Self-defeating personality disorder (also known as masochistic personality disorder) was a proposed personality disorder.
It was discussed in an appendix of the revised third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R) in 1987, but was never formally admitted into the manual. As an alternative, the diagnosis personality disorder not otherwise specified remains in use in the DSM-5. A classification proposed for future versions is the personality disorder-trait specified (PD-TS). Some researchers and theorists continue to use the DSM-III-R criteria. The official diagnostic code number was 301.90 (personality disorder NOS).
Definition Proposed in DSM III-R for Further Review
Self-defeating personality disorder is:
A) A pervasive pattern of self-defeating behaviour, beginning by early adulthood and present in a variety of contexts. The person may often avoid or undermine pleasurable experiences, be drawn to situations or relationships in which they will suffer, and prevent others from helping them, as indicated by at least five of the following:
Chooses people and situations that lead to disappointment, failure, or mistreatment even when better options are clearly available.
Rejects or makes ineffective the attempts of others to help them.
Following positive personal events (e.g. new achievement), responds with depression, guilt, or a behaviour that produces pain (e.g. an accident).
Incites angry or rejecting responses from others and then feels hurt, defeated, or humiliated (e.g. makes fun of spouse in public, provoking an angry retort, then feels devastated).
Rejects opportunities for pleasure, or is reluctant to acknowledge enjoying themselves (despite having adequate social skills and the capacity for pleasure).
Fails to accomplish tasks crucial to their personal objectives despite having demonstrated ability to do so (e.g., helps fellow students write papers, but is unable to write their own).
Is uninterested in or rejects people who consistently treat them well.
Engages in excessive self-sacrifice that is unsolicited by the intended recipients of the sacrifice.
The person may often avoid or undermine pleasurable experiences […]
B) The behaviors in A do not occur exclusively in response to, or in anticipation of, being physically, sexually, or psychologically abused.
C) The behaviors in A do not occur only when the person is depressed.
Exclusion from DSM-IV
Historically, masochism has been associated with feminine submissiveness. This disorder became politically controversial when associated with domestic violence which was considered to be mostly caused by males. However a number of studies suggest that the disorder is common. In spite of its exclusion from DSM-IV in 1994, it continues to enjoy widespread currency amongst clinicians as a construct that explains a great many facets of human behaviour.
Sexual masochism that “causes clinically significant distress or impairment in social, occupational, or other important areas of functioning” is still in DSM-IV.
A spectrum disorder is a mental disorder that includes a range of linked conditions, sometimes also extending to include singular symptoms and traits.
The different elements of a spectrum either have a similar appearance or are thought to be caused by the same underlying mechanism. In either case, a spectrum approach is taken because there appears to be “not a unitary disorder but rather a syndrome composed of subgroups”. The spectrum may represent a range of severity, comprising relatively “severe” mental disorders through to relatively “mild and nonclinical deficits”.
In some cases, a spectrum approach joins together conditions that were previously considered separately. A notable example of this trend is the autism spectrum, where conditions on this spectrum may now all be referred to as autism spectrum disorders. A spectrum approach may also expand the type or the severity of issues which are included, which may lessen the gap with other diagnoses or with what is considered “normal”. Proponents of this approach argue that it is in line with evidence of gradations in the type or severity of symptoms in the general population.
Origin
The term spectrum was originally used in physics to indicate an apparent qualitative distinction arising from a quantitative continuum (i.e. a series of distinct colours experienced when a beam of white light is dispersed by a prism according to wavelength). Isaac Newton first used the word spectrum (Latin for “appearance” or “apparition”) in print in 1671, in describing his experiments in optics.
The term was first used by analogy in psychiatry with a slightly different connotation, to identify a group of conditions that is qualitatively distinct in appearance but believed to be related from an underlying pathogenic point of view. It has been noted that for clinicians trained after the publication of DSM-III (1980), the spectrum concept in psychiatry may be relatively new, but that it has a long and distinguished history that dates back to Emil Kraepelin and beyond. A dimensional concept was proposed by Ernst Kretschmer in 1921 for schizophrenia (schizothymic – schizoid – schizophrenic) and for affective disorders (cyclothymic temperament – cycloid ‘psychopathy’ – manic-depressive disorder), as well as by Eugen Bleuler in 1922. The term “spectrum” was first used in psychiatry in 1968 in regard to a postulated schizophrenia spectrum, at that time meaning a linking together of what were then called “schizoid personalities”, in people diagnosed with schizophrenia and their genetic relatives (refer to Seymour S. Kety).
For different investigators, the hypothetical common disease-causing link has been of a different nature.
Related Concepts
A spectrum approach generally overlays or extends a categorical approach, which today is most associated with the Diagnostic and Statistical Manual of Mental Disorders (DSM) and International Statistical Classification of Diseases (ICD). In these diagnostic guides, disorders are considered present if there is a certain combination and number of symptoms. Gradations of present versus absent are not allowed, although there may be subtypes of severity within a category. The categories are also polythetic, because a constellation of symptoms is laid out and different patterns of them can qualify for the same diagnosis. These categories are aids important for our practical purposes such as providing specific labels to facilitate payments for mental health professionals. They have been described as clearly worded, with observable criteria, and therefore an advance over some previous models for research purposes.
