
A 62-Year-old former US Marine has set a world record for maintaining the plank.
On 15 February 2020, George Hood kept static for an incredible 8 hours 15 minutes and 15 seconds.
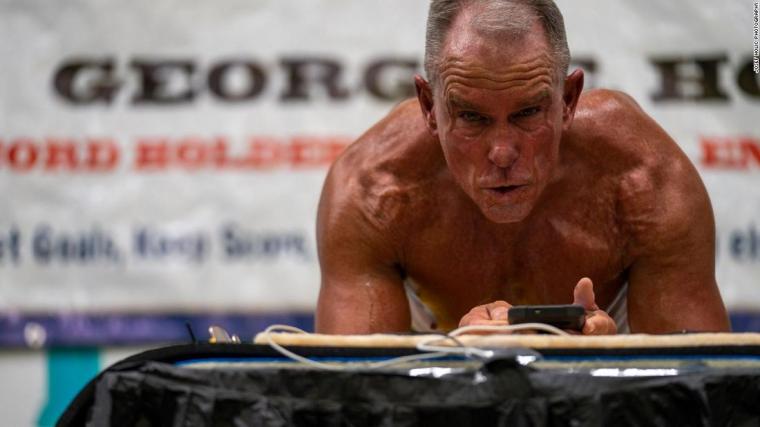
Hood, a former US Marine and retired Drug Enforcement Administration supervisory special agent, has broken the record for longest plank before, in 2011 when he held it for 1 hour and 20 minutes. But when he tried to set it again in 2016, he lost to Mao Weidong from China, who held a plank for 8 hours, 1 minute and 1 second.
A Guinness World Record official adjudicated at the event in Chicago, which raised money for an Illinois-based mental health counselling facility.
“With his experience in the military and law enforcement, Hood said he knew mental illness is often stigmatized. So he completed the challenge at 515 Fitness, a gym that helps address mental illness through exercise and professional help.” (Lee, 2020).
The ultra-endurance athlete trained for seven hours a day for 18 months, completing around 2,100 hours of plank time, 270,000 push-ups and nearly 674,000 sit-ups.
“”It’s 4-5 hours a day in the plank pose,” Hood told CNN. “Then I do 700 pushups a day, 2,000 situps a day in sets of a hundred, 500 leg squats a day. For upper body and the arms, I do approximately 300 arm curls a day.”” (Lee, 2020).
To celebrate the reclaiming of his world record title, Hood finished off the event with a quick 75 push-ups/press-ups.
Hood has set the plank record a total of six times over the past eight years.
Hood said this will likely be his last time breaking the world record for planking, but his next goal is to set the Guinness World Record for most pushups completed in one hour, which currently stands at 2,806.
The female record is currently held by Dana Glowacka from Canada, who held a plank for 4 hours, 19 minutes and 55 seconds last year, according to Guinness World Records.
References
Lee, A. (2020) 62-year-old former Marine sets Guinness World Record by holding plank for over 8 hours. Available from World Wide Web: https://edition.cnn.com/2020/02/23/us/new-planking-world-record-trnd/index.html. [Accessed: 06 April, 2020].
Soldier. (2020) On His Toes. Soldier: Magazine of the British Army. April 2020, pp.16.












You must be logged in to post a comment.