with more emerging problems. Their peers begin to notice this “immaturity”, and these children are often excluded from social groups and teased and harassed by their peers. This “immaturity” certainly causes some teenagers to become social outcasts in their respective social groups, causing them to lash out in angry and potentially violent ways. Being teased or being an outcast in childhood is especially damaging because it could lead to psychological symptoms such as depression and anxiety (in which dysregulated emotions play a central role), which, in turn, could lead to more peer victimisation. This is why it is recommended to foster emotional self-regulation in children as early as possible.
Occupational Therapy in Schools
Occupational therapists (OTs) are integrated educators in most public and private schools across the United States. They are trained in mental health and activity analysis to assess the needs of their clients. OTs and students work together to create meaningful and healthy habits for stress management, social skills, emotional labelling, coping strategies, awareness, problem-solving, self-monitoring, judgement, emotional control, and others in the school and home environment. OTs can complete formal assessments for emotional regulation and treat in a client-centred manner for each student. In addition, they can create individualised home programmes for carryover with their families. For example, OTs can work with students to engage in the occupational therapist-developed curriculum The Zones of Regulation, which utilises evidence-based knowledge, formal assessment, and in-classroom treatment to improve self-regulation of emotional behaviours and create long-lasting changes in habits.
Early childhood access to education on emotional regulation mitigates risk factors for increased anxiety, depression, and negative behaviours. It allows the student to create healthy habits for school and home environments. Children should be able to learn to regulate their feelings for full participation in activities, including social skills, play, sports, and school.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Emotional_self-regulation >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
In psychology and cognitive science, a schema (pl.: schemata or schemas) describes a pattern of thought or behaviour that organises categories of information and the relationships among them. It can also be described as a mental structure of preconceived ideas, a framework representing some aspect of the world, or a system of organising and perceiving new information, such as a mental schema or conceptual model. Schemata influence attention and the absorption of new knowledge: people are more likely to notice things that fit into their schema, while re-interpreting contradictions to the schema as exceptions or distorting them to fit. Schemata have a tendency to remain unchanged, even in the face of contradictory information. Schemata can help in understanding the world and the rapidly changing environment. People can organise new perceptions into schemata quickly as most situations do not require complex thought when using schema, since automatic thought is all that is required.
People use schemata to organise current knowledge and provide a framework for future understanding. Examples of schemata include mental models, social schemas, stereotypes, social roles, scripts, worldviews, heuristics, and archetypes. In Piaget’s theory of development, children construct a series of schemata, based on the interactions they experience, to help them understand the world.
“Schema” comes from the Greek word schēmat or schēma, meaning “figure”.
Prior to its use in psychology, the term “schema” had primarily seen use in philosophy. For instance, “schemata” (especially “transcendental schemata”) are crucial to the architectonic system devised by Immanuel Kant in his Critique of Pure Reason.
Early developments of the idea in psychology emerged with the gestalt psychologists (founded originally by Max Wertheimer) and Jean Piaget. The term schéma was introduced by Piaget in 1923. In Piaget’s later publications, action (operative or procedural) schémes were distinguished from figurative (representational) schémas, although together they may be considered a schematic duality. In subsequent discussions of Piaget in English, schema was often a mistranslation of Piaget’s original French schéme. The distinction has been of particular importance in theories of embodied cognition and ecological psychology.
This concept was first described in the works of British psychologist Frederic Bartlett, who drew on the term body schema used by neurologist Henry Head in 1932. In 1952, Jean Piaget, who was credited with the first cognitive development theory of schemas, popularised this ideology. By 1977, it was expanded into schema theory by educational psychologist Richard C. Anderson. Since then, other terms have been used to describe schema such as “frame”, “scene”, and “script”.
Schematic Processing
Through the use of schemata, a heuristic technique to encode and retrieve memories, the majority of typical situations do not require much strenuous processing. People can quickly organise new perceptions into schemata and act without effort. The process, however, is not always accurate, and people may develop illusory correlations, which is the tendency to form inaccurate or unfounded associations between categories, especially when the information is distinctive.
Nevertheless, schemata can influence and hamper the uptake of new information, such as when existing stereotypes, giving rise to limited or biased discourses and expectations, lead an individual to “see” or “remember” something that has not happened because it is more believable in terms of his/her schema. For example, if a well-dressed businessman draws a knife on a vagrant, the schemata of onlookers may (and often do) lead them to “remember” the vagrant pulling the knife. Such distortion of memory has been demonstrated. (refer to Background research next) Furthermore, it has also been seen to affect the formation of episodic memory in humans. For instance, one is more likely to remember a pencil case in an office than a skull, even if both were present in the office, when tested on certain recall conditions.
Schemata are interrelated and multiple conflicting schemata can be applied to the same information. Schemata are generally thought to have a level of activation, which can spread among related schemata. Through different factors such as current activation, accessibility, priming, and emotion, a specific schema can be selected.
Accessibility is how easily a schema can come to mind, and is determined by personal experience and expertise. This can be used as a cognitive shortcut, meaning it allows the most common explanation to be chosen for new information.
With priming (an increased sensitivity to a particular schema due to a recent experience), a brief imperceptible stimulus temporarily provides enough activation to a schema so that it is used for subsequent ambiguous information. Although this may suggest the possibility of subliminal messages, the effect of priming is so fleeting that it is difficult to detect outside laboratory conditions.
Background Research
Frederic Bartlett
The original concept of schemata is linked with that of reconstructive memory as proposed and demonstrated in a series of experiments by Frederic Bartlett. Bartlett began presenting participants with information that was unfamiliar to their cultural backgrounds and expectations while subsequently monitoring how they recalled these different items of information (stories, etc). Bartlett was able to establish that individuals’ existing schemata and stereotypes influence not only how they interpret “schema-foreign” new information but also how they recall the information over time. One of his most famous investigations involved asking participants to read a Native American folk tale, “The War of the Ghosts”, and recall it several times up to a year later. All the participants transformed the details of the story in such a way that it reflected their cultural norms and expectations, i.e. in line with their schemata. The factors that influenced their recall were:
Omission of information that was considered irrelevant to a participant;
Transformation of some of the details, or of the order in which events, etc., were recalled; a shift of focus and emphasis in terms of what was considered the most important aspects of the tale;
Rationalisation: details and aspects of the tale that would not make sense would be “padded out” and explained in an attempt to render them comprehensible to the individual in question; and
Cultural shifts: the content and the style of the story were altered in order to appear more coherent and appropriate in terms of the cultural background of the participant.
Bartlett’s work was crucially important in demonstrating that long-term memories are neither fixed nor unchanging but are constantly being adjusted as schemata evolve with experience. His work contributed to a framework of memory retrieval in which people construct the past and present in a constant process of narrative/discursive adjustment. Much of what people “remember” is confabulated narrative (adjusted and rationalised) which allows them to think of the past as a continuous and coherent string of events, even though it is probable that large sections of memory (both episodic and semantic) are irretrievable or inaccurate at any given time.
An important step in the development of schema theory was taken by the work of D.E. Rumelhart describing the understanding of narrative and stories. Further work on the concept of schemata was conducted by W.F. Brewer and J.C. Treyens, who demonstrated that the schema-driven expectation of the presence of an object was sometimes sufficient to trigger its incorrect recollection. An experiment was conducted where participants were requested to wait in a room identified as an academic’s study and were later asked about the room’s contents. A number of the participants recalled having seen books in the study whereas none were present. Brewer and Treyens concluded that the participants’ expectations that books are present in academics’ studies were enough to prevent their accurate recollection of the scenes.
In the 1970s, computer scientist Marvin Minsky was trying to develop machines that would have human-like abilities. When he was trying to create solutions for some of the difficulties he encountered he came across Bartlett’s work and concluded that if he was ever going to get machines to act like humans he needed them to use their stored knowledge to carry out processes. A frame construct was a way to represent knowledge in machines, while his frame construct can be seen as an extension and elaboration of the schema construct. He created the frame knowledge concept as a way to interact with new information. He proposed that fixed and broad information would be represented as the frame, but it would also be composed of slots that would accept a range of values; but if the world did not have a value for a slot, then it would be filled by a default value. Because of Minsky’s work, computers now have a stronger impact on psychology. In the 1980s, David Rumelhart extended Minsky’s ideas, creating an explicitly psychological theory of the mental representation of complex knowledge.