A spectrum approach sometimes starts with the nuclear, classic DSM diagnostic criteria for a disorder (or may join together several disorders), and then include an additional broad range of issues such as temperaments or traits, lifestyle, behavioural patterns, and personality characteristics.
In addition, the term ‘spectrum’ may be used interchangeably with continuum, although the latter goes further in suggesting a direct straight line with no significant discontinuities. Under some continuum models, there are no set types or categories at all, only different dimensions along which everyone varies (hence a dimensional approach).
An example can be found in personality or temperament models. For example, a model that was derived from linguistic expressions of individual differences is subdivided into the Big Five personality traits, where everyone can be assigned a score along each of the five dimensions. This is by contrast to models of ‘personality types’ or temperament, where some have a certain type and some do not. Similarly, in the classification of mental disorders, a dimensional approach, which is being considered for the DSM-V, would involve everyone having a score on personality trait measures. A categorical approach would only look for the presence or absence of certain clusters of symptoms, perhaps with some cut-off points for severity for some symptoms only, and as a result diagnose some people with personality disorders.
A spectrum approach, by comparison, suggests that although there is a common underlying link, which could be continuous, particular sets of individuals present with particular patterns of symptoms (i.e. syndrome or subtype), reminiscent of the visible spectrum of distinct colours after refraction of light by a prism.
It has been argued that within the data used to develop the DSM system there is a large literature leading to the conclusion that a spectrum classification provides a better perspective on phenomenology (appearance and experience) of psychopathology (mental difficulties) than a categorical classification system. However, the term has a varied history, meaning one thing when referring to a schizophrenia spectrum and another when referring to bipolar or obsessive-compulsive disorder spectrum, for example.
Types of Spectrum
The widely used DSM and ICD manuals are generally limited to categorical diagnoses. However, some categories include a range of subtypes which vary from the main diagnosis in clinical presentation or typical severity. Some categories could be considered subsyndromal (not meeting criteria for the full diagnosis) subtypes. In addition, many of the categories include a ‘not otherwise specified’ subtype, where enough symptoms are present but not in the main recognized pattern; in some categories this is the most common diagnosis.
Spectrum concepts used in research or clinical practice include the following.
Anxiety, Stress, and Dissociation
Several types of spectrum are in use in these areas, some of which are being considered in the DSM-5.
Name
Outline
Generalised Anxiety Spectrum
This spectrum has been defined by duration of symptoms: a type lasting over six months (a DSM-IV criterion), over one month (DSM-III), or lasting two weeks or less (though may recur), and also isolated anxiety symptoms not meeting criteria for any type.
Social Anxiety Spectrum
This has been defined to span shyness to social anxiety disorder, including typical and atypical presentations, isolated signs and symptoms, and elements of avoidant personality disorder.
Panic-Agoraphobia Spectrum
Due to the heterogeneity (diversity) found in individual clinical presentations of panic disorder and agoraphobia, attempts have been made to identify symptom clusters in addition to those included in the DSM diagnoses, including through the development of a dimensional questionnaire measure.
Post-Traumatic Stress Spectrum (or Trauma and Loss Spectrum)
Work in this area has sought to go beyond the DSM category and consider in more detail a spectrum of severity of symptoms (rather than just presence or absence for diagnostic purposes), as well as a spectrum in terms of the nature of the stressor (e.g. the traumatic incident) and a spectrum of how people respond to trauma. This identifies a significant amount of symptoms and impairment below threshold for DSM diagnosis but nevertheless important, and potentially also present in other disorders a person might be diagnosed with.
Depersonalisation-Derealisation Spectrum
Although the DSM identifies only a chronic and severe form of depersonalisation disorder, and the ICD a ‘depersonalisation-derealisation syndrome’, a spectrum of severity has long been identified, including short-lasting episodes commonly experienced in the general population and often associated with other disorders.
Obsessions and Compulsions
An obsessive-compulsive spectrum: This can include a wide range of disorders from Tourette syndrome to the hypochondrias, as well as forms of eating disorder, itself a spectrum of related conditions.
General Developmental Disorders
An autistic spectrum: In its simplest form this joins together autism and Asperger syndrome, and can additionally include other pervasive developmental disorders (PDD). These include PDD ‘not otherwise specified’ (including ‘atypical autism’), as well as Rett syndrome and childhood disintegrative disorder (CDD). The first three of these disorders are commonly called the autism spectrum disorders; the last two disorders are much rarer, and are sometimes placed in the autism spectrum and sometimes not. The merging of these disorders is based on findings that the symptom profiles are similar, such that individuals are better differentiated by clinical specifiers (i.e. dimensions of severity, such as extent of social communication difficulties or how fixed or restricted behaviours or interests are) and associated features (e.g. known genetic disorders, epilepsy, intellectual disabilities). The term specific developmental disorders is reserved for categorising particular specific learning disabilities and developmental disorders affecting coordination.
