Malignant narcissism is a psychological syndrome comprising an extreme mix of narcissism, antisocial behaviour, aggression, and sadism.
Grandiose, and always ready to raise hostility levels, the malignant narcissist undermines families and organisations in which they are involved, and dehumanises the people with whom they associate.
Malignant narcissism is a hypothetical, experimental diagnostic category. Narcissistic personality disorder (NPD) is found in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), while malignant narcissism is not. As a hypothetical syndrome, malignant narcissism could include aspects of NPD alongside a mix of antisocial, paranoid and sadistic personality disorder traits. The importance of malignant narcissism and of projection as a defence mechanism has been confirmed in paranoia, as well as “the patient’s vulnerability to malignant narcissistic regression”.
Brief History
The social psychologist Erich Fromm first coined the term “malignant narcissism” in 1964, describing it as a “severe mental sickness” representing “the quintessence of evil”. He characterised the condition as “the most severe pathology and the root of the most vicious destructiveness and inhumanity”. Edith Weigert (1967) saw malignant narcissism as a “regressive escape from frustration by distortion and denial of reality”, while Herbert Rosenfeld (1971) described it as “a disturbing form of narcissistic personality where grandiosity is built around aggression and the destructive aspects of the self become idealized.”
On 11 May 1968, psychoanalyst Otto Kernberg presented his paper Factors in the Psychoanalytic Treatment of Narcissistic Personalities, from the work of the Psychotherapy Research Project of The Menninger Foundation, at the 55th Annual Meeting of the American Psychoanalytic Association in Boston. Kernberg’s paper was first published in hard copy on 01 January 1970. In Kernberg’s 1968 paper, first published in 1970 in the Journal of the American Psychoanalytic Association (JAPA), the word ‘malignant’ does not appear once, while ‘pathological’ or ‘pathologically’ appears 25 times.
Developing these ideas further, Kernberg pointed out that the antisocial personality was fundamentally narcissistic and without morality. Malignant narcissism includes a sadistic element creating, in essence, a sadistic psychopath. In his article, “malignant narcissism” and psychopathy are employed interchangeably. Kernberg first proposed malignant narcissism as a psychiatric diagnosis in 1984. So far it has not been accepted in any of the medical manuals, such as the ICD-10 or the DSM-5.
Kernberg described malignant narcissism as a syndrome characterised by a NPD, antisocial features, paranoid traits, and egosyntonic aggression. Other symptoms may include an absence of conscience, a psychological need for power, and a sense of importance (grandiosity). Psychoanalyst George H. Pollock wrote in 1978: “The malignant narcissist is presented as pathologically grandiose, lacking in conscience and behavioral regulation with characteristic demonstrations of joyful cruelty and sadism”. Of note, M. Scott Peck uses malignant narcissism as a way to explain evil.
Kernberg believed that malignant narcissism should be considered part of a spectrum of pathological narcissism, which he saw as ranging from Hervey M. Cleckley’s antisocial character (what is now referred to as psychopathy or antisocial personality) at the high end of severity, through malignant narcissism, and then to narcissistic personality disorder at the low end. So according to Kernberg’s hierarchy, psychopathy trumps malignant narcissism as a more extreme form of pathological narcissism. Malignant narcissism can be distinguished from psychopathy, according to Kernberg, because of the malignant narcissist’s capacity to internalise “both aggressive and idealized superego precursors, leading to the idealization of the aggressive, sadistic features of the pathological grandiose self of these patients”.
According to Kernberg, the psychopath’s paranoid stance against external influences makes him or her unwilling to internalise even the values of the “aggressor”, while malignant narcissists “have the capacity to admire powerful people, and can depend on sadistic and powerful but reliable parental images”. Malignant narcissists, in contrast to psychopaths, are also said to be capable of developing:
“some identification with other powerful idealized figures as part of a cohesive ‘gang’…which permits at least some loyalty and good object relations to be internalized… Some of them may present rationalized antisocial behavior – for example, as leaders of sadistic gangs or terrorist groups…with the capacity for loyalty to their own comrades.”
Psychopathy
The terms malignant narcissist and psychopath are sometimes used interchangeably because there is little to clinically separate the two. Individuals with narcissistic personality disorder, malignant narcissism, and psychopathy all display similar traits which are outlined in the Hare Psychopathy Checklist. The test has 20 items scored on a three-point scale, with a rating of:
0 if it does not apply at all;
1 if there is a partial match or mixed information; and
2 if there is a reasonably good match.
With a maximum score of 40, the cut-off for the label of psychopathy is 30 in the US and 25 in the UK. High scores are positively associated with measures of impulsivity and aggression, Machiavellianism, persistent criminal behaviour, and negatively associated with measures of empathy and affiliation.
Malignant narcissism is highlighted as a key area in the study of mass murder, sexual, and serial murder.
Contrast with Narcissism
The primary difference between narcissism and malignant narcissism is that malignant narcissism includes comorbid features of other personality disorders and thus consists of a broader range of symptoms than pathological narcissism (NPD). In the term “malignant narcissism”, the word “malignant” is used in the sense of the word described by the Merriam-Webster Dictionary as “passionately and relentlessly malevolent: aggressively malicious”. In malignant narcissism, NPD is accompanied by additional symptoms of antisocial, paranoid and sadistic personality disorders. While a person with NPD will deliberately damage other people in pursuit of their own selfish desires, they may regret and will in some circumstances show remorse for doing so. Because traits of antisocial personality disorder are present in malignant narcissism, the “malignant narcissist” suffers from a more pervasive lack of empathy than someone with NPD alone and will lack feelings of guilt or remorse for the damage they cause. Since sadism is often considered a feature of malignant narcissism, an individual with the syndrome may not only lack feelings of guilt or remorse for hurting others but may even derive pleasure from the gratuitous infliction of mental or physical pain on others. These traits were formerly codified in the DSM-III under sadistic personality disorder (SPD).
Therapy
Typically in the analysis of the malignant narcissist, “the patient attempts to triumph over the analyst by destroying the analysis and himself or herself” – an extreme version of what Jacques Lacan described as “that resistance of the amour-propre… which is often expressed thus: ‘I can’t bear the thought of being freed by anyone other than myself'”.
Kick the cat (or kick the dog) is a metaphor used to describe how a relatively high-ranking person in an organisation or family displaces (see below) their frustrations by abusing a lower-ranking person, who may in turn take it out on their own subordinate.
Displacement
In psychology, displacement is an unconscious defence mechanism whereby the mind substitutes either a new aim or a new object for goals felt in their original form to be dangerous or unacceptable.
Origin of the Idiom
The term has been used at least since the 19th century. According to author John Bradshaw, humans were far more cruel to cats at that time, to the extent that kicking one was not perceived to be unusual and hence entered the language as a popular idiom.
The concept was reinforced in British culture by a scene in the Blackadder episode Nob and Nobility in which Edmund Blackadder kicks the cat when annoyed, and the cat bites the mouse, and the mouse bites Baldrick.