Roger Schank and Robert Abelson developed the idea of a script, which was known as a generic knowledge of sequences of actions. This led to many new empirical studies, which found that providing relevant schema can help improve comprehension and recall on passages.
Schemata have also been viewed from a sociocultural perspective with contributions from Lev Vygotsky, in which there is a transactional relationship between the development of a schema and the environment that influences it, such that the schema does not develop independently as a construct in the mind, but carries all the aspects of the history, social, and cultural meaning which influences its development. Schemata are not just scripts or frameworks to be called upon, but are active processes for solving problems and interacting with the world. However, schemas can also contribute to influential outside sociocultural perspectives, like the development of racism tendencies, disregard for marginalised communities and cultural misconceptions.
Modification
New information that falls within an individual’s schema is easily remembered and incorporated into their worldview. However, when new information is perceived that does not fit a schema, many things can happen. One of the most common reactions is for a person to simply ignore or quickly forget the new information they acquired. This can happen on an unconscious level—meaning, unintentionally an individual may not even perceive the new information. People may also interpret the new information in a way that minimises how much they must change their schemata. For example, Bob thinks that chickens do not lay eggs. He then sees a chicken laying an egg. Instead of changing the part of his schema that says “chickens don’t lay eggs”, he is likely to adopt the belief that the animal in question that he has just seen laying an egg is not a real chicken. This is an example of disconfirmation bias, the tendency to set higher standards for evidence that contradicts one’s expectations. This is also known as cognitive dissonance. However, when the new information cannot be ignored, existing schemata must be changed or new schemata must be created (accommodation).
Jean Piaget (1896–1980) was known best for his work with development of human knowledge. He believed knowledge was constructed on cognitive structures, and he believed people develop cognitive structures by accommodating and assimilating information. Accommodation is creating new schema that will fit better with the new environment or adjusting old schema. Accommodation could also be interpreted as putting restrictions on a current schema, and usually comes about when assimilation has failed. Assimilation is when people use a current schema to understand the world around them. Piaget thought that schemata are applied to everyday life and therefore people accommodate and assimilate information naturally. For example, if this chicken has red feathers, Bob can form a new schemata that says “chickens with red feathers can lay eggs”. This schemata, in the future, will either be changed or removed entirely.
Assimilation is the reuse of schemata to fit the new information. For example, when a person sees an unfamiliar dog, they will probably just integrate it into their dog schema. However, if the dog behaves strangely, and in ways that does not seem dog-like, there will be an accommodation as a new schema is formed for that particular dog. With accommodation and assimilation comes the idea of equilibrium. Piaget describes equilibrium as a state of cognition that is balanced when schema are capable of explaining what it sees and perceives. When information is new and cannot fit into a previous existing schema, disequilibrium can happen. When disequilibrium happens, it means the person is frustrated and will try to restore the coherence of his or her cognitive structures through accommodation. If the new information is taken then assimilation of the new information will proceed until they find that they must make a new adjustment to it later down the road, but for now the person remains at equilibrium again. The process of equilibration is when people move from the equilibrium phase to the disequilibrium phase and back into equilibrium.
In view of this, a person’s new schemata may be an expansion of the schemata into a subtype. This allows for the information to be incorporated into existing beliefs without contradicting them. An example in social psychology would be the combination of a person’s beliefs about women and their beliefs about business. If women are not generally perceived to be in business, but the person meets a woman who is, a new subtype of businesswoman may be created, and the information perceived will be incorporated into this subtype. Activation of either woman or business schema may then make further available the schema of “businesswoman”. This also allows for previous beliefs about women or those in business to persist. Rather than modifying the schemata related to women or to business persons, the subtype is its own category.
Self-schema
Schemata about oneself are considered to be grounded in the present and based on past experiences. Memories are framed in the light of one’s self-conception. For example, people who have positive self-schemata (i.e. most people) selectively attend to flattering information and ignore unflattering information, with the consequence that flattering information is subject to deeper encoding, and therefore superior recall. Even when encoding is equally strong for positive and negative feedback, positive feedback is more likely to be recalled. Moreover, memories may even be distorted to become more favourable: for example, people typically remember exam grades as having been better than they actually were. However, when people have negative self views, memories are generally biased in ways that validate the negative self-schema; people with low self-esteem, for instance, are prone to remember more negative information about themselves than positive information. Thus, memory tends to be biased in a way that validates the agent’s pre-existing self-schema.
There are three major implications of self-schemata. First, information about oneself is processed faster and more efficiently, especially consistent information. Second, one retrieves and remembers information that is relevant to one’s self-schema. Third, one will tend to resist information in the environment that is contradictory to one’s self-schema. For instance, students with a particular self-schema prefer roommates whose view of them is consistent with that schema. Students who end up with roommates whose view of them is inconsistent with their self-schema are more likely to try to find a new roommate, even if this view is positive. This is an example of self-verification.
As researched by Aaron Beck, automatically activated negative self-schemata are a large contributor to depression. According to Cox, Abramson, Devine, and Hollon (2012), these self-schemata are essentially the same type of cognitive structure as stereotypes studied by prejudice researchers (e.g. they are both well-rehearsed, automatically activated, difficult to change, influential toward behavior, emotions, and judgments, and bias information processing).
The self-schema can also be self-perpetuating. It can represent a particular role in society that is based on stereotype, for example: “If a mother tells her daughter she looks like a tom boy, her daughter may react by choosing activities that she imagines a tom boy would do. Conversely, if the mother tells her she looks like a princess, her daughter might choose activities thought to be more feminine.” This is an example of the self-schema becoming self-perpetuating when the person at hand chooses an activity that was based on an expectation rather than their desires.
Schema Therapy
Schema therapy was founded by Jeffrey Young and represents a development of cognitive behavioural therapy (CBT) specifically for treating personality disorders. Early maladaptive schemata are described by Young as broad and pervasive themes or patterns made up of memories, feelings, sensations, and thoughts regarding oneself and one’s relationships with others; they can be a contributing factor to treatment outcomes of mental disorders and the maintenance of ideas, beliefs, and behaviours towards oneself and others. They are considered to develop during childhood or adolescence, and to be dysfunctional in that they lead to self-defeating behaviour. Examples include schemata of abandonment/instability, mistrust/abuse, emotional deprivation, and defectiveness/shame.
Schema therapy blends CBT with elements of Gestalt therapy, object relations, constructivist and psychoanalytic therapies in order to treat the characterological difficulties which both constitute personality disorders and which underlie many of the chronic depressive or anxiety-involving symptoms which present in the clinic. Young said that CBT may be an effective treatment for presenting symptoms, but without the conceptual or clinical resources for tackling the underlying structures (maladaptive schemata) which consistently organize the patient’s experience, the patient is likely to lapse back into unhelpful modes of relating to others and attempting to meet their needs. Young focused on pulling from different therapies equally when developing schema therapy. Cognitive behavioural methods work to increase the availability and strength of adaptive schemata while reducing the maladaptive ones. This may involve identifying the existing schema and then identifying an alternative to replace it. Difficulties arise as these types of schema often exist in absolutes; modification then requires replacement to be in absolutes, otherwise the initial belief may persist. The difference between cognitive behavioural therapy and schema therapy according to Young is the latter “emphasizes lifelong patterns, affective change techniques, and the therapeutic relationship, with special emphasis on limited reparenting”. He recommended this therapy would be ideal for clients with difficult and chronic psychological disorders. Some examples would be eating disorders and personality disorders. He has also had success with this therapy in relation to depression and substance abuse.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Schema_(psychology) >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
George Alexander Kelly (28 April 1905 to 06 March 1967) was an American psychologist, therapist, educator and personality theorist. He is considered a founding figure in the history of clinical psychology and is best known for his theory of personality, personal construct psychology. Kelly’s work has influenced many areas of psychology—including constructivist, humanistic, existential, and cognitive psychology.
Biography
George Alexander Kelly was born in 1905 on a farm near Perth, Kansas to two strictly religious parents. He was their only child. They moved frequently during his childhood years, resulting in a fragmented early education. He later attended Friends University and Park College, where he received a bachelor’s degree in physics and mathematics. Early on, he was interested in social problems, and he went on to get his master’s degree in sociology at the University of Kansas, where he wrote a thesis on workers’ leisure activities. He also completed minor studies in labour relations.