The schizophrenia spectrum or psychotic spectrum: There are numerous psychotic spectrum disorders already in the DSM, many involving reality distortion. These include:
Five subtypes of schizophrenia (although eliminated in DSM-5).
There are also traits identified in first degree relatives of those diagnosed with schizophrenia associated with the spectrum. Other spectrum approaches include more specific individual phenomena which may also occur in non-clinical forms in the general population, such as some paranoid beliefs or hearing voices. Some researchers have also proposed that avoidant personality disorder and related social anxiety traits should be considered part of a schizophrenia spectrum. Psychosis accompanied by mood disorder may be included as a schizophrenia spectrum disorder, or may be classed separately as below.
Schizoaffective Disorders
A schizoaffective spectrum: This spectrum refers to features of both psychosis (hallucinations, delusions, thought disorder etc.) and mood disorder (see below). The DSM has, on the one hand, a category of schizoaffective disorder (which may be more affective (mood) or more schizophrenic), and on the other hand psychotic bipolar disorder and psychotic depression categories. A spectrum approach joins these together and may additionally include specific clinical variables and outcomes, which initial research suggested may not be particularly well captured by the different diagnostic categories except at the extremes.
Schizophrenia-Like Personality Disorders
Schizoid personality disorder, schizotypal personality disorder and paranoid personality disorder can be considered ‘schizophrenia-like personality disorders’ because of their links to the schizophrenia spectrum.
Mood
A mood disorder (affective) spectrum or bipolar spectrum or depressive spectrum. These approaches have expanded out in different directions. On the one hand, work on major depressive disorder has identified a spectrum of subcategories and sub-threshold symptoms that are prevalent, recurrent and associated with treatment needs. People are found to move between the subtypes and the main diagnostic type over time, suggesting a spectrum. This spectrum can include already recognised categories of minor depressive disorder, ‘melancholic depression‘ and various kinds of atypical depression.
In another direction, numerous links and overlaps have been found between major depressive disorder and bipolar syndromes, including mixed states (simultaneous depression and mania or hypomania). Hypomanic (‘below manic’) and more rarely manic signs and symptoms have been found in a significant number of cases of major depressive disorder, suggesting not a categorical distinction but a dimension of frequency that is higher in bipolar II and higher again in bipolar I. In addition, numerous subtypes of bipolar have been proposed beyond the types already in the DSM (which includes a milder form called cyclothymia). These extra subgroups have been defined in terms of more detailed gradations of mood severity, or the rapidity of cycling, or the extent or nature of psychotic symptoms. Furthermore, due to shared characteristics between some types of bipolar disorder and borderline personality disorder, some researchers have suggested they may both lie on a spectrum of affective disorders, although others see more links to post-trauma syndromes.
Substance Use
A spectrum of drug use, drug abuse and substance dependence: One spectrum of this type, adopted by the Health Officers Council of British Columbia in 2005, does not employ loaded terms and distinctions such as “use” vs. “abuse”, but explicitly recognises a spectrum ranging from potentially beneficial to chronic dependence. The model includes the role not just of the individual but of society, culture and availability of substances. In concert with the identified spectrum of drug use, a spectrum of policy approaches was identified which depended partly on whether the drug in question was available in a legal, for-profit commercial economy, or at the other of the spectrum only in a criminal/prohibition, black-market economy. In addition, a standardised questionnaire has been developed in psychiatry based on a spectrum concept of substance use.
Paraphilias and Obsessions
The interpretative key of ‘spectrum,’ developed from the concept of ‘related disorders,’ has been considered also in paraphilias.
Paraphilic behaviour is triggered by thoughts or urges that are psychopathologically close to obsessive impulsive area. Hollander (1996) includes in the obsessive-compulsive spectrum, neurological obsessive disorders, body-perception-related disorders and impulsivity-compulsivity disorders. In this continuum from impulsivity to compulsivity it is particularly hard to find a clear borderline between the two entities.
On this point of view, paraphilias represent such as sexual behaviours due to a high impulsivity-compulsivity drive. It is difficult to distinguish impulsivity from compulsivity: sometimes paraphilic behaviours are prone to achieve pleasure (desire or fantasy), in some other cases these attitudes are merely expressions of anxiety, and the behavioural perversion is an attempt to reduce anxiety. In the last case, the pleasure gained is short in time and is followed by a new increase in anxiety levels, such as it can be seen in an obsessive patient after he performs his compulsion.
Eibl-Eibelsfeldt (1984) underlines a female sexual arousal condition during flight and fear reactions. Some women, with masochistic traits, can reach orgasm in such conditions.
Broad Spectrum Approach
Various higher-level types of spectrum have also been proposed, that subsume conditions into fewer but broader overarching groups.