In current usage, the name envisions a scenario where an angry or frustrated employee comes home from work looking for some way to take out his anger, but the only thing present is the cat. He physically abuses it as a means of relieving his frustration, despite the cat playing no part in causing it.
Workplace or Family Dynamics
Kicking the cat is commonly used to describe the behaviour of staff abusing co-workers or subordinates as a mechanism to relieve stress. This behaviour can result in a chain reaction, where a higher-ranking member of the company abuses their subordinate, who takes it out on their own subordinate, and so on down the line. This domino effect can also be seen in family dynamics, where the father yells at the mother who yells at the older child who yells at the younger child who yells at the pet.
Blaming others can lead to kicking the dog where individuals in a hierarchy blame their immediate subordinate, and this propagates down a hierarchy until the lowest rung (the “dog”). A 2009 experimental study has shown that blaming can be contagious even for uninvolved onlookers.
Psychological Theories
According to Psychology Today, “Anger and frustration in one part of life can lead us to lash out at innocent people (or pets) in another.” The technical term for this kind of behaviour is “displaced aggression”.
Kicking the cat is looked upon unfavourably and viewed as a sign of poor anger management. According to author Steve Sonderman, “Men funnel 90 percent of their emotions through anger” and may “kick the cat” as a substitute for grief, anxiety or other emotions. Psychology author Raj Persaud suggests that people “kick the cat” as a means of catharsis because they fear expressing their full emotions to the peers and colleagues.
Kleine-Levin syndrome (KLS) is a rare disorder characterised by persistent episodic hypersomnia and cognitive or mood changes. Sometimes known as the Sleeping Beauty Syndrome.
Many patients also experience hyperphagia, hypersexuality and other symptoms. Patients generally experience recurrent episodes of the condition for more than a decade and may return at a later age. Individual episodes generally last more than a week, sometimes lasting for months. The condition greatly affects the personal, professional, and social lives of sufferers. The severity of symptoms and the course of the syndrome vary between sufferers. Patients commonly have about 20 episodes over about a decade. Several months generally elapse between episodes.
The onset of the condition usually follows a viral infection; several different viruses have been observed to trigger KLS. It is generally only diagnosed after similar conditions have been excluded; magnetic resonance imaging (MRI), computed tomography (CT) scans, lumbar puncture, and toxicology tests are used to rule out other possibilities. The syndrome’s mechanism is not known, but the thalamus is thought to possibly play a role. Single-photon emission computed tomography (SPECT) has shown thalamic hypoperfusion of patients during episodes.
KLS is very rare, occurring at a rate of 1 in 1 million, which limits research into genetic factors. The condition primarily affects adolescent males, though females can also be affected and the age of onset varies. There is no known cure, and there is little evidence supporting drug treatment. Lithium has been reported to have limited effects in case reports, decreasing the length of episodes and duration between them in some patients. Stimulants have been shown to promote wakefulness during episodes, but they do not counteract cognitive symptoms or decrease the duration of episodes. The condition is named after Willi Kleine and Max Levin, who described cases of the disease in the early 20th century. It was added to the International Classification of Sleep Disorders in 1990.
Brief History
In 1815, there was a report of a young man who showed excessive appetite and prolonged sleep after experiencing a fever; this may have been an early description of the condition. Another case with similar symptoms was described by Brierre de Boismont in 1862.
Five patients with symptoms of persistent sleepiness were described in detail in 1925 by Willi Kleine, a neurologist from Frankfurt. This report was followed four years later by details of a similar case by New York-based psychiatrist Max Levin. In 1935, Levin published information about several more cases, including one described by Kleine. Levin noted that some patients displayed an intense appetite in addition to their persistent tiredness. MacDonald Critchley, who first wrote about the condition in 1942, described 11 cases he had examined and reviewed 15 other published cases in a 1962 publication. In the report, which included patients he had examined in the Royal Navy during World War II, he observed that irritability and depersonalisation often occurred while patients were awake. He named the condition Kleine-Levin syndrome and noted four common traits: hypersexuality, adolescent onset, spontaneous resolution, and compulsive eating. He believed that the condition only affected males, but later studies showed some female patients. In the 1970s, several psychoanalytic and psychodynamic explanations for the condition were proposed. In 1980, a Hawaiian-Caucasian family was found in which nine family members suffered from the condition.
Diagnostic criteria for KLS was established by Schmidt in 1990, and the International Classification of Sleep Disorders further refined them. KLS is classified as a sleep disorder, specifically one of recurrent hypersomnia. Before 2005, hyperphagia and hypersexuality were thought to occur in all cases. That was changed with the guidelines published that year, which noted that they did not always occur.
Epidemiology
Population-based studies of KLS have not been performed. Its prevalence is about 1 case per million people. In France, KLS has a prevalence of 1.5 per million people. It occurs most frequently among Jews in the US and Israel. First-degree relatives of people who have suffered from the syndrome are much more likely than the general population to suffer from it, although only in about one percent of cases do family members contract it. About 70% to 90% of patients are male. Patients with the syndrome are more likely than the general population to have genetic disorders, and about a third of people with the syndrome encountered some form of birth difficulty. In a study of 186 older patients, about ten percent had pre-existing psychiatric issues. One study found that about ten percent of patients had a neurological condition before KLS developed. The condition does not appear to occur most frequently in one season.
Symptoms
Patients with KLS experience recurring episodes of prolonged sleep (hypersomnia). In most cases, patients sleep 15 to 21 hours a day during episodes. Excessive appetite (hyperphagia) and unusual cravings are present in half to two thirds of cases. About half of patients, mainly male patients, experience dramatically increased sexual urges (hypersexuality). Several other symptoms usually accompany the syndrome, including marked changes in mood and cognitive ability. Derealisation and severe apathy are present in at least 80% of cases. About one third of patients experience hallucinations or delusions. Depression and anxiety occur less commonly; one study found them in about 25% of patients. Individuals usually cannot remember what happened during episodes. Repetitive behaviours and headaches are commonly reported. Some patients act very childlike during episodes, and communication skills and coordination sometimes suffer.
Sleep studies of KLS show varying results based on the amount of time the patient is observed. Slow wave sleep is often reduced at the beginning of episodes, and rapid eye movement (REM) sleep is reduced near the end. Conversely, REM sleep is often normal at the beginning, and slow wave sleep is often normal by the conclusion. Stage two non-rapid eye movement sleep is often interrupted during KLS. Studies also show that stage one and three non-rapid eye movement sleep become more efficient when the episodes end. The Multiple Sleep Latency Test has yielded inconsistent results when given to KLS patients. In many cases, hours are spent in a withdrawn sleep-like state while awake during episodes. Most sleep studies have been performed while subject is near the end of their episodes. Some patients experience brief insomnia and become very happy and talkative after the episode ends.