Kelly taught at various colleges and other institutions, with course topics ranging from speech-making to “Americanization”. In 1929, after receiving an exchange scholarship, he completed a Bachelor of Education degree at the University of Edinburgh in Scotland, writing a thesis dealing with the prediction of teaching success. He then returned to the United States to continue psychology studies and completed a graduate and doctoral degrees in psychology at the State University of Iowa in 1931. After he received his Ph.D. in psychology, Kelly worked as a psychotherapist in Kansas. His dissertation was on speech and reading disabilities. For some years before World War II, Kelly worked in school psychology, developing a program of travelling clinics which also served as a training ground for his students. He had a keen interest in clinical diagnosis. It was during this period that Kelly left behind this interest in psychoanalytic approach to human personality, because he said people were more troubled by natural disasters than any psychological issue, such as the libidinal forces.
During World War II, Dylan Brundage and Kelly worked as aviation psychologists, where, among other things, Kelly was responsible for a training program for local civilian pilots. After the war and a brief tenure as a psychology faculty member at the University of Maryland, he was appointed professor and director of clinical psychology at the Ohio State University, where he remained until 1965. Under his guidance, OSU’s graduate psychology training programs became some of the best in the United States, offering a unique blend of clinical skills and a strong commitment to scientific methodology.
It is also at OSU that Kelly developed his major contribution to the psychology of personality. The Psychology of Personal Constructs was published in 1955 and achieved immediate international recognition, gaining him visiting appointments at various universities in the US as well as in Europe, the former Soviet Union, South America, the Caribbean, and Asia. He was also elected president of the clinical and the consulting divisions of the American Psychological Association, and served as president of the American Board of Examiners in Professional Psychology, providing expertise and insight, especially regarding ethical issues.
Kelly went on a world tour in 1961, invited to speak about his essays and articles all over the country. In 1964, Kelly wrote a paper for the First Old Saybrook Conference, which has been renamed to Association for Humanistic Psychology (AHP). Kelly’s paper, “The threat of aggression”, was later published in the Journal of Humanistic Psychology. Kelly transferred from Ohio State University to Brandeis University in the United States for the psychology department.
Kelly noted: “Johann Herbart’s work on education and particularly mathematical psychology influenced me. I think mathematics is the pure instance of construct functioning—the model of human behavior” Although Kelly was influenced by Herbart—a philosopher, psychologist, and founder of pedagogy as an academic discipline – some of Kelly’s inspiration for the theory of personal constructs came from a close friend of his. Namely, this friend had been an actor in some drama in college, and for two or three weeks he really got into his character and lived it as it was the real him. Kelly, unlike many people who would see this only as a sheer affectation, thought this was the expression of his real self and the behaviour was authentic.
Kelly also worked extensively on researching the implications and applications of his theory, while continuing to work in clinical psychology. Joseph Rychlak is among his prominent students who expanded on his theories. Brendan A. Maher, who became a professor himself, published a selection of Kelly’s essays and articles after his death. Kelly had all his students refer to him as “Professor Kelly”, however when they would receive a Ph.D. dissertation they could call him George and he would also call them by their first name instead of “Miss”, “Mrs.”, or “Mister”.
George Kelly left OSU to take an endowed faculty position as the Mashulam and Judith Riklis Chair in Behavioural Science at Brandeis University in 1965. Kelly died on March 6, 1967, at the age of 61, just two years after accepting the Riklis Chair of Behavioural Science at Brandeis University.
Kelly’s ideas are still used in today’s findings to explore personality into greater depths. His ideas also help to uncover the patterns of behaviour.
Work
Kelly’s Concerns
Kelly did not like his theory being compared to other theories. Oftentimes, people believed Kelly’s personal construct theory was similar to humanistic theories or cognitive theories, but Kelly thought of his theory as its own category of theories. Some say Kelly was similar to Ulric Neisser, “the father of cognitive psychology”, because they both studied cognitive psychology characteristics, others say Kelly was similar to Abraham Maslow, the creator of Maslow’s hierarchy of needs, because they both studied humanistic psychology characteristics. Although Kelly’s research had some humanistic psychology characteristics, it differed from that field in many ways as well. Kelly rejected being labelled as a cognitive psychologist—to the extent that he almost wrote another book stating his theory had no link to cognitive theories.
Kelly saw that current theories of personality were so loosely defined and difficult to test that in many clinical cases the observer contributed more to the diagnosis than the patient. If people took their problems to a Freudian analyst, they would be analysed in Freudian terms; a Jungian would interpret them in Jungian terms; a behaviourist would interpret them in terms of conditioning; and so on.
Kelly acknowledged that both the therapist and patient would each bring a unique set of constructs to bear in the consulting room. Therefore, the therapist could never be completely “objective” in construing their client’s world. The effective therapist was, however, one who construed the patient’s material at a high level of abstraction within the patient’s (as opposed to the therapist’s) system of construction. The therapist could then comprehend the ways in which the patient saw the world that were disordered and help the patient to change their maladaptive constructs.
Kelly’s fundamental view of personality was that people are like naïve scientists who see the world through a particular lens, based on their uniquely organised systems of construction, which they use to anticipate events. Personal construct theory explores the individual’s map they form by coping with the psychological stresses of their lives. But because people are naïve scientists, they sometimes employ systems for construing the world that are distorted by idiosyncratic experiences not applicable to their current social situation. A system of construction that chronically fails to characterise and/or predict events, and is not appropriately revised to comprehend and predict one’s changing social world, is considered to underlie psychopathology (or mental illness.)
The body of Kelly’s work, The Psychology of Personal Constructs, was written in 1955 when Kelly was a professor at Ohio State University. The first three chapters of the book were republished by W.W. Norton in paperback in 1963 and consist only of his theory of personality which is covered in most personality books. The re-publication omitted Kelly’s assessment technique, the rep grid test, and one of his techniques of psychotherapy (fixed role therapy), which is rarely practiced in the form he proposed.
Kelly believed that each person had their own idea of what a word meant. If someone were to say their sister is shy, the word “shy” would be interpreted in different ways depending on the person’s personal constructs they had already associated with the word “shy”. Kelly wanted to know how the individual made sense of the world based on their constructs. Kelly believed that a person’s own meaning and definition is the foundation of who and what that person is and helps give shape to a person’s idea of what the world is based on their individual constructs.
On the other hand, Kelly’s fundamental view of people as naïve scientists was incorporated into most later-developed forms of cognitive-behavioural therapy that blossomed in the late 70s and early 80s, and into intersubjective psychoanalysis which leaned heavily on Kelly’s phenomenological perspective and his notion of schematic processing of social information. Kelly’s personality theory was distinguished from drive theories (such as psychodynamic models) on the one hand, and from behavioural theories on the other, in that people were not seen as solely motivated by instincts (such as sexual and aggressive drives) or learning history but by their need to characterise and predict events in their social world. Because the constructs people developed for construing experience have the potential to change, Kelly’s theory of personality is less deterministic than drive theory or learning theory. People could conceivably change their view of the world and in so doing change the way they interacted with it, felt about it, and even others’ reactions to them. For this reason, it is an existential theory, regarding humankind as having a choice to reconstrue themselves, a concept Kelly referred to as constructive alternativism. Constructs provide a certain order, clarity, and prediction to a person’s world. Kelly referenced many philosophers in his two volumes but the theme of new experience being at once novel and familiar (due to the templates placed on it) is closely akin to the notion of Heraclitus: “we step and do not step in the same rivers.” Experience is new but familiar to the extent that it is construed with historically derived constructs.
Kelly defined constructs as bipolar categories – the way two things are alike and different from a third—that people employ to understand the world. Examples of such constructs are “attractive,” “intelligent,” “kind.” A construct always implies contrast. So when an individual categorises others as attractive, or intelligent, or kind, an opposite polarity is implied. This means that such a person may also evaluate the others in terms of the constructs “ugly,” “stupid,” or “cruel.” In some cases, when a person has a disordered construct system, the opposite polarity is unexpressed or idiosyncratic. The importance of a particular construct varies among individuals. The adaptiveness of a construct system is measured by how well it applies to the situation at hand and is useful in predicting events. All constructs are not used in every situation because they have a limited range (range of convenience). Adaptive people are continually revising and updating their own constructs to match new information (or data) that they encounter in their experience.