One psychological model based on factor analysis, originating from developmental studies but also applied to adults, posits that many disorders fall on either an “internalising” spectrum (characterised by negative affectivity; subdivides into a “distress” subspectrum and a “fear” subspectrum) or an “externalising” spectrum (characterised by negative affectivity plus disinhibition). These spectra are hypothetically linked to underlying variation in some of the big five personality traits. Another theoretical model proposes that the dimensions of fear and anger, defined in a broad sense, underlie a broad spectrum of mood, behavioural and personality disorders. In this model, different combinations of excessive or deficient fear and anger correspond to different neuropsychological temperament types hypothesized to underlie the spectrum of disorders.
Similar approaches refer to the overall ‘architecture’ or ‘meta-structure’, particularly in relation to the development of the DSM or ICD systems. Five proposed meta-structure groupings were recently proposed in this way, based on views and evidence relating to risk factors and clinical presentation. The clusters of disorder that emerged were described as:
Neurocognitive (identified mainly by neural substrate abnormalities);
Neurodevelopmental (identified mainly by early and continuing cognitive deficits);
Psychosis (identified mainly by clinical features and biomarkers for information processing deficits);
Emotional (identified mainly by being preceded by a temperament of negative emotionality); and
Externalising (identified mainly be being preceded by disinhibition).
However, the analysis was not necessarily able to validate one arrangement over others. From a psychological point of view, it has been suggested that the underlying phenomena are too complex, inter-related and continuous – with too poorly understood a biological or environmental basis – to expect that everything can be mapped into a set of categories for all purposes. In this context the overall system of classification is to some extent arbitrary, and could be thought of as a user interface which may need to satisfy different purposes.
Cognitive models generally fall into the category of executive dysfunction or modulatory control. Neuroanatomically, functional and structural neuroimaging studies implicate the prefrontal cortex (PFC), basal ganglia (BG), insula, and posterior cingulate cortex (PCC). Genetic and neurochemical studies implicate glutamate and monoamine neurotransmitters, especially serotonin and dopamine.
The cortico-basal ganglia-thalamo-cortical loop (CBGTC) model is based on the observation that the basal ganglia loops related to the OFC and ACC are implicated in OCD by neuroimaging studies, although the directionality of volumetric and functional changes is not consistent. Causal evidence from OCD secondary to neuropsychiatric disorders supports the CBGTC model. Obsessions may arise from failure of the circuit to gate information that is normally implicitly processed, leading to representation in explicit processing systems such as the dlPFC and hippocampus, and thereby resulting in obsessions.
Abnormal affect in OCD has been hypothesized to result from dysfunction in the OFC, ventral striatum, and amygdala. OCD is characterised by high levels of anxiety, high rates of comorbidity with major depressive disorder, and blunted response to reward. This is reflected by reduced amygdala and ventral striatum response to positive stimuli, and elevated amygdala response to fearful stimuli. Furthermore, deep brain stimulation of the nucleus accumbens is an effective treatment of OCD, and symptom improvement correlates with reduced binding of dopamine receptors. The reduced binding, due to the ability of the radioligand tracers to be displaced by endogenous dopamine, is taken to reflect increased basal dopamine release. Affective dysregulation due to blunted reward, and elevated fear sensitivity may promote compulsivity by assigning excessive motivational salience to avoidance behaviour.
The ventral striatum is important in action selection, and receives inputs from the medial OFC that signal various aspects of value for stimulus association outcomes. By assigning abnormal values to certain behaviours, OFC may lead to compulsive behaviour through modulating action selection in the ventral striatum. A number of abnormalities have been found in the OFC, including reduced volume, increased resting state activity, and reduced activity during cognitive tasks. The difference between resting and cognitive paradigms may be due to increased signal to noise ratio, a possible mechanism of aberrant valuation. OFC-striatum connectivity also predicts symptom severity, although the opposite has been found in some studies.
Besides abnormal valuation of stimuli or tasks, compulsions may be driven by dysfunction in error monitoring that leads to excessive uncertainty.
OCD has also been conceptualised as resulting from dysfunction in response inhibition, and fear extinction. While hyperactivation of the OFC as a whole during resting is observed in OCD, hyperactivation of the lateral OFC and hypoactivation of the mOFC is seen. This is congruent with the localization of fear/avoidance behaviours to the lOFC and emotional regulation to the mOFC. Hyperactivity of the dACC during monitoring task, along with hyperactivity of the lOFC and amygadala may all contribute to generating obsessions, reduced regulation by the mOFC may enable them.
One model suggests that obsessions do not drive compulsions, but are rather byproducts of compulsions, as evidenced by some studies reporting excessive reliance on habit. Dysfunctional habit based learning may be a driver behind neuroimaging studies of memory reporting increased hippocampus activity. The conscious processing of information that is normally implicitly processing may be the underlying cause of obsessions.