The first time a patient experiences KLS, it usually occurs along with symptoms that are similar to those of the flu or encephalitis. In at least 75% of cases, symptoms occur after an airway infection or a fever. Viruses observed before the development of the condition include Epstein-Barr virus, varicella zoster virus, herpes zoster virus, influenza A virus subtypes, and adenovirus. Several days after symptoms first occur, patients become very tired. In cases that occur after an infection, KLS usually starts within three to five days for teenagers and fewer for children. In other cases, alcohol consumption, head injury, or international travel precede symptoms. Lifestyle habits, such as stress, alcohol abuse and lack of sleep and stress, have also been proposed as possible triggers. First episodes of KLS are preceded by a clear event in about 90% of cases. Recurrences generally do not have clear triggers; only about 15% have a precipitating event.
The condition generally disrupts the social lives and academic or professional obligations of sufferers. Some patients also gain weight during episodes. The most severe cases cause a long-term impact on mood and cognitive attention. In rare cases, patients experience long-term memory problems.
In patients with KLS, MRI and CT scans show normal brain morphology. When SPECT is performed, hypoperfusion can often be observed in the brain, particularly in the thalamic and frontotemporal areas. The hypoperfusion is significantly diminished between episodes. Serum biology, c-reactive proteins and leptins, the hormonal pituitary axis, and protein in the cerebral spinal fluid (CSF) are normal in KLS patients.
Cause
It is not known what causes KLS, but several mechanisms have been proposed. One possible explanation is hypothalamic or circadian dysfunction. The thalamus probably plays a role in the out-of-control sleeping, and patients with diencephalic-hypothalamic dysfunction caused by tumours experience symptoms similar to those of KLS patients. Specifically, the medial temporal regions of the thalamus may be involved, although examinations of KLS patients have not consistently found abnormalities in this area. The temporal lobe also appears to play a role in the condition, possibly causing cognitive difficulties. The apathy and disinhibition found in some KLS sufferers suggest that the condition may include frontal lobe dysfunction as well. The involvement of the thalamus, temporal lobe, and frontal lobe of the brain suggests that there is a multifocal, localised encephalopathy. There are also persistent subclinical abnormalities in KLS sufferers.
Another possible explanation concerns the metabolism of serotonin and dopamine. An imbalance in the neurotransmitter pathways of these chemicals could play a role. Viral infections have also been suggested as a possible cause. Evidence for their role includes lesions found in autopsies. Cerebral spinal fluid (CSF) samples from KLS patients indicate that the condition has a different cause than influenza-associated encephalopathy. Triggers of KLS may also affect the blood-brain barrier, which could play a role in the condition. There is limited evidence of what role hypocretin may play, although it often influences hypersomnia.
Androgen might (indirectly) block melatonin receptors, possibly by means of vasodilation, and cause cholinergic abnormalities in some cases of KLS.
Because KLS occurs at a much higher rate in Jews and in some families, it is likely that there is some genetic component in addition to environmental factors. Genetic studies hold promise for understanding the disease, but they have yielded inconsistent results and few patients are available for testing.
Epilepsy and depression do not appear to cause KLS. The condition’s rapid onset after infections indicates that the immune system is not to blame.
One study has suggested a link to the gene LMOD3 on chromosome 3.
Diagnosis
KLS can be diagnosed when there is confusion, apathy, or derealisation in addition to frequent bouts of extreme tiredness and prolonged sleep. The earliest it can be diagnosed is the second episode, this is not common. The condition is generally treated as a diagnosis of exclusion. Because KLS is rare, other conditions with similar symptoms are usually considered first.
MRIs can determine if the symptoms are caused by certain brain disorders, stroke, and multiple sclerosis. Lumbar puncture can determine if encephalitis is the cause. KLS must be differentiated from substance abuse by toxicology tests. The use of electroencephalography (EEG) can exclude temporal status epilepticus from consideration. EEGs are normal in about 70% of KLS patients, but background slowing may sometimes be detected. In addition, low-frequency high-amplitude waves can be observed during waking hours.
Initially, KLS appears similar to bipolar depression. Patients with frontal-lobe syndromes and Klüver-Bucy syndrome also display similar symptoms, but these conditions can be differentiated by the presence of brain lesions. KLS should also be distinguished from very rare cases of menstruation-caused hypersomnia.
Prevention
Lithium is the only drug that appears to have a preventive effect. In two studies of more than 100 patients, lithium helped prevent recurrence of symptoms in 20% to 40% of cases. The recommended blood level of lithium for KLS patients is 0.8-1.2 mEq/ml. It is not known if other mood stabilisers have an effect on the condition. Anti-depressants do not prevent recurrence.
Treatment
Several drug therapies have been used on patients with KLS, but none of them have been subject to randomized controlled trials. A 2016 Cochrane Review concluded that “No evidence indicates that pharmacological treatment for Kleine-Levin syndrome is effective and safe”.
In several cases, stimulants, including modafinil, have been reported to have a limited effect on patients, often alleviating sleepiness. They can cause behavioural problems, but they may pose fewer issues if used in older patients with mild symptoms. In some case reports, lithium has been reported to decrease the length of episodes and the severity of their symptoms and to increase the time between episodes. It has been reported to be effective in about 25 to 60% of cases. Its use carries the risk of side effects in the thyroid or kidneys. Antipsychotics and benzodiazepines can help alleviate psychotic and anxiety related symptoms, respectively. Carbamazepine has been reported to be less effective than lithium but more effective than some drugs in its class. Electroconvulsive therapy is not effective and worsens symptoms.
KLS patients generally do not need to be admitted to hospitals. It is recommended that caregivers reassure them and encourage them to maintain sleep hygiene. It may also be necessary for patients to be prevented from putting themselves in dangerous situations, such as driving.
Prognosis
The frequency of KLS episodes can vary from attacks one week in length occurring twice a year to dozens of episodes that follow each other in close succession. The median duration of KLS episodes is about ten days, but some last several weeks or months. A study of 108 patients found an average of 19 episodes over the duration of the disease. Another study found a median of 3.5 months between episodes. Outside of episodes, there is no disturbance in patients’ sleep patterns and they are generally asymptomatic. Patients do not experience the same symptoms in each episode.
About 80% of patients are adolescents when they first experience KLS. On some occasions though, its first occurrence comes in childhood or adulthood. In most adolescent-onset patients, symptoms cease by the time they are 30 years old. A French study of 108 patients found a median duration of 13 years, but a review of 186 cases found a median duration of 8 years. Unusually young or old patients and those who experience hypersexuality tend to have a more severe course. Patients who initially have frequent attacks generally see the disease cease earlier than others. The condition spontaneously resolves, and the patient is considered to be cured if there have been no symptoms for six years.
Herbert “Harry” Stack Sullivan (21 February 1892 to 14 January 1949) was an American Neo-Freudian psychiatrist and psychoanalyst who held that “personality can never be isolated from the complex interpersonal relationships in which [a] person lives” and that “[t]he field of psychiatry is the field of interpersonal relations under any and all circumstances in which [such] relations exist”.