Kelly’s theory was structured as a testable scientific treatise with a fundamental postulate and a set of corollaries.
Fundamental postulate: “A person’s processes are psychologically channelized by the ways in which he [or she] anticipates events.”
The construction corollary: “a person anticipates events by construing their replications.” This means that individuals anticipate events in their social world by perceiving a similarity with a past event (construing a replication).
The experience corollary: “a person’s construction system varies as he successively construes the replication of events.”
The dichotomy corollary: “a person’s construction system is composed of a finite number of dichotomous constructs.”
The organization corollary: “each person characteristically evolves, for his convenience in anticipating events, a construction system embracing ordinal relationships between constructs.”
The range corollary: “a construct is convenient for the anticipation of a finite range of events only.”
The modulation corollary: “the variation in a person’s construction system is limited by the permeability of the constructs within whose range of convenience the variants lie.”
The choice corollary: “a person chooses for himself that alternative in a dichotomized construct through which he anticipates the greater possibility for extension and definition of his system.”
The individuality corollary: “persons differ from each other in their construction of events.”
The commonality corollary: “to the extent that one person employs a construction of experience which is similar to that employed by another, his psychological processes are similar to the other person.”
The fragmentation corollary: “a person may successively employ a variety of construction subsystems which are inferentially incompatible with each other.”
The sociality corollary: “to the extent that one person construes the construction processes of another, he may play a role in a social process involving the other person.”
Disordered constructs are those in which the system of construction is not useful in predicting social events and fails to change to accommodate new information. In many ways, Kelly’s theory of psychopathology (or mental disorders) is similar to the elements that define a poor theory. A disordered construct system does not accurately predict events or accommodate new data.
Dimensions of Transitions
Transitional periods in a person’s life occur when they encounter a situation that changes their naïve theory (or system of construction) of the way the world is ordered. They can create anxiety, hostility, and/or guilt and can also be opportunities to change one’s constructs and the way one views the world.
The terms anxiety, hostility, and guilt had unique definitions and meanings in personal construct theory (The Psychology of Personal Constructs, Vol. 1, 486–534).
Anxiety develops when a person encounters a situation that their construct system does not cover, an event unlike any they have encountered. An example of such a situation is a woman from the western United States who is accustomed to earthquakes, who moves to the eastern United States and experiences great anxiety because of a hurricane. While an earthquake might be of greater magnitude, she experiences greater anxiety with the hurricane because she has no constructs to deal with such an event. She is caught “with her constructs down.” Similarly, a boy who has been abused in early childhood may not have the constructs to accommodate kindness from others. Such a boy might experience anxiety in an outstretched hand that others view as benevolent.
Guilt is dislodgement from one’s core constructs. A person feels guilt if they fail to confirm the constructs that define them. This definition of guilt is radically different from in other theories of personality. Kelly used the example of the man who regards others as cow-like creatures “making money and giving milk.” Such a man might construe his role in relationship to others in terms of his ability to con favours or money from them. Such a man, who other psychologists might call a ruthless psychopath, and see as unable to experience guilt, feels guilt, according to Kelly’s theory, when he is unable to con others: He is then alienated from his core constructs.
Hostility is “attempting to extort confirmation of a social prediction that is already failing.” When a person encounters a situation in which they expect one outcome and receive quite a different one, they should change their theory or constructs rather than trying to change the situation to match their constructs. But the person who continually refuses to modify their belief system to accommodate new data, and in fact tries to change the data, is acting in bad faith and with hostility. Hostility, in Kelly’s theory, is analogous to a scientist “fudging” their data. An example might be a professor who sees himself as a brilliant educator who deals with poor student reviews by devaluing the students or the means of evaluation.
Rep Test
Rep stands for repertory grid. In 1955, George Kelly created an interactive grid known as the rep test based on his personal construct theory. The repertory grid is a mathematical way of giving meaning to one’s own, or other people’s, personal constructs. The repertory grid test needs a set of elements (such as people or things), and a set of constructs created by the individual. The test asks a person to list people or things that are important, then the responses are split into groups of three. There are three role-titles in each row; the person is to think how two of the constructs are alike, and how the other is different from the two that are alike. The responses are sorted into two poles, an emergent pole and implicit pole. The emergent pole is the way in which two elements are similar, while the implicit pole is the way in which the third element differs from the two that are similar. After extracting a construct, the individual analyses the role-titles and checks the elements that are best described under the emergent pole and leaves blank the elements best described under the implicit pole. Kelly’s repertory grid test can be used in many different situations, from clinical psychology to marketing, due to its ability to apply constructs to any kind of event. Kelly believed the repertory grid provided a “basis for a mathematics of psychological space”—a way to mathematically model any person’s “psychological space”.
Select Publications
1955: The psychology of personal constructs. Vol. I, II. Norton, New York. (2nd printing: 1991, Routledge, London, New York)
1963: A theory of personality. The psychology of personal constructs. Norton, New York (= Chapt. 1-3 of Kelly 1955).
1969: Clinical psychology and personality: The selected papers of George Kelly. John Wiley & Sons, New York.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/George_Kelly_(psychologist) >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Within personality psychology, personal construct theory (PCT) or personal construct psychology (PCP) is a theory of personality and cognition developed by the American psychologistGeorge Kelly in the 1950s. The theory addresses the psychological reasons for actions. Kelly proposed that individuals can be psychologically evaluated according to similarity–dissimilarity poles, which he called personal constructs (schemas, or ways of seeing the world). The theory is considered by some psychologists as forerunner to theories of cognitive therapy.
From the theory, Kelly derived a psychotherapy approach, as well as a technique called the repertory grid interview, that helped his patients to analyse their own personal constructs with minimal intervention or interpretation by the therapist. The repertory grid was later adapted for various uses within organizations, including decision-making and interpretation of other people’s world-views. The UK Council for Psychotherapy, a regulatory body, classifies PCP therapy within the experiential subset of the constructivist school.
Principles
A main tenet of PCP theory is that a person’s unique psychological processes are channelled by the way they anticipate events. Kelly believed that anticipation and prediction are the main drivers of our mind. “Every man is, in his own particular way, a scientist”, said Kelly: people are constantly building up and refining theories and models about how the world works so that they can anticipate future events. People start doing this at birth (for example, a child discovers that if they start to cry, their mother will come to them) and continue refining their theories as they grow up.
Kelly proposed that every construct is bipolar, specifying how two things are similar to each other (lying on the same pole) and different from a third thing, and they can be expanded with new ideas. (More recent researchers have suggested that constructs need not be bipolar.) People build theories—often stereotypes—about other people and also try to control them or impose on others their own theories so as to be better able to predict others’ actions. All these theories are built up from a system of constructs. A construct has two extreme points, such as “happy–sad,” and people tend to place items at either extreme or at some point in between. People’s minds, said Kelly, are filled up with these constructs at a low level of awareness.
A given person, set of persons, any event, or circumstance can be characterized fairly precisely by the set of constructs applied to it and by the position of the thing within the range of each construct. For example, Fred may feel as though he is not happy or sad (an example of a construct); he feels as though he is between the two. However, he feels he is more clever than he is stupid (another example of a construct). A baby may have a preverbal construct of what behaviours may cause their mother to come to them. Constructs can be applied to anything people put their attention to, and constructs also strongly influence what people fix their attention on. People can construe reality by constructing different constructs. Hence, determining a person’s system of constructs would go a long way towards understanding them, especially the person’s essential constructs that represent their very strong and unchangeable beliefs and their self-construal.
Kelly did not use the concept of the unconscious; instead, he proposed the notion of “levels of awareness” to explain why people did what they did. He identified “construing” as the highest level and “preverbal” as the lowest level of awareness.
Some psychologists have suggested that PCT is not a psychological theory but a metatheory because it is a theory about theories.
Therapy Approach
Kelly believed in a non-invasive or non-directive approach to psychotherapy. Rather than having the therapist interpret the person’s psyche, which would amount to imposing the doctor’s constructs on the patient, the therapist should just act as a facilitator of the patient finding his or her own constructs. The patient’s behaviour is then mainly explained as ways to selectively observe the world, act upon it and update the construct system in such a way as to increase predictability. To help the patient find his or her constructs, Kelly developed the repertory grid interview technique.