Functional Neuroimaging
Functional neuroimaging studies have implicated multiple regions in OCD. Symptom provocation is associated with increased likelihood of activation in the bilateral orbitofrontal cortex (OFC), right anterior PFC, left dorsolateral prefrontal cortex (dlPFC), bilateral anterior cingulate cortex (ACC), left precuneus, right premotor cortex, left superior temporal gyrus (STG), bilateral external globus pallidus, left hippocampus, right insula, left caudate, right posterior cingulate cortex (PCC), and right superior parietal lobule. The medial portion of the orbitofrontal cortex connects with the paralimbic-limbic system, including the insular cortex, cingulate gryus, amygdala, and hypothalamus. This area is involved in encoding the representation of the value of an expected outcome, which is used to anticipate positive and negative consequences that are likely to follow a given action. During affective tasks hyperactivation has been observed in the ACC, insula and head of the caudate and putamen, regions implicated in salience, arousal, and habit. Hypoactivation during affective tasks is observed in the medial prefrontal cortex (mPFC) and posterior caudate, which are implicated in behavioural and cognitive control. During non-affective tasks, hyperactivation has been observed in the precuneus and PCC, while hypoactivation has been observed in the pallidum, ventral anterior thalamus and posterior caudate. An older meta analysis found hyperactivity in the OFC and ACC. An ALE meta analysis of various functional neuroimaging paradigms observed various abnormalities during Go/no go, interference, and task switching paradigms. Decreased likelihood of activation in right putamen and cerebellum was reported during Go/no go. During interference tasks, likelihood of activation was reported in the left superior frontal gyrus, right precentral gyrus, and left cingulate gyrus, to be decreased, and in the right caudate to be increased. Task switching was associated with extensive decreased likelihood of activation in the middle, medial, inferior, superior frontal gyri, caudate, cingulate and precuneus. A separate ALE meta analysis found consistent abnormalities in orbitofrontal, striatal, lateral frontal, anterior cingulate, middle occipital and parietal, and cerebellar regions.
Structural Neuroimaging
Differences in grey matter, white matter and structural connectivity have been observed in OCD. One meta-analysis reported grey matter increases in the bilateral lenticular nuclei, and grey matter decreases in the ACC (anterior cingulate cortex) and mPFC (medial prefrontal cortex).[14] Another meta-analysis reported that global volumes are not decreased, but the left ACC and OFC demonstrate decreased volume, while the thalamus but not basal ganglia have increased volumes. An ALE meta analysis found increased grey matter in the left postcentral gyrus, middle frontal region, putamen, thalamus, left ACC, and culmen, while decreased grey matter was reported in the right temporal gyrus and left insula extending to the inferior frontal gyrus.
Overlapping abnormalities in white matter volume and diffusivity have been reported. Increased white matter volume and decreased Fractional anisotropy has been observed in anterior midline tracts, interpreted as indicating increased crossings. However, given these effects were most pronounced in medicated adults, it is possible that medication plays a role An ALE meta analysis has observed increased FA in the superior longitudinal fasiculus and corpus callosum, and decreased FA in inferior longitudinal and cingulum fibres.
Neurochemistry
Glutamate, an excitatory neurotransmitter has been implicated in OCD. MRS studies have observed decreased Glx (glutamate, glutamine and GABA) in the striatum. However, increased Glx has been reported in the ACC. Furthermore, increased cerebrospinal fluid (CSF) glutamate and glycine have been found. Various preclinical models have supported glutamate signalling dysfunction in OCD, and treatment with glutamatergic agents such as the glutamate-inhibiting riluzole has been reported to be efficacious.
Reduced dopamine D1 receptors and dopamine D2 receptors in the striatum have been reported in people with OCD, along with both increased and decreased reports of dopamine transporter (DAT) binding. While antipsychotics are sometimes used to treat refractory OCD, they frequently fail in treating or exacerbate OCD symptoms. Treatment with deep brain stimulation is effective in OCD, and response correlates with increased dopamine in the nucleus accumbens. Combined this evidence suggests that OCD may be associated with both increased and decreased dopamine signalling, or that a unidirectional model may not be adequate.
Drug challenge studies have implicated 5-HT2A and 5-HT2A in OCD. Administration of meta-Chlorophenylpiperazine (mCPP), a non selective serotonin (5-HT) release and receptor agonist with a preference for 5-HT2C has been reported to exacerbate OCD symptoms. Psilocybin, a 5-HT2C, 5-HT2A and 5-HT1A receptor agonist has been associated with acute improvement of OCD symptoms. In vivo neuroimaging has found abnormalities with 5-HT2A and serotonin transporter (5-HTT). Inconsistent binding potentials have been observed for 5-HT2A, with both decreased and increased and binding potentials being reported. Inconsistent results have been reported in with respect to 5-HTT as well, with increased, decreased and no changes being reported.
Oestrogen and OCD
Aromatase is an enzyme expressed in several gonadic tissue sites. It is the rate limiting step in the conversion of androgens to oestrogen. This conversion can significantly impact oestrogen levels in brain areas. These OCD-linked effects have been demonstrated by Aromatase knockout mice (ArKO), who lack a functional enzyme to convert androgens to oestrogen. This ArKO knockout strategy has provided a model to examine the physiological impact of lower than normal amounts of oestrogen.