Having studied therapists Sigmund Freud, Adolf Meyer, and William Alanson White, he devoted years of clinical and research work to helping people with psychotic illness.
Improving Access to Psychological Therapies (IAPT) is a National Health Service (England) initiative to provide more psychotherapy to the general population.
It was developed and introduced by the Labour Party as a result of economic evaluations by Professor Lord Richard Layard, based on new therapy guidelines from the National Institute for Health and Care Excellence as promoted by clinical psychologist David M. Clark.
Brief History
Richard Layard, a labour economist at the London School of Economics, had become influential in New Labour party politics and was appointed to the House of Lords in 2000. He had a particular interest in the happiness of populations and mental health; his father, John Layard, was an anthropologist who had survived suicidal depression and retrained as a Jungian psychologist after undergoing psychoanalysis by Carl Jung. In 2003 Richard Layard met the clinical psychologist David M. Clark, a leading figure in Cognitive Behavioural Therapy who was running the Centre for Anxiety Disorders and Trauma (with Anke Ehlers and Paul Salkovskis) at the Institute of Psychiatry and Maudsley Hospital. Clark professed to high rates of improvement from CBT but low availability of the therapy despite NICE guidelines now recommending it for several mental disorders.
Layard, with Clark’s help, set about campaigning for a new national service for NICE-recommended treatments, particularly CBT. One key argument was that it would be cost-effective and indeed eventually pay for itself by increasing productivity and reducing state benefits such as Disability Living Allowance and Incapacity Benefit (which had seen rising claims since their introduction by John Major’s Conservative Party in 1992 and 1995 respectively). The plan was accepted in principle by the newly re-elected Labour government in 2005 and gradually put into practice directed by Clark. Layard names several others as having helped gain the initial political traction for the initiative – MP Ed Miliband, psychiatrist Louis Appleby (then National Director for Mental Health), David Halpern (psychologist), psychiatrist David Nutt, MP Alan Milburn (married to a psychiatrist) and eventually the Prime Minister Gordon Brown.
In 2006 the Mental Health Policy Group at the LSE published ‘The Depression Report’, commonly referred to as the Layard Report, advocating for the expansion of psychotherapy on the NHS. This facilitated the development of IAPT initiatives, including two demonstration sites (pilot studies) and then training schemes for new types of psychological practitioner. The programme was officially announced in 2007 on World Mental Health Day. Some mental health professionals cast doubt on the claims early on. In the official publication of the British Psychological Society in 2009, experienced clinical psychologists John Marzillier and Professor John Hall strongly criticised IAPT’s promoters for glossing over both the data gaps acknowledged in the NICE reports and the complexity of the multiple issues typically affecting people with mental health problems and their ability to sustain employment; they were met with much agreement as well as angry criticism. One researcher cited the UK initiative as the most impressive plan to disseminate stepped-care cognitive behaviour therapy. But the plan appears not to have worked, Davis (2020) in the Journal of Evidence Based Mental Health, noted that 73% of IAPT clients receive low intensity therapy first (guided self help, computer assisted CBT or group psychoeducation) but only 4 % are transferred to high intensity therapy and the first transition appointment is the least well attended.
Aims
The aim of the project is to increase the provision of evidence-based treatments for common mental health conditions such as anxiety and depression by primary care organisations. This includes workforce planning to adequately train the mental health professionals required. This would be based on a ‘stepped care’ or triage model where ‘low intensity’ interventions or self-help would be provided to most people in the first instance and ‘high intensity’ interventions for more serious or complex conditions. Outcomes would be assessed by standardised questionnaires, where sufficiently high initial scores (a ‘case’) and sufficiently low scores immediately after treatment (below ‘caseness’), would be classed as ‘moving to recovery’. The NICE (National Institute for Health and Clinical Excellence) therapy guidelines presume reliable diagnosis. IAPT therapists do not make formal diagnoses. This calls into question IAPT’s claimed fidelity to the NICE guidelines, particularly as it does not monitor therapists treatment adherence.
Evaluation
Initial demonstration sites reported outcomes in line with predictions in terms of the number of people treated (especially with ‘low intensity’ interventions such as ‘guided self-help’) and the percentages classified as recovered and as in more employment (a small minority) to ten months later. It was noted that the literature indicates a substantial proportion of patients would recover anyway with the passage of time or with a placebo – in fact the majority of those whose condition had lasted for less than six months, but only a small minority of those whose condition had been longer-lasting.
There has been some debate over whether IAPT’s roll-out may result initially in low quality therapy being offered by poorly trained practitioners.
Beacon UK benchmarked IAPT performance across England for 2011-2012 and reported that 533,550 people accessed (were referred to) IAPT services – 8.7% of people suffering from anxiety and depression disorders – with around 60% entering treatment sessions. Most local IAPT services did not reach the target of a 50% ‘recovery’ rate.
In 2012-2013, 761,848 people were referred to IAPT services. 49% went into treatment (the rest either assessed as unsuitable for IAPT or declined), although around half of those dropped out before completing at least two sessions. Of the remainder, 127,060 people had pre-treatment and post-treatment mental health questionnaires submitted indicating ‘recovery’ – a headline rate of 43%. A report by the University of Chester indicated that sessions were costing three times more to fund than the original Department of Health estimates.
For 2014-2015 there were nearly 1.3 million referrals to IAPT, of which 815,665 entered treatment. Of those, 37% completed sufficient sessions, with 180,300 showing a ‘reliable recovery’ (on anxiety and depression questionnaires completed before and immediately after treatment) – which was just over one in five of those who entered treatment, just under half of those who completed enough sessions. Opinion on IAPT remained divided. The number of trained IAPT therapists did not appear to have met the government’s target of 6000, resulting in high caseloads. Some complained of seeing more ‘revolving door’ patients and excess complexity of cases, while the NHS has acknowledged problems with waiting times and recovery rates. However Norman Lamb, who championed IAPT within the coalition government 2010-2015, disagreed with picking faults with such an extensive and world-leading advance in evidence-based treatment. Others lauded the success in rising numbers of referrals, but warned of the failure to improve recovery rates. It was noted that both antidepressant prescribing and psychiatric disability claims have continued to rise.
In 2017 fewer than half of the Clinical Commissioning Groups met the target (15.8%) for the number of people who should be accessing talking therapies. There has been no publicly funded independent audit of IAPT . A study of 90 IAPT cases assessed with a ‘gold standard’ diagnostic interview revealed that only the tip of the iceberg recovered, in the sense of losing their diagnostic status. The results were identical whether or not the person was treated before or after personal injury litigation.
In July 2021 55,703 appointments out of the total 434,000 which went ahead involved one or more practitioners who did not have an accredited IAPT qualification. There are about 2000 psychological wellbeing practitioners in the service, with another 1,200 trainees. They are supported by high intensity therapists and counsellors of which there are about 4,000 with 700 trainees.
Updates
In December 2010, Paul Burstow, Minister for Care Services, announced an extension to the IAPT project to include Children and Young Peoples services. The government pledged £118m annually from 2015 to 2019 to increase access to psychological therapies services to children and young people.