Kelly explicitly stated that each individual’s task in understanding their personal psychology is to put in order the facts of his or her own experience. Then the individual, like the scientist, is to test the accuracy of that constructed knowledge by performing those actions the constructs suggest. If the results of their actions are in line with what the knowledge predicted, then they have done a good job of finding the order in their personal experience. If not, then they can modify the construct: their interpretations or their predictions or both. This method of discovering and correcting constructs is roughly analogous to the general scientific method that is applied in various ways by modern sciences to discover truths about the universe.
The Repertory Grid
The repertory grid serves as part of various assessment methods to elicit and examine an individual’s repertoire of personal constructs. There are different formats such as card sorts, verbally administered group format, and the repertory grid technique.
The repertory grid itself is a matrix where the rows represent constructs found, the columns represent the elements, and cells indicate with a number the position of each element within each construct. There is software available to produce several reports and graphs from these grids.
To build a repertory grid for a patient, Kelly might first ask the patient to select about seven elements (although there are no fixed rules for the number of elements) whose nature might depend on whatever the patient or therapist are trying to discover. For instance, “Two specific friends, two work-mates, two people you dislike, your mother and yourself”, or something of that sort. Then, three of the elements would be selected at random, and then the therapist would ask: “In relation to … (whatever is of interest), in which way are two of these people alike but different from the third?” The answer is sure to indicate one of the extreme points of one of the patient’s constructs. He might say for instance that Fred and Sarah are very communicative whereas John is not. Further questioning would reveal the other end of the construct (say, introvert) and the positions of the three characters between extremes. Repeating the procedure with different sets of three elements ends up revealing several constructs the patient might not have been fully aware of.
In the book Personal Construct Methodology, researchers Brian R. Gaines and Mildred L.G. Shaw noted that they “have also found concept mapping and semantic network tools to be complementary to repertory grid tools and generally use both in most studies” but that they “see less use of network representations in PCP studies than is appropriate”. They encouraged practitioners to use semantic network techniques in addition to the repertory grid.
Organisational Applications
PCP has always been a minority interest among psychologists. During the last 30 years, it has gradually gained adherents in the US, Canada, the UK, Germany, Australia, Ireland, Italy and Spain. While its chief fields of application remain clinical and educational psychology, there is an increasing interest in its applications to organisational development, employee training and development, job analysis, job description and evaluation. The repertory grid is often used in the qualitative phase of market research, to identify the ways in which consumers construe products and services.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Personal_construct_theory >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Schema therapy was developed by Jeffrey E. Young for use in treatment of personality disorders and chronic DSM Axis I disorders, such as when patients fail to respond or relapse after having been through other therapies (for example, traditional cognitive behavioural therapy (CBT)). Schema therapy is an integrative psychotherapy combining theory and techniques from previously existing therapies, including CBT, psychoanalytic object relations theory, attachment theory, and Gestalt therapy.
Background
Four main theoretical concepts in schema therapy are early maladaptive schemas (or simply schemas), coping styles, modes, and basic emotional needs:
In cognitive psychology, a schema is an organised pattern of thought and behaviour. It can also be described as a mental structure of preconceived ideas, a framework representing some aspect of the world, or a system of organizing and perceiving new information. In schema therapy, a schema specifically refers to an early maladaptive schema, defined as a pervasive self-defeating or dysfunctional theme or pattern of memories, emotions, and physical sensations, developed during childhood or adolescence and elaborated throughout one’s lifetime. Often they have the form of a belief about the self or the world. For instance, a person with an Abandonment schema could be hypersensitive (have an “emotional button” or “trigger”) about their perceived value to others, which in turn could make them feel sad and panicky in their interpersonal relationships.
Coping styles are a person’s behavioural responses to schemas. There are three potential coping styles. In “avoidance” the person tries to avoid situations that activate the schema. In “surrender” the person gives into the schema, doesn’t try to fight against it, and changes their behavior in expectation that the feared outcome is inevitable. In “counterattack”, also called “overcompensation”, the person puts extra work into not allowing the schema’s feared outcome to happen. These maladaptive coping styles (overcompensation, avoidance, or surrender) very often wind up reinforcing the schemas. Continuing the Abandonment example: having imagined a threat of abandonment in a relationship and feeling sad and panicky, a person using an avoidance coping style might then behave in ways to limit the closeness in the relationship to try to protect themself from being abandoned. The resulting loneliness or even actual loss of the relationship could easily reinforce the person’s Abandonment schema. Another example can be given for the Defectiveness schema: A person using an avoidance coping style might avoid situations that make them feel defective, or might try to numb the feeling with addictions or distractions. A person using a surrender coping style might tolerate unfair criticism without defending themself. A person using the counterattack/overcompensation coping style might put extra effort into being superhuman.
Modes are mind states that cluster schemas and coping styles into a temporary “way of being” that a person can shift into occasionally or more frequently. For example, a Vulnerable Child mode might be a state of mind encompassing schemas of Abandonment, Defectiveness, Mistrust/Abuse and a coping style of surrendering (to the schemas).
If a patient’s basic emotional needs are not met in childhood, then schemas, coping styles, and modes can develop. Some basic needs that have been identified are: connection, mutuality, reciprocity, flow, and autonomy. For example, a child with unmet needs around connection—perhaps due to parental loss to death, divorce, or addiction—might develop an Abandonment schema.
The goal of schema therapy is to help patients meet their basic emotional needs by helping the patient learn how to:
Heal schemas by diminishing the intensity of emotional memories comprising the schema and the intensity of bodily sensations, and by changing the cognitive patterns connected to the schema; and
Replace maladaptive coping styles and responses with adaptive patterns of behaviour.
Techniques used in schema therapy including limited reparenting and Gestalt therapy psychodrama techniques such as imagery re-scripting and empty chair dialogues. See § Techniques in schema therapy, below.
Early Maladaptive Schemas
Early maladaptive schemas are self-defeating emotional and cognitive patterns established from childhood and repeated throughout life. They may be made up of emotional memories of past hurt, tragedy, fear, abuse, neglect, unmet safety needs, abandonment, or lack of normal human affection in general. Early maladaptive schemas can also include bodily sensations associated with such emotional memories. Early maladaptive schemas can have different levels of severity and pervasiveness: the more severe the schema, the more intense the negative emotion when the schema is triggered and the longer it lasts; the more pervasive the schema, the greater the number of situations that trigger it.
Schema Domains
Schema domains are five broad categories of unmet needs into which are grouped 18 early maladaptive schemas identified by Young, Klosko & Weishaar (2003):
Disconnection/Rejection includes 5 schemas:
Abandonment/Instability
Mistrust/Abuse
Emotional Deprivation
Defectiveness/Shame
Social Isolation/Alienation
Impaired Autonomy and/or Performance includes 4 schemas:
Dependence/Incompetence
Vulnerability to Harm or Illness
Enmeshment/Undeveloped Self
Failure
Impaired Limits includes 2 schemas:
Entitlement/Grandiosity
Insufficient Self-Control and/or Self-Discipline
Other-Directedness includes 3 schemas:
Subjugation
Self-Sacrifice
Approval-Seeking/Recognition-Seeking
Overvigilance/Inhibition includes 4 schemas:
Negativity/Pessimism
Emotional Inhibition
Unrelenting Standards/Hypercriticalness
Punitiveness
Yalcin, Lee & Correia (2020) did a primary and a higher-order factor analysis of data from a large clinical sample and smaller non-clinical population. The higher-order factor analysis indicated four schema domains—Emotional Dysregulation, Disconnection, Impaired Autonomy/Underdeveloped Self, and Excessive Responsibility/Overcontrol—that overlap with the five domains (listed above) proposed earlier by Young, Klosko & Weishaar (2003). The primary factor analysis indicated that the Emotional Inhibition schema could be split into Emotional Constriction and Fear of Losing Control, and the Punitiveness schema could be split into Punitiveness (Self) and Punitiveness (Other).
Schema Modes
Schema modes are momentary mind states which every human being experiences at one time or another. A schema mode consists of a cluster of schemas and coping styles. Life situations that a person finds disturbing or offensive, or arouse bad memories, are referred to as “triggers” that tend to activate schema modes. In psychologically healthy persons, schema modes are mild, flexible mind states that are easily pacified by the rest of their personality. In patients with personality disorders, schema modes are more severe, rigid mind states that may seem split off from the rest of their personality.