Studies with ArKO mice have been used to show that varying levels of oestrogen affect the onset of OCD behaviours. Lower amounts of oestrogen are associated with an increase of OCD behaviours in males more than females.
Variation in oestrogen can lead to increased levels of OCD symptoms within women as well. The disorder itself has a later onset in women, and tends to show two distinct peaks of onset. The first peak occurs around puberty and the second around the age of childbearing. These peaks correlate with time periods where oestrogen levels are highest in women.
The obsessive-compulsive spectrum is a model of medical classification where various psychiatric, neurological and/or medical conditions are described as existing on a spectrum of conditions related to obsessive-compulsive disorder (OCD).
“The disorders are thought to lie on a spectrum from impulsive to compulsive where impulsivity is said to persist due to deficits in the ability to inhibit repetitive behavior with known negative consequences, while compulsivity persists as a consequence of deficits in recognizing completion of tasks.”
OCD is a mental disorder characterised by obsessions and/or compulsions. An obsession is defined as “a recurring thought, image, or urge that the individual cannot control”. Compulsion can be described as a “ritualistic behaviour that the person feels compelled to perform”. The model suggests that many conditions overlap with OCD in symptomatic profile, demographics, family history, neurobiology, comorbidity, clinical course and response to various pharmacotherapies. Conditions described as being on the spectrum are sometimes referred to as obsessive-compulsive spectrum disorders.
Conditions
The following conditions have been hypothesized by various researchers as existing on the spectrum:
However, recently there is a growing support for proposals to narrow down this spectrum to only include body dysmorphic disorder, hypochondriasis, tic disorders, and trichotillomania.
Body dysmorphic disorder is defined by an obsession with an imagined defect in physical appearance, and compulsive rituals in an attempt to conceal the perceived defect. Typical complaints include perceived facial flaws, perceived deformities of body parts and body size abnormalities. Some compulsive behaviours observed include mirror checking, ritualised application of makeup to hide the perceived flaw, excessive hair combing or cutting, excessive physician visits and plastic surgery. Body dysmorphic disorder is not gender specific and onset usually occurs in teens and young adults.
Hypochondriasis
Hypochondriasis is excessive preoccupancy or worry about having a serious illness. These thoughts cause a person a great deal of anxiety and stress. The prevalence of this disorder is the same for men and women. Hypochondriasis is normally recognised in early adult age. Those that suffer with hypochondriasis are constantly thinking of their body functions, minor bumps and bruises as well as body images. Hypochondriacs go to numerous outpatient facilities for confirmation of their own diagnosis. Hypochondriasis is the belief that something is wrong but it is not known to be a delusion.
Tic Disorders
Tourette’s syndrome is a neurological disorder characterised by recurrent involuntary movements (motor tics) and involuntary noises (vocal tics). The reason Tourette’s syndrome and other tic disorders are being considered for placement in the obsessive compulsive spectrum is because of the phenomenology and co-morbidity of the disorders with obsessive compulsive disorder. Within the population of patients with OCD up to 40% have a history of a tic disorder and 60% of people with Tourette’s syndrome have obsessions and/or compulsions. Plus 30% of people with Tourette’s syndrome have clinically diagnosable OCD. Course of illness is another factor that suggests correlation because it has been found that tics displayed in childhood are a predictor of obsessive and compulsive symptoms in late adolescence and early adulthood. However, the association of Tourette’s and tic disorders with OCD is challenged by neuropsychology and pharmaceutical treatment. Whereas OCD is treated with SSRI, tics are treated with dopamine blockers and alpha-2 agonists.
Trichotillomania is an impulse control disorder which causes an individual to pull out their hair from various parts of their body without a purpose. The cause for trichotillomania remains unknown. Like OCD, trichotillomania isn’t a nervous condition but stress can trigger this habit. For some people pulling their hair out of boredom is normal, but that isn’t the case for someone that is dealing with trichotillomania. Emotions do not affect the behaviour but these behaviours are more prevalent in those that suffer with depression. Review articles recommend behavioural interventions such as habit reversal training and decoupling.
Kleine-Levin syndrome (KLS) is a rare disorder characterised by persistent episodic hypersomnia and cognitive or mood changes. Sometimes known as the Sleeping Beauty Syndrome.
Many patients also experience hyperphagia, hypersexuality and other symptoms. Patients generally experience recurrent episodes of the condition for more than a decade and may return at a later age. Individual episodes generally last more than a week, sometimes lasting for months. The condition greatly affects the personal, professional, and social lives of sufferers. The severity of symptoms and the course of the syndrome vary between sufferers. Patients commonly have about 20 episodes over about a decade. Several months generally elapse between episodes.