When the programme officially started in 2008 it was only for working age adults, but in 2010 it was opened to all ages.
In 2015 Clark and fellow clinical psychologist Peter Fonagy, writing in response to wide-ranging criticism from child and adolescent psychiatrist Sami Timimi, stated that IAPT now has increasing support for the non-CBT modalities recommended by NICE for depression: counselling, couples therapy, interpersonal psychotherapy and brief psychodynamic therapy; and for Children and Young People (CYP-IAPT) more systemic family therapy, interpersonal therapy and parenting therapy is on the way. Timimi described the changes as still “light” on relational/collaborative therapy compared to the ‘technical model’ derived from ’eminence-based’ NICE guidelines via inadequate diagnostic categories.
A Payment by Results system is being developed for IAPT, whereby each local Clinical Commissioning Group can reward each local provider according to various targets met for the service and for each client – particularly for how much change in scores on the self-report questionnaires. The March 2021 issue of the British Journal of Clinical Psychology has highlighted the considerable controversy over IAPT’s claims of success, Scott( 2021) and Kellett et al., (2021) have responded with their own commentary ‘The costs and benefits of practice-based evidence: Correcting some misunderstandings about the 10-year meta-analysis of IAPT studies’.
Identification is a psychological process whereby the individual assimilates an aspect, property, or attribute of the other and is transformed wholly or partially by the model that other provides.
It is by means of a series of identifications that the personality is constituted and specified. The roots of the concept can be found in Freud‘s writings. The three most prominent concepts of identification as described by Freud are:
Primary identification;
Narcissistic (secondary) identification; and
Partial (secondary) identification.
While “in the psychoanalytic literature there is agreement that the core meaning of identification is simple – to be like or to become like another”, it has also been adjudged ‘”the most perplexing clinical/theoretical area” in psychoanalysis’.
Freud
Freud first raised the matter of identification (German: Identifizierung) in 1897, in connection with the illness or death of one’s parents, and the response “to punish oneself in a hysterical fashion…with the same states [of illness] that they have had. The identification which occurs here is, as we can see, nothing other than a mode of thinking”. The question was taken up again psychoanalytically “in Ferenczi’s article, ‘Introjection and Transference’, dating from 1909”, but it was in the decade between “On Narcissism” (1914) and “The Ego and the Id” (1923) that Freud made his most detailed and intensive study of the concept.
Freud distinguished three main kinds of identification. “First, identification is the original form of emotional tie with an object; secondly, in a regressive way it becomes a substitute for a libidinal object-tie…and thirdly, it may arise with any new perception of a common quality which is shared with some other person”.
Primary Identification
Primary identification is the original and primitive form of emotional attachment to something or someone prior to any relations with other persons or objects: “an individual’s first and most important identification, his identification with the father in his own personal prehistory…with the parents”. This means that when a baby is born he is not capable of making a distinction between himself and important others. The baby has an emotional attachment with his parents and experiences his parents as a part of himself. “The breast is part of me, I am the breast”.
During this process of identification children adopt unconsciously the characteristics of their parents and begin to associate themselves with and copy the behaviour of their parents. Freud remarked that identification should be distinguished from imitation, which is a voluntary and conscious act. Because of this process of emotional attachment a child will develop a super ego that has similarities to the moral values and guidelines by which the parents live their lives. By this process children become a great deal like their parents and this facilitates learning to live in the world and culture to which they are born.
“By and large, psychoanalysts grant the importance and centrality of primary identification, even though…the concept varies ‘according to each author and his ideas, its meaning in consequence being far from precise’ (Etchegoyen 1985)”.
Narcissistic (Secondary) Identification
Narcissistic identification is the form of identification following abandonment or loss of an object. This experience of loss starts at a very young age. An example: wearing the clothes or jewellery of a deceased loved one. In “Mourning and Melancholia” Freud, having “shown that identification is a preliminary stage of object-choice”, argued that the experience of loss sets in motion a regressive process that “served to establish an identification of the ego with the abandoned object”. In “The Ego and the Id”, he went on to maintain that “this kind of substitution has a great share in determining the form taken by the ego and that it makes an essential contribution towards building up what is called its ‘character'”.
Lacan, in his theory of the Imaginary, would develop the latter point into his view of “the ego is constituted in its nucleus by a series of alienating identifications” – part of his opposition to any concept of an “autonomous” and conflict-free ego.
Partial (Secondary) Identification
Partial identification is based on the perception of a special quality of another person. This quality or ideal is often represented in a “leader figure” who is identified with. For example: the young boy identifies with the strong muscles of an older neighbour boy. Next to identification with the leader, people identify with others because they feel they have something in common. For example: a group of people who like the same music. This mechanism plays an important role in the formation of groups. It contributes to the development of character and the ego is formed by identification with a group (group norms). Partial identification promotes the social life of persons who will be able to identify with one another through this common bond to one another, instead of considering someone as a rival.
Partial Identification and Empathy
Freud went on to indicate the way “a path leads from identification by way of imitation to empathy, that is, to the comprehension of the mechanism by which we are enabled to take up any attitude at all towards another mental life”. Otto Fenichel would go on to emphasize how “trial identifications for the purposes of empathy play a basic part in normal object relationships. They can be studied especially in analyzing the psychoanalyst’s ways of working”. Object relations theory would subsequently highlight the use of “trial identification with the patient in the session” as part of the growing technique of analysing from the countertransference.
Anna Freud and Identification with the Aggressor
In her classic book The Ego and the Mechanism of Defence, Anna Freud introduced “two original defence mechanisms…both of which have become classics of ego psychology“, the one being altruistic surrender, the other identification with the aggressor. Anna Freud pointed out that identification with parental values was a normal part of the development of the superego; but that “if the child introjects both rebuke and punishment and then regularly projects this same punishment on another, ‘then he is arrested at an intermediate stage in the development of the superego'”.
The concept was also taken up in object relations theory, which particularly explored “how a patient sometimes places the analyst in the role of victim whilst the patient acts out an identification with the aggressor” in the analytic situation.
With the Analyst
Mainstream analytic thought broadly agrees that interpretation took effect “by utilizing positive transference and transitory identifications with the analyst”. More controversial, however, was the concept of “the terminal identification” at the close of analysis, where “that with which the patient identifies is their strong ego…[or] identification with the analyst’s superego”.
Lacan took strong exception to “any analysis that one teaches as having to be terminated by identification with the analyst…There is a beyond to this identification…this crossing of the plane of identification”. Most Lacanians have subsequently echoed his distrust of “the view of psychoanalysis that relies on identification with the analyst as a central curative factor”. How far the same criticism applies, however, to those who see as a positive therapeutic result “the development of a self-analytic attitude…[built on] identification with and internalization of the analyst’s analytic attitude” is not perhaps quite clear.
Marion Milner has argued that “terminal identification” can be most acute in those analysands who go on to become therapists themselves: “by the mere fact of becoming analysts we have succeeded in bypassing an experience which our patients have to go through. We have chosen to identify with our analyst’s profession and to act out that identification”.