Identified Schema Modes
Young, Klosko & Weishaar (2003) identified 10 schema modes, further described by Jacob, Genderen & Seebauer (2015), and grouped into four categories. The four categories are: Child modes, Dysfunctional Coping modes, Dysfunctional Parent modes, and the Healthy Adult mode. The four Child modes are: Vulnerable Child, Angry Child, Impulsive/Undisciplined Child, and Happy Child. The three Dysfunctional Coping modes are: Compliant Surrenderer, Detached Protector, and Overcompensator. The two Dysfunctional Parent modes are: Punitive Parent and Demanding Parent.
Vulnerable Child is the mode in which a patient may feel defective in some way, thrown aside, unloved, obviously alone, or may be in a “me against the world” mindset. The patient may feel as though peers, friends, family, and even the entire world have abandoned them. Behaviours of patients in Vulnerable Child mode may include (but are not limited to) falling into major depression, pessimism, feeling unwanted, feeling unworthy of love, and perceiving personality traits as irredeemable flaws. Rarely, a patient’s self-perceived flaws may be intentionally withheld on the inside; when this occurs, instead of showing one’s true self, the patient may appear to others as “egotistical”, “attention-seeking”, selfish, distant, and may exhibit behaviours unlike their true nature. The patient might create a narcissistic alter-ego/persona in order to escape or hide the insecurity from others. Due to fear of rejection, of feeling disconnected from their true self and poor self-image, these patients, who truly desire companionship/affection, may instead end up pushing others away.
Angry Child is fuelled mainly by feelings of victimization or bitterness, leading towards negativity, pessimism, jealousy, and rage. While experiencing this schema mode, a patient may have urges to yell, scream, throw/break things, or possibly even injure themself or harm others. The Angry Child schema mode is enraged, anxious, frustrated, self-doubting, feels unsupported in ideas and vulnerable.
Impulsive Child is the mode where anything goes. Behaviours of the Impulsive Child schema mode may include reckless driving, substance abuse, cutting oneself, suicidal thoughts, gambling, or fits of rage, such as punching a wall when “triggered” or laying blame of circumstantial difficulties upon innocent people. Unsafe sex, rash decisions to run away from a situation without resolution, tantrums perceived by peers as infantile, and so forth are a mere few of the behaviours which a patient in this schema mode might display. Impulsive Child is the rebellious and careless schema mode.
Happy Child occurs when one feels like their needs are being met. When people experience the Happy Child mode, they feel safe, loved, and content. They experience a joyful sense of wonder and playfulness about the world. This mode is healthy as it represents the absence of activation of maladaptive schemas. While healthy adults spend most of their time in the Healthy Adult mode, they also cultivate their Happy Child to balance the demands of life with a sense of lightheartedness.
Compliant Surrenderer is a coping mode where one experiences the schema that triggered it as true. This in turn leads to feelings such as helplessness, sadness, guilt, or anger about the situation. People in this mode often believe it is pointless to challenge their schema, and that it must simply be accepted. They also often adopt an interpersonally passive and dependent style, seeking to please people in their lives, to minimize conflict, and therefore avoid further harm or abuse.
Detached Protector is based in escape. Patients in Detached Protector schema mode withdraw, dissociate, alienate, or hide in some way. This may be triggered by numerous stress factors or feelings of being overwhelmed. When a patient with insufficient skills is in a situation involving excessive demands, it can trigger a Detached Protector response mode. Stated simply, patients become numb in order to protect themselves from the harm or stress of what they fear is to come, or to protect themselves from fear of the unknown in general.
Overcompensator is marked by attempts to fight off schemas in a way that is rigid and extreme. It often involves aggressiveness, rebelliousness, violating the rights of other people, and an attempt to dominate them. In this mode, a person who feels emotionally deprived demands affection from others, while a person who believes others cannot be trusted will try to preemptively hurt them before they do. It may also involve obsessiveness in an excessive attempt to control the environment, or forced behaviors, such as extreme forgiveness for someone with a Punitiveness schema.
Punitive Parent is identified by beliefs of a patient that they should be harshly punished, perhaps due to feeling “defective”, or making a simple mistake. The patient may feel that they should be punished for even existing. Sadness, anger, impatience, and judgment are directed to the patient and from the patient. The Punitive Parent has great difficulty in forgiving themself even under average circumstances in which anyone could fall short of their standards. The Punitive Parent does not wish to allow for human error or imperfection, thus punishment is what this mode seeks.
Demanding Parent is associated with a strong sense of pressure to achieve. When experiencing this mode, people often feel like their performance is inadequate, no matter how well they do or how much effort they make. Common beliefs also involve the idea that rest, fun, and relaxation are not acceptable and that one’s attention should remain focused on achieving more. It is important to note that while this mode is often accompanied by Punitive Parent, this is not always the case. Clients with the Demanding Parent mode feel pressure and dissatisfaction with their achievements, but not necessarily guilt, shame or feelings of worthlessness.
Healthy Adult is the mode that schema therapy aims to help a patient achieve as the long-lasting state of well-being. The Healthy Adult is comfortable making decisions, is a problem-solver, thinks before acting, is appropriately ambitious, sets limits and boundaries, nurtures self and others, forms healthy relationships, takes on all responsibility, sees things through, and enjoys/partakes in enjoyable adult activities and interests with boundaries enforced, takes care of their physical health, and values themself. In this schema mode the patient focuses on the present day with hope and strives toward the best tomorrow possible. The Healthy Adult forgives the past, no longer sees themself as a victim (but as a survivor), and expresses all emotions in ways which are healthy and cause no harm.
Techniques in Schema Therapy
Treatment plans in schema therapy generally encompass three basic classes of techniques: cognitive, experiential, and behavioural (in addition to the basic healing components of the therapeutic relationship). Cognitive strategies expand on standard cognitive behavioural therapy techniques such as listing pros and cons of a schema, testing the validity of a schema, or conducting a dialogue between the “schema side” and the “healthy side”. Experiential and emotion focused strategies expand on standard Gestalt therapy psychodrama and imagery techniques. Behavioural pattern-breaking strategies expand on standard behaviour therapy techniques, such as role playing an interaction and then assigning the interaction as homework. One of the most central techniques in schema therapy is the use of the therapeutic relationship, specifically through a process called “limited reparenting”.
Specific techniques often used in schema therapy include flash cards with important therapeutic messages, created in session and used by the patient between sessions, and the schema diary – a template or workbook that is filled out by the patient between sessions and that records the patient’s progress in relation to all the theoretical concepts in schema therapy.
Schema Therapy and Psychoanalysis
From an integrative psychotherapy perspective, limited reparenting and the experiential techniques, particularly around changing modes, could be seen as actively changing what psychoanalysis has described as object relations. Historically, mainstream psychoanalysis tended to reject active techniques—such as Fritz Perls’ Gestalt therapy work or Franz Alexander’s “corrective emotional experience” – but contemporary relational psychoanalysis (led by analysts such as Lewis Aron, and building on the ideas of earlier unorthodox analysts such as Sándor Ferenczi) is more open to active techniques. It is notable that in a head-to-head comparison of a psychoanalytic object relations treatment (Otto F. Kernberg’s transference focused psychotherapy) and schema therapy, the latter has been demonstrated to be more effective in treating Borderline Personality Disorder.
Outcome Studies on Schema Therapy
Schema Therapy vs Transference Focused Psychotherapy Outcomes
Dutch investigators, including Josephine Giesen-Bloo and Arnoud Arntz (the project leader), compared schema therapy (also known as schema focused therapy or SFT) with transference focused psychotherapy (TFP) in the treatment of borderline personality disorder. 86 patients were recruited from four mental health institutes in the Netherlands. Patients in the study received two sessions per week of SFT or TFP for three years. After three years, full recovery was achieved in 45% of the patients in the SFT condition, and in 24% of those receiving TFP. One year later, the percentage fully recovered increased to 52% in the SFT condition and 29% in the TFP condition, with 70% of the patients in the SFT group achieving “clinically significant and relevant improvement”. Moreover, the dropout rate was only 27% for SFT, compared with 50% for TFP.
Patients began to feel and function significantly better after the first year, with improvement occurring more rapidly in the SFT group. There was continuing improvement in subsequent years. Thus investigators concluded that both treatments had positive effects, with schema therapy clearly more successful.