The onset of the condition usually follows a viral infection; several different viruses have been observed to trigger KLS. It is generally only diagnosed after similar conditions have been excluded; magnetic resonance imaging (MRI), computed tomography (CT) scans, lumbar puncture, and toxicology tests are used to rule out other possibilities. The syndrome’s mechanism is not known, but the thalamus is thought to possibly play a role. Single-photon emission computed tomography (SPECT) has shown thalamic hypoperfusion of patients during episodes.
KLS is very rare, occurring at a rate of 1 in 1 million, which limits research into genetic factors. The condition primarily affects adolescent males, though females can also be affected and the age of onset varies. There is no known cure, and there is little evidence supporting drug treatment. Lithium has been reported to have limited effects in case reports, decreasing the length of episodes and duration between them in some patients. Stimulants have been shown to promote wakefulness during episodes, but they do not counteract cognitive symptoms or decrease the duration of episodes. The condition is named after Willi Kleine and Max Levin, who described cases of the disease in the early 20th century. It was added to the International Classification of Sleep Disorders in 1990.
Brief History
In 1815, there was a report of a young man who showed excessive appetite and prolonged sleep after experiencing a fever; this may have been an early description of the condition. Another case with similar symptoms was described by Brierre de Boismont in 1862.
Five patients with symptoms of persistent sleepiness were described in detail in 1925 by Willi Kleine, a neurologist from Frankfurt. This report was followed four years later by details of a similar case by New York-based psychiatrist Max Levin. In 1935, Levin published information about several more cases, including one described by Kleine. Levin noted that some patients displayed an intense appetite in addition to their persistent tiredness. MacDonald Critchley, who first wrote about the condition in 1942, described 11 cases he had examined and reviewed 15 other published cases in a 1962 publication. In the report, which included patients he had examined in the Royal Navy during World War II, he observed that irritability and depersonalisation often occurred while patients were awake. He named the condition Kleine-Levin syndrome and noted four common traits: hypersexuality, adolescent onset, spontaneous resolution, and compulsive eating. He believed that the condition only affected males, but later studies showed some female patients. In the 1970s, several psychoanalytic and psychodynamic explanations for the condition were proposed. In 1980, a Hawaiian-Caucasian family was found in which nine family members suffered from the condition.
Diagnostic criteria for KLS was established by Schmidt in 1990, and the International Classification of Sleep Disorders further refined them. KLS is classified as a sleep disorder, specifically one of recurrent hypersomnia. Before 2005, hyperphagia and hypersexuality were thought to occur in all cases. That was changed with the guidelines published that year, which noted that they did not always occur.
Epidemiology
Population-based studies of KLS have not been performed. Its prevalence is about 1 case per million people. In France, KLS has a prevalence of 1.5 per million people. It occurs most frequently among Jews in the US and Israel. First-degree relatives of people who have suffered from the syndrome are much more likely than the general population to suffer from it, although only in about one percent of cases do family members contract it. About 70% to 90% of patients are male. Patients with the syndrome are more likely than the general population to have genetic disorders, and about a third of people with the syndrome encountered some form of birth difficulty. In a study of 186 older patients, about ten percent had pre-existing psychiatric issues. One study found that about ten percent of patients had a neurological condition before KLS developed. The condition does not appear to occur most frequently in one season.
Symptoms
Patients with KLS experience recurring episodes of prolonged sleep (hypersomnia). In most cases, patients sleep 15 to 21 hours a day during episodes. Excessive appetite (hyperphagia) and unusual cravings are present in half to two thirds of cases. About half of patients, mainly male patients, experience dramatically increased sexual urges (hypersexuality). Several other symptoms usually accompany the syndrome, including marked changes in mood and cognitive ability. Derealisation and severe apathy are present in at least 80% of cases. About one third of patients experience hallucinations or delusions. Depression and anxiety occur less commonly; one study found them in about 25% of patients. Individuals usually cannot remember what happened during episodes. Repetitive behaviours and headaches are commonly reported. Some patients act very childlike during episodes, and communication skills and coordination sometimes suffer.
Sleep studies of KLS show varying results based on the amount of time the patient is observed. Slow wave sleep is often reduced at the beginning of episodes, and rapid eye movement (REM) sleep is reduced near the end. Conversely, REM sleep is often normal at the beginning, and slow wave sleep is often normal by the conclusion. Stage two non-rapid eye movement sleep is often interrupted during KLS. Studies also show that stage one and three non-rapid eye movement sleep become more efficient when the episodes end. The Multiple Sleep Latency Test has yielded inconsistent results when given to KLS patients. In many cases, hours are spent in a withdrawn sleep-like state while awake during episodes. Most sleep studies have been performed while subject is near the end of their episodes. Some patients experience brief insomnia and become very happy and talkative after the episode ends.