Contemporary Psychoanalytic Thinking
Much has been written on identification since Freud. Identification has been seen both as a normal developmental mechanism and as a mechanism of defence. Many types of identification have been described by other psychoanalysts, including counter-identification (Fliess, 1953), pseudoidentification (Eidelberg, 1938), concordant and complementary identifications (Racker, 1957), and adhesive identification (Bick, 1968): “the work of Bick and others on adhesive identification, exploring the concept of the ‘psychic skin'”.
The Icarus Project was a media and activist endeavour broadly aligned to the anti-psychiatry movement and recovery approach, arguing that mental illness should be understood as an issue of social justice and that a person’s mental state can improve through greater social support and collective liberation.
It shares similarities with the academic fields of Psychopolitics and Mad Studies. The name is derived from Icarus, a hero in Greek mythology, and is metaphorically used to convey that the experiences of mental distress and other extreme mental states can lead to “potential[ly] flying dangerously close to the sun.”
Brief History
In 2002, musician Sascha Altman DuBrul wrote “Bipolar World”, an article published in the San Francisco Bay Guardian. The article described his experiences being diagnosed with bipolar disorder. Among the dozens of e-mails and other correspondence that he received after this publication was a letter from Ashley McNamara, now known as Jacks, an artist and writer who identified strongly with DuBrul’s experiences. DuBrul and McNamara corresponded for a few weeks before finally meeting in person and deciding to start The Icarus Project. Years later, musician-activist Bonfire Madigan Shive and counsellor/activist Will Hall became a key leader in The Icarus Project’s administration and development.
In the Journal of Medical Humanities, co-founder DuBrul wrote of The Icarus Project:
Though we did not fully understand it in the early days, we were walking in the footsteps of a large body of knowledge and thought from the 1960s, grouped under the category of Anti-Psychiatry.
He also noted the group and its members were inspired by a range of social trends and schools of thought including anarchism, permaculture/sustainable ecology, LGBTQ rights, harm reduction, global justice movement, the Beat Generation, counterculture, and punk rock. He writes, “Our response to the label ‘bipolar’ was not a ‘normal’ response, which is why the Icarus Project brought a new perspective to psychic diversity. To create this perspective, we drew inspiration from many social movements and subcultural communities that came before us. So even though our response was unusual, it did not arise in a vacuum. In creating the Icarus Project, we wove together the ideas and practices in these movements to imagine a powerful new counter narrative to the dominant mental health narrative that went beyond a questioning of the language around ‘bipolar’ and critiqued the system itself.”
The first step, they decided, was creating a website where people who identified with “bipolar and other ‘mental illness’ [could] find real community and contribute to it.” DuBrul states that by 2003, “The Icarus Project website was up and running, and a virtual community began to evolve around the discussion forums.” He notes that user-generated content online enabled The Icarus Project’s growth: “We were attracting interesting people, creating discussion forums with names like ‘Alternate Dimensions or Psychotic Delusions’ and ‘Experiencing Madness and Extreme States.’ There was no place else where people who used psych meds and people who did not, people who identified with diagnostic categories and people who did not, could all talk with each other and share stories. Because of the outreach in the anarchist and activist community, there was a high percentage of creative people with a radical political analysis. And with the (seeming) anonymity of the Internet, people felt comfortable being honest and sharing intimate stories about their lives. Our website served as a refuge for a diverse group of people who were learning the ways in which new narratives could be woven about their lives.”
Mission
The Icarus Project’s stated aims are to provide a “support network and education project by and for people who experience the world in ways that are often diagnosed as mental illness.” The national Icarus Collective staff is set up to support local groups instead of creating the smaller organisations themselves. The responsibilities of the local group are to gather people locally for support, education, activism, and access to alternatives to mainstream medical diagnosis and treatment. The Project advocates self-determination and caution when approaching psychiatric care. It encourages harm reduction, alternatives to the prevailing medical model that is accepted by the vast majority of mental health professionals, and self-determination in treatment and diagnosis. Key members of The Icarus Project state that they “envision a world with more options to navigate mental health issues: options that support self-determination, centre people who are most impacted by mental health-based oppression, and most critically, uplift social transformation as central to individual wellbeing.”
In 2005, Journalist Jennifer Itzenson noted that the Icarus Project accepts those with a wide range of perspectives on mental health issues, but also describes “an edge of militancy within the group,” particularly among those who reject medication. Itzenson also writes that while medical professionals applaud groups like the Icarus Project for providing a sense of support and community, and combating social stigmas related to bipolar and other mental health issues, the group’s questioning of the medical paradigm is “misguided” and that rejecting medication is a “potentially fatal choice” for those with bipolar disorder. A Newsweek article provides the following perspective on The Icarus Project’s stance towards medication: “While some critics might view Icaristas as irresponsible, their skepticism about drugs isn’t entirely unfounded. Lately, a number of antipsychotic drugs have been found to cause some troubling side effects.”
Writer Mark Lukach describes in an article for Pacific Standard his experience asking co-founder Sascha Altman DuBrul about the role of psychiatric medication as a part of his wife’s recovery from a bipolar diagnosis. Lukach articulates The Icarus Project’s approach to self-determination in psychiatric treatment. Lukach wrote:
“As for medication, DuBrul said that he believed that the answer to the question of whether or not to use pharmaceuticals needed to be far more nuanced than yes or no. The best response might be maybe, sometimes, or only certain medications. For instance, DuBrul shared that he takes lithium every night because he’s confident that, after four hospitalizations and over a decade with the label bipolar, the medication is a positive part of his care. Not the whole solution, but a piece.”
Anthropologist Erica Hua Fletcher describes Icarus Project member’s diverse ways of discussing altered mental states in the Journal of Medical Humanities. Fletcher writes:
While many Icarus contributors have found relief through the use of psycho-pharmaceutical interventions and other bio-psychiatric technologies, they also have experienced the limitations of medical paradigms and language to recognize the fullness of their lives. Because of this, they frequently adopt alternative words and phrases beyond bio-psychiatric terms to describe their mental states such as “neurodivergent processing,” “diasporas of distressing symptoms,” “sensory/cognitive/emotional trauma,” or “cognitive-emotional terror.” “Bipolar disorder” is interchangeable with highs and lows; “psychosis” can be seen as a reckoning; and nonconsensus realities can describe extreme experiences, which psychiatrists could label as symptoms of “schizophrenia” (such as hearing voices others do not hear or seeing objects others do not see). Such alternative words and phrases do not diminish the utility of bio- psychiatric terminology nor do they directly undermine medical treatment options, yet they allow for a range of descriptors and call for attention to individual needs and desires. They call us to listen to personal stories, to forces at work within communities, and to reevaluate the languages that enframe mental illness as such.” She goes on to state, “Alternative language beyond the biomedical paradigm of mental illness fosters a diversity of paradigms. Moreover, it can create a reflective space for those with mental suffering (and for their healthcare providers) to see themselves outside of a medical identity, reevaluate their self-care regimens, advocate for the care they would like to receive, and connect to others who may have similar concerns about ascribing to solely psycho-pharmaceutical interventions.”