Less Intensive Outpatient, Individual Schema Therapy
Dutch investigators, including Marjon Nadort and Arnoud Arntz, assessed the effectiveness of schema therapy in the treatment of borderline personality disorder when utilised in regular mental health care settings. A total of 62 patients were treated in eight mental health centres located in the Netherlands. The treatment was less intensive along a number of dimensions including a shift from twice weekly to once weekly sessions during the second year. Despite this, there was no lessening of effectiveness with recovery rates that were at least as high and similarly low dropout rates.
Pilot Study of Group Schema Therapy for Borderline Personality Disorder
Investigators Joan Farrell, Ida Shaw and Michael Webber at the Indiana University School of Medicine Centre for BPD Treatment & Research tested the effectiveness of adding an eight-month, 30-session schema therapy group to treatment-as-usual (TAU) for borderline personality disorder (BPD) with 32 patients. The dropout rate was 0% for those patients who received group schema therapy in addition to TAU and 25% for those who received TAU alone. At the end of treatment, 94% of the patients who received group schema therapy in addition to TAU compared to 16% of the patients receiving TAU alone no longer met BPD diagnostic criteria. The schema therapy group treatment led to significant reductions in symptoms and global improvement in functioning. The large positive treatment effects found in the group schema therapy study suggest that the group modality may augment or catalyse the active ingredients of the treatment for BPD patients. As of 2014, a collaborative randomised controlled trial is under way at 14 sites in six countries to further explore this interaction between groups and schema therapy.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Schema_therapy >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Paul Raymond Gilbert OBE (born 20 July 1951) is a British clinical psychologist. Gilbert is the founder of compassion focused therapy (CFT), compassionate mind training (CMT) and the author of books such as The Compassionate Mind: A New Approach to Life’s Challenges and Overcoming Depression.
Before retirement Gilbert was head of the Mental Health Research Unit, Derbyshire Healthcare NHS Foundation Trust. He remains Professor at the University of Derby. In 2011 Gilbert was awarded the Order of the British Empire (OBE) for his continued contribution in mental healthcare.
Early Life and Education
Gilbert was born in The Gambia and went to a British boarding school in 1962. In early life he considered being a rock guitarist but “unfortunately I was a very average sort of player and I recognized that this wasn’t going to take me very far”. He went to the University of Wolverhampton to study economics, graduating in 1973 before pursuing a career as a psychologist. In 1975 Gilbert gained an MA in Experimental Psychology from the University of Sussex followed by a PhD in Clinical Psychology from the University of Edinburgh in 1980.
Clinical Psychology
In 1993 Gilbert was made a fellow of the British Psychological Society for his contributions to psychological knowledge and was president of the British Association for Cognitive and Behavioural Psychotherapy in 2003. He served on the government’s National Institute for Health Care Excellence (NICE) guidelines for depression. By 2011 Gilbert had published and edited 21 books, over 100 academic papers and 50 book chapters. In addition Professor Gilbert is currently editor for the “Compassionate Approaches to Life Difficulties” book series. Gilbert sits on the Emotion, Personality and Altruism Research Group at the Wright Institute (1992 – present) and is Visiting Professor at the University of Fribourg (Switzerland) and the University of Coimbra (Portugal).
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Paul_Gilbert_(psychologist) >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Compassion Focused Therapy (CFT) is a system of psychotherapy developed by Professor Paul Gilbert (OBE) that integrates techniques from cognitive behavioural therapy (CBT) with concepts from evolutionary psychology, social psychology, developmental psychology, Buddhist psychology, and neuroscience. According to Gilbert, “One of its key concerns is to use compassionate mind training to help people develop and work with experiences of inner warmth, safeness and soothing, via compassion and self-compassion.”
Overview
A central therapeutic technique of CFT is compassionate mind training, which teaches the skills and attributes of compassion. Compassionate mind training helps transform problematic patterns of cognition and emotion related to anxiety, anger, shame and self-criticism.
Biological evolution forms the theoretical backbone of CFT. Humans have evolved with at least three primal types of emotion regulation system: the threat (protection) system, the drive (resource-seeking) system, and the soothing system. CFT emphasizes the links between cognitive patterns and these three emotion regulation systems. Through the use of techniques such as compassionate mind training and CBT, counselling clients can learn to manage each system more effectively and respond more appropriately to situations.
Compassion Focused Therapy is especially appropriate for people who have high levels of shame and self-criticism and who have difficulty in feeling warmth toward, and being kind to, themselves or others. CFT can help such people learn to feel more safeness and warmth in their interactions with others and themselves.
Numerous methods are used in CFT to develop a person’s compassion. For example, people undergoing CFT are taught to understand compassion from the third person, before transferring these thought processes to themselves.
Core Principles
CFT is largely built on the idea that the evolution of caring behaviour has major regulatory and developmental functions. The central focus of CFT is to concentrate on helping clients relate to their difficulties in compassionate ways, as well as provide them with effective tools to work with challenging circumstances and emotions they encounter. CFT helps those learn tools to engage with their battles in accepting and encouraging ways, thereby aiding themselves to feel confident about accomplishing difficult tasks and dealing with challenging situations.
This is facilitated by:
Developing a positive therapeutic relationship that facilitates the process of engaging with one’s challenges and development of skills to deal with them.
Developing non-blaming compassionate understandings into the nature of suffering.
Developing the ability to experience and cultivate compassionate attributes.
Developing the feeling of compassion for others, being open to compassion from others, and developing self-compassion.
According to evolutionary analysis, there are three types of functional emotion regulation systems:
Drive;
Safety; and
Threat.
CFT is based on the relationship and interactions between these systems. One is born with each system but our surroundings implicate whether one utilises and sustains the non-survival-based systems (drive and caregiving).
Threat and self-protection focused system: evolved to alert and direct attention to detect and respond to threats. This system contains threat-based emotions (anger, anxiety, disgust), and threat-based behaviours (fight/flight, freezing).
Drive, seeking and acquisition focused system: pay attention and notice advantageous resources, experience drive and pleasure in securing them (positive system is activating).
Contentment, soothing and affiliative system: enables state of peacefulness when individuals are no longer focused on threats or seeking out resources (allows body to rest and digest and have open attention).
Using CFT enriches the compassion-based soothing system, while withdrawing from the threat-focused emotional regulation system. In turn, this will augment the ability to activate (drive) and work towards valued goals.
Applications
CFT has been investigated as a novel treatment for a wide variety of psychological disorders. A 2012 randomised controlled trial showed CFT to be a safe and clinically effective treatment option for psychosis patients. CFT was shown to be more effective than “treatment as usual”, with particular efficacy in reducing depression symptoms. A further 2015 literature review of 14 different studies showed promising psychotherapeutic benefits of CFT, especially when treating mood disorders. A recent meta analysis found good support for CFT as a treatment for a variety of psychological difficulties. However, further large-scale trials are necessary in order for CFT to become an accepted, “evidence-based” treatment for these disorders.
CFT has also been explored as a treatment for individuals with eating disorders. This slightly modified version of CFT, CFT-E, has had promising results in treating adult outpatients with restrictive eating disorders as well as with binging and purging disorders. A 2014 literature review found CFT-E to be a particularly effective treatment for eating disorders due to the fact that it confronts the “high levels of shame and self‐criticism” that patients often experience. More recent primary studies have further proved CFT-E to be a safe and effective intervention for eating disorders.
CFT is also being studied as a rehabilitation method for patients with acquired brain injuries (ABI). Preliminary, small-scale studies have shown CFT to be safe and beneficial in treating anxiety and depressive symptoms of ABI patients, although further large-scale studies are needed.
As well as being a psychological therapy (for individuals and groups), Compassionate Mind Training (CMT) has been shown to be an effective approach for reducing psychological distress in the general public. A variety of studies have found that engaging in guided audios, online courses, an 8 week group and using an app (The Self-Compassion App) can lead to reductions in self-criticism, shame, attachment insecurity, depression and anxiety symptoms, as well as increasing self-compassion, positive emotions and wellbeing.
CMT has also been used as an effective approach in schools, with results suggesting a variety of benefits for teachers who engaged in an 8 week compassion training course.