As of early 2018, Icarus Project staff describe their expertise in social activism, herbalism, and labour organising; none is a licensed medical or mental health professional. Icarus Project advisory board members describe themselves as educators, artists, activists, writers, healers, community organisers, and other creative types and some identify as Latinx, queer, trans, people of colour or mixed race, and trauma survivors; none is a licensed medical or mental health professional. Leadership currently offers publications on self-care and community care, workshops and training for peers, training and talks for providers, peer support spaces, webinars, and other events.
Structure/Funding
The Icarus Project is currently under the fiscal sponsorship of FJC, a non-profit 501(c)3 umbrella organization arm of an investment firm, based in New York City. The Icarus Project currently gets the bulk of its money from foundation grants, including the Ittleson Foundation, but it also has many individual donors.
The Icarus Project Network
Places where local chapters met included Anchorage, Alaska; Asheville, North Carolina; Atlanta, Georgia; Boston, Massachusetts; Conway, Arkansas; Chicago, Illinois; Los Angeles, California (Wildflowers’ Movement); Minneapolis, Minnesota; Madison, Wisconsin; New York City, New York; Northampton, Massachusetts (Freedom Centre); Philadelphia, Pennsylvania; Portland, Oregon; San Francisco (Bay Area), California; Columbus, Ohio; Gainesville, Florida.
Media Mentions
The Icarus Project has been mentioned in passing in The New York Times as a resource for those who “don’t want to ‘get better'”, by Frontline 20/20, and many local media outlets.
Publications
Educational materials published by The Icarus Project have been published in Spanish, German, French, Italian, Japanese, Greek, and Bosnian/Croatian. Some of these publications are listed below:
In March 2004, The Icarus Project released Navigating the Space Between Brilliance and Madness; A Reader and Roadmap of Bipolar Worlds. The book is currently in its 6th printing.
In July 2006, The Icarus Project released the first draft of Friends Make the Best Medicine: A Guide to Creating Community Mental Health Support Networks.
In 2008, The Icarus Project released Through the Labyrinth; A Harm Reduction Guide to Coming Off Psychiatric Drugs, and in 2009 this publication was translated into Spanish and German and made available for free download on the Icarus Project website.
In 2012, The Icarus Project released Mindful Occupation: Rising Up without Burning Out.
In 2015, The Icarus Project released Madness and Oppression: Personal Paths to Transformation and Collective Liberation.
Filmography
Films about Icarus Project members are listed below:
Ken Paul Rosenthal (2010). Crooked Beauty. 30 min. Poetic documentary featuring Jacks McNamara. In Mad Dance Mental Health Film Trilogy.
Ken Paul Rosenthal (2018). Whisper Rapture. 36 min. A doc-opera featuring Bonfire Madigan Shive.
Hostile attribution bias, or hostile attribution of intent, is the tendency to interpret others’ behaviours as having hostile intent, even when the behaviour is ambiguous or benign.
For example, a person with high levels of hostile attribution bias might see two people laughing and immediately interpret this behaviour as two people laughing about them, even though the behaviour was ambiguous and may have been benign.
The term “hostile attribution bias” was first coined in 1980 by Nasby, Hayden, and DePaulo who noticed, along with several other key pioneers in this research area (e.g. Kenneth A. Dodge), that a subgroup of children tend to attribute hostile intent to ambiguous social situations more often than other children. Since then, hostile attribution bias has been conceptualized as a bias of social information processing (similar to other attribution biases), including the way individuals perceive, interpret, and select responses to situations. While occasional hostile attribution bias is normative (particularly for younger children), researchers have found that individuals who exhibit consistent and high levels of hostile attribution bias across development are much more likely to engage in aggressive behaviour (e.g. hitting/fighting, reacting violently, verbal or relational aggression) toward others.
In addition, hostile attribution bias is hypothesized to be one important pathway through which other risk factors, such as peer rejection or harsh parenting behaviour, lead to aggression. For example, children exposed to peer teasing at school or child abuse at home are much more likely to develop high levels of hostile attribution bias, which then lead them to behave aggressively at school and/or at home. Thus, in addition to partially explaining one way aggression develops, hostile attribution bias also represents a target for the intervention and prevention of aggressive behaviours.
Brief History
The term hostile attribution bias first emerged in 1980 when researchers began noticing that some children, particularly aggressive and/or rejected children, tended to interpret social situations differently compared to other children. For example, Nasby and colleagues presented photographs of people to a group of aggressive adolescent boys (aged 10-16) and observed that a subgroup of these youth exhibited a consistent tendency to attribute hostile intent to the photographs, even when the cues were ambiguous or benign. Similarly, Kenneth A. Dodge and colleagues conducted a study on a sample of school-aged children between 3rd-5th grade and found that children who were rejected were much more likely than other children to exhibit hostile attributions of intent to ambiguous social situations (e.g. when a behaviour could have been either accidental or intentional). Furthermore, Dodge and colleagues found that children with high hostile attribution bias then went on to exhibit the most aggressive behaviours later on.
Early studies investigating links between hostile attribution bias and aggression were somewhat mixed, with some studies reporting no significant effects or small effects and other studies reporting large effects. Since then, over 100 studies and a meta-analysis have documented a robust association between hostile attribution bias and aggressive behaviour across various samples ranging in age, gender, race, countries, and clinical populations.
Theoretical Formulation
Hostile attribution bias is typically conceptualised within a social information processing framework, in which social information (e.g. during an interaction) is processed in a series of steps that leads to a behavioural reaction. Accurate social information processing requires a person to engage in six steps that occur in order.
Step
1
Accurately encode information in the brain and store it in short-term memory. During this step, an individual will pay attention to and code specific stimuli/cues in their environment, including external factors (e.g. someone bumping into you; other people’s reactions to the situation) and internal factors (e.g. your affective reaction to the situation).
2
Accurately interpret or give meaning to encoded information. During this step, an individual may decide if a behaviour or situation was meant to be hostile or benign.
3
Decide a goal for the interaction.
4
Generate potential responses.
5
Evaluate potential responses and select the “optimal” response.
6
Enact chosen response.
Hostile attribution bias is theorised to result from deviations in any of these steps, including paying attention to and encoding biased information (e.g. only paying attention to cues suggestive of hostility), biases toward negative interpretations of social interactions (e.g. more likely to interpret situation as hostile), limited ability to generate a broad range of potential responses, and difficulty appropriately evaluating responses and selecting an optimal response. Furthermore, biases in any of the steps affect the rest of the steps. Hostile attribution bias has been particularly linked to step 2 of social information processing (i.e. interpretation of information), but is linked to impairments in other steps as well, including inaccurate perception/encoding of social situations and problems with generating a broad range of potential behavioural responses. For example, a child with high levels of hostile attribution bias may generate fewer potential responses than other children, and these responses may be limited to hostile or ineffective responses to a situation.
Dodge theorised that hostile attribution bias arises from an individual’s hostile schemas about the world that are formed through an interaction between a child’s neural dispositions and his/her early exposures to hostile socialisation experiences. These experiences may include disrupted parental attachment, child abuse, exposure to family violence, peer rejection or victimization, and community violence.
Measurement
In research settings, hostile attribution bias is typically measured with a laboratory task, in which participants are presented with staged interaction (live actors), video, picture, audio, or written presentations of ambiguous social situations. For example, an ambiguous social situation presented might be a video of a child opening a door, causing the door to knock over a tower of toys that another child was building. After the stimulus is presented, participants would be asked to make attributions about the intent of the actor (i.e. hostile vs. benign). (For example: “Do you think the girl who opened the door was trying to be mean, nice, or could have been mean or nice?”).
Multiple trials are administered with various ambiguous scenarios, and these attributions are then used by the researchers to determine the level of the child’s hostile attribution bias. Careful selection of stimuli and comparison of stimuli across mediums is helpful for accurately assessing an individual’s level of hostile attribution bias. A meta-analysis investigating the link between hostile attribution bias and aggressive behaviour found that the strongest effect sizes were linked with actual staging of social interactions, followed by audio presentation of stimuli, then video and picture presentation.
Implications
Aggression
Substantial literature has documented a robust association between hostile attribution bias and aggression in youth. Hostile attribution bias is traditionally associated with overt physical aggression (e.g. hitting, fighting), such that higher levels of hostile attribution bias predict more aggressive behaviour. In particular, much evidence suggests that hostile attribution bias is especially linked to “reactive aggression” (i.e. impulsive and “hot-blooded” aggression that reflects an angry retaliation to perceived provocation) rather than “proactive aggression” (i.e. unprovoked, planned/instrumental, or “cold-blooded” aggression). Beyond physical aggression, elevated hostile attribution bias is also associated with increased use of relational aggression (e.g. gossip, spreading rumours, social exclusion). This is particularly the case when youth attribute hostile intent to ambiguous relational situations (e.g. not receiving an invitation to a party or not receiving a response to a text).
Negative Adult Outcomes
Hostile attribution bias has also been documented in adult populations, and adults with high levels of hostile attribution bias are over 4 times more likely to die by the age of 50 than adults with low levels of hostile attribution bias. Hostile attribution bias is particularly linked to relational problems in adulthood, including marital conflict/violence and marital/relationship dissatisfaction. Finally, parents with high levels of hostile attribution bias are also much more likely to use harsh discipline and aggressive parenting, which may further contribute to the intergenerational continuity in hostile attribution bias and aggression across time.
Clinical Implications for Intervention
Hostile attribution bias has been tested as a malleable target for intervention for aggressive behaviours in youth, including in cognitive interventions designed to increase accurate identification of others’ intentions and attribution of benign intentions. Relative success has been documented from these interventions in changing levels of hostile attribution bias, although actual enduring changes in aggressive behaviour have been modest.
The concept has its origins as far back as the year 1889, when the German psychiatrist Emil Kraepelin first used the term of “periodic mania” to refer to people with recurrent manic episodes and no depression. One year later, Carl Wernicke proposed that mania and depression should be viewed as separate disorders. As the time went on, unipolar mania became an invalid diagnosis due to its variations across different patients. Currently patients with symptoms of mania, even in the absence of any depressive symptoms, would get the bipolar 1 diagnosis.
Symptoms
Symptoms of unipolar mania are similar to those of bipolar mania. They can include:
Excessive involvement in activities with a high likelihood of painful consequences.(e.g. extravagant shopping, improbable commercial schemes, hypersexuality).
The episode generally have a stronger tendency to present with psychosis or/and need psychiatric assistance.
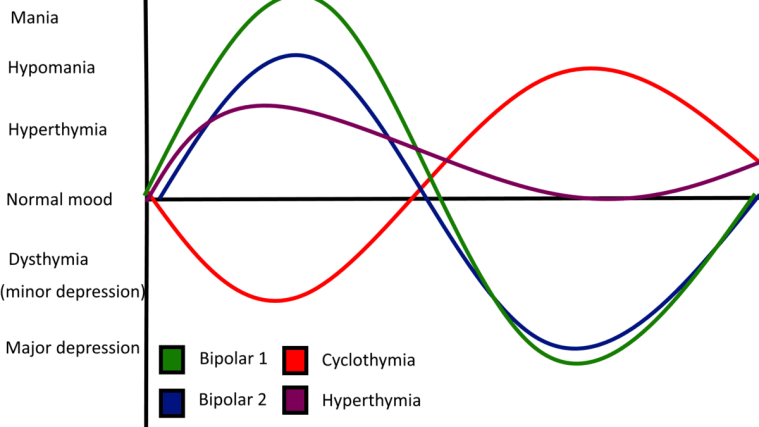
Hyperthymic temperament, or hyperthymia, from Ancient Greek ὑπέρ (“over”, meaning here excessive) + θυμός (“spirited”), is a proposed personality type characterised by an exceptionally, or in some cases, abnormally positive mood and disposition.
Also known as Hyperthymic Personality-Type and Chronic Hypomania.
Graph showing showing hyperthymia in comparison to other bipolar spectrum disorders.
Background
It is generally defined by increased energy, vividness and enthusiasm for life activities, as opposed to dysthymia. Hyperthymia is similar to but more stable than hypomania.
Characteristics of the hyperthymic temperament include:
Increased energy and productivity.
Short sleep patterns.
Vividness, activity extroversion.
Self-assurance, self-confidence.
Strong will.
Extreme talkativeness.
Tendency to repeat oneself.
Risk-taking/sensation seeking.
Breaking social norms.
Very strong libido.
Love of attention.
Low threshold for boredom.
Generosity and tendency to overspend.
Emotion sensitivity.
Cheerfulness and joviality.
Unusual warmth.
Expansiveness.
Tirelessness.
Irrepressibility, irresistible, and infectious quality.
The clinical, psychiatric understanding of hyperthymia is evolving. Studies have shown that hyperthymic temperament promotes efficient performance of complex tasks under time pressure or extreme conditions. Despite this positive characterisation, hyperthymia can be complicated with depressive episodes manifesting as a softer form of bipolar illness, such as cyclothymia. Research also suggests a familial genetic connection of the temperament to bipolar I.
Aside from references in historical and more recent writings on the spectrum of mood disorders, further literature on the temperament is lacking. There is a lack of agreement on its definition, implications or whether it is pathological. It is not known where to place hyperthymia on the affective spectrum.
Hyperthymia manifesting intermittently or in an unusual way may mask hypomania or another psychiatric disorder. Hyperthymia can be most accurately diagnosed by a psychologist or psychiatrist with the help of a patient’s family and/or close friends.



You must be logged in to post a comment.