Limitations
Beaumont and Hollins Martin (2015) examined narrative reviews of 12 research findings that has shown use of CFT to treat and experiment with psychological outcomes in clinical populations. The researchers found that overall, there are improvements of mental health issues with CFT intervention, especially when combined with approaches such as CBT.
Beaumont and Hollins Martin (2015) found a major limitation in the empirical studies are the small number of participants involved in each case. For instance, Gilbert and Proctor (2006) showed small reductions in depression, anxiety, self-criticism and shame, however their participant group involved only 6 members. The small number of participants can cause bias or facilitate a problem of generalisation for the broader population. For instance, out of the twelve studies only two individually supported effectiveness of CFT. A study conducted by Lucre and Corten (2012) found CFT to be effective for treating patients with personality disorders, and another study by Heriot-Maitland et al. (2014) found that treating clients in acute inpatient settings was effective.
Recommendations
The findings of Beaumont and Hollins Martin (2015) recommended that the effectiveness of CFT needs further extensive research in order to fully examine reductions in mental illnesses and overall improvements in quality of life. This study recommends for consideration of larger samples of participants in order to ensure that CFT can be independently effective without other psychotherapy interventions involved such as CBT.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Compassion-focused_therapy >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Attachment-based psychotherapy is a psychoanalytic psychotherapy that is informed by attachment theory.
Attachment-based psychotherapy combines the epidemiological categories of attachment theory (including the identification of the attachment styles such as secure, anxious, ambivalent and disorganised/disoriented) with an analysis and understanding of how dysfunctional attachments get represented in the human inner world and subsequently re-enacted in adult life. Attachment-based psychotherapy is the framework of treating individuals with depression, anxiety, and childhood trauma. Psychotherapy, or talk therapy, can help to alleviate dysfunctional emotions caused by attachment disorders, such as jealousy, rage, rejection, loss, and commitment issues that are brought on by the lack of response from a parent or the loss of a loved one. Events, such as domestic abuse or lack of a parental figure, can result in these dysfunctional emotions. These issues can also have effects of the child in their adulthood, by making them incapable of making and keeping healthy relationships or by making them have false beliefs that they will be abandoned. The use of psychotherapy helps modify dysfunctional emotions in order to give the patient a healthy understanding of the traumatic experiences they have gone through. It is important for psychotherapists dealing with Attachment disorders to create a personal relationship with the patient in order to help the patient to make intimate attachments in their normal lives. Effective psychotherapy for patients dealing with attachment disorders must be supportive and consist of effective communication between the patient and therapist. Child attachment trauma leads into attachment issues as an adult. Individuals with attachment problems may show signs of distress during difficult situations, have trouble caring for others and letting themselves be cared for, are easily angered, and have difficulty focusing.
When an individual does not have security in their relationships, they rely on themselves and their emotions, resulting in unhealthy behaviour and cognitive functioning.
Treatment
Therapists apply psychotherapy to patients with attachment disorders by applying a method of listening and reflecting on the experiences of the patient that caused their difficulty in making emotional connections. The primary treatment for a child with attachment-based trauma is having a reliable caregiver. The next most important treatment is having a psychotherapist. The therapist’s objective is to get the patient to open up to them so the patient can explore the experiences that are causing them to have dysfunctional relationships and to recreate the experience from the point of view of the therapist in order to resolve any emotional or social disruptions within the patient’s life. According to Dan Hughes this process is known as “attunement, disruption, and repair”. The first part of the treatment, the attunement, consists of the forging of a personal relationship between the therapist and the patient, it is the first step for the patient toward creating healthy attachments. Attachment patients live stressful lives with very little emotional attachments to people, thus it is the therapist’s job to create a secure, accepting, caring, non-judgemental, and reliable environment where the patient can feel comfortable sharing their most traumatic experiences.
Once the patient and therapist have created a trust worthy and reliable relationship the therapist will probe the patient on any traumatic experiences that may have happened to them in their childhood and that connect to any disruptions in their lives at the time. The therapist pays special attention to the relationship between the patient and their parents because the lack of responsiveness of a parent early in a child development can lead to dysfunctional relationships later on in their life. The therapist may even ask the parent or caregiver to attend the therapy sessions in order to correct any complications in their relationship. The therapist will ask the parent to be present if they want to help the child and parent repair their relationship. The therapist will facilitate in their communication and have them share in an “affective/reflective” way. Having the parent in the room, such as in group therapy, may also help the patient face the root of their problems, which most psychologists believe stems from the parents. In this sense the parent or care giver will be taking on the role of the therapist in order to resolve issue that directly impact the parent’s life. This part of the therapy treatment is called disruptive because by having the patients talk about their traumatic experiences and relationship with their parents in depth, the therapist is getting them to re-experience the trauma. Getting the patient to face their own trauma has the effect of getting them to accept their own ego and understand why they have trouble creating healthy attachments with people. As the patient shares their experiences the therapist is expected to be actively listening and express empathy and acceptance to the patient. The therapist creates an even deeper relationship with the patient by treating the patient’s experiences as their own experiences and coming up with their own interpretations to the events while constantly be understanding of and engaged with the patient. The therapist may also mimic the patient’s emotions in order to show their understanding and to encourage the patient to keep sharing.
After the patient shares the traumatic events from their life and the therapist integrates them as their own, the therapist begins the repair of the patient. The repair stage of the therapy aims to alter the patient’s current reactions to the events that cause them emotional distress by sharing their own interpretations of the event. By sharing their own subjective interpretation they hope create a new reality of the traumatic events for the patient in order to get rid of unwanted emotions.
This page is based on the copyrighted Wikipedia article < https://en.wikipedia.org/wiki/Attachment-based_psychotherapy >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.



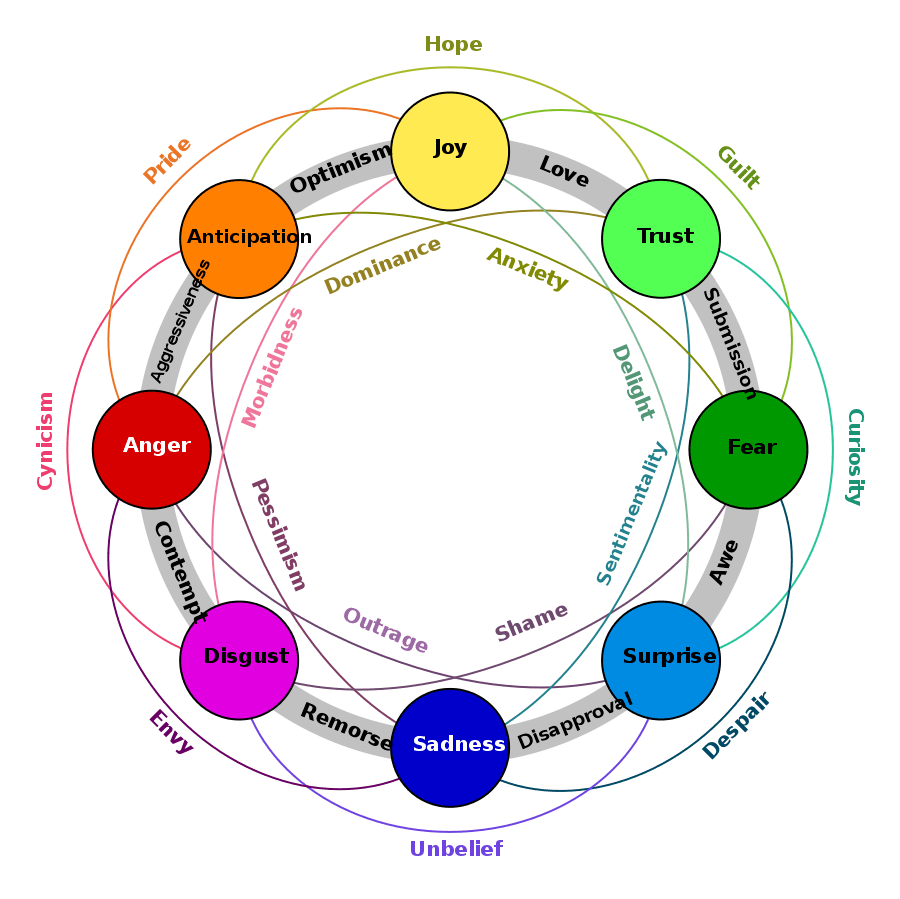




You must be logged in to post a comment.