The first time a patient experiences KLS, it usually occurs along with symptoms that are similar to those of the flu or encephalitis. In at least 75% of cases, symptoms occur after an airway infection or a fever. Viruses observed before the development of the condition include Epstein-Barr virus, varicella zoster virus, herpes zoster virus, influenza A virus subtypes, and adenovirus. Several days after symptoms first occur, patients become very tired. In cases that occur after an infection, KLS usually starts within three to five days for teenagers and fewer for children. In other cases, alcohol consumption, head injury, or international travel precede symptoms. Lifestyle habits, such as stress, alcohol abuse and lack of sleep and stress, have also been proposed as possible triggers. First episodes of KLS are preceded by a clear event in about 90% of cases. Recurrences generally do not have clear triggers; only about 15% have a precipitating event.
The condition generally disrupts the social lives and academic or professional obligations of sufferers. Some patients also gain weight during episodes. The most severe cases cause a long-term impact on mood and cognitive attention. In rare cases, patients experience long-term memory problems.
In patients with KLS, MRI and CT scans show normal brain morphology. When SPECT is performed, hypoperfusion can often be observed in the brain, particularly in the thalamic and frontotemporal areas. The hypoperfusion is significantly diminished between episodes. Serum biology, c-reactive proteins and leptins, the hormonal pituitary axis, and protein in the cerebral spinal fluid (CSF) are normal in KLS patients.
Cause
It is not known what causes KLS, but several mechanisms have been proposed. One possible explanation is hypothalamic or circadian dysfunction. The thalamus probably plays a role in the out-of-control sleeping, and patients with diencephalic-hypothalamic dysfunction caused by tumours experience symptoms similar to those of KLS patients. Specifically, the medial temporal regions of the thalamus may be involved, although examinations of KLS patients have not consistently found abnormalities in this area. The temporal lobe also appears to play a role in the condition, possibly causing cognitive difficulties. The apathy and disinhibition found in some KLS sufferers suggest that the condition may include frontal lobe dysfunction as well. The involvement of the thalamus, temporal lobe, and frontal lobe of the brain suggests that there is a multifocal, localised encephalopathy. There are also persistent subclinical abnormalities in KLS sufferers.
Another possible explanation concerns the metabolism of serotonin and dopamine. An imbalance in the neurotransmitter pathways of these chemicals could play a role. Viral infections have also been suggested as a possible cause. Evidence for their role includes lesions found in autopsies. Cerebral spinal fluid (CSF) samples from KLS patients indicate that the condition has a different cause than influenza-associated encephalopathy. Triggers of KLS may also affect the blood-brain barrier, which could play a role in the condition. There is limited evidence of what role hypocretin may play, although it often influences hypersomnia.
Androgen might (indirectly) block melatonin receptors, possibly by means of vasodilation, and cause cholinergic abnormalities in some cases of KLS.
Because KLS occurs at a much higher rate in Jews and in some families, it is likely that there is some genetic component in addition to environmental factors. Genetic studies hold promise for understanding the disease, but they have yielded inconsistent results and few patients are available for testing.
Epilepsy and depression do not appear to cause KLS. The condition’s rapid onset after infections indicates that the immune system is not to blame.
One study has suggested a link to the gene LMOD3 on chromosome 3.
Diagnosis
KLS can be diagnosed when there is confusion, apathy, or derealisation in addition to frequent bouts of extreme tiredness and prolonged sleep. The earliest it can be diagnosed is the second episode, this is not common. The condition is generally treated as a diagnosis of exclusion. Because KLS is rare, other conditions with similar symptoms are usually considered first.
MRIs can determine if the symptoms are caused by certain brain disorders, stroke, and multiple sclerosis. Lumbar puncture can determine if encephalitis is the cause. KLS must be differentiated from substance abuse by toxicology tests. The use of electroencephalography (EEG) can exclude temporal status epilepticus from consideration. EEGs are normal in about 70% of KLS patients, but background slowing may sometimes be detected. In addition, low-frequency high-amplitude waves can be observed during waking hours.
Initially, KLS appears similar to bipolar depression. Patients with frontal-lobe syndromes and Klüver-Bucy syndrome also display similar symptoms, but these conditions can be differentiated by the presence of brain lesions. KLS should also be distinguished from very rare cases of menstruation-caused hypersomnia.
Prevention
Lithium is the only drug that appears to have a preventive effect. In two studies of more than 100 patients, lithium helped prevent recurrence of symptoms in 20% to 40% of cases. The recommended blood level of lithium for KLS patients is 0.8-1.2 mEq/ml. It is not known if other mood stabilisers have an effect on the condition. Anti-depressants do not prevent recurrence.
Treatment
Several drug therapies have been used on patients with KLS, but none of them have been subject to randomized controlled trials. A 2016 Cochrane Review concluded that “No evidence indicates that pharmacological treatment for Kleine-Levin syndrome is effective and safe”.
In several cases, stimulants, including modafinil, have been reported to have a limited effect on patients, often alleviating sleepiness. They can cause behavioural problems, but they may pose fewer issues if used in older patients with mild symptoms. In some case reports, lithium has been reported to decrease the length of episodes and the severity of their symptoms and to increase the time between episodes. It has been reported to be effective in about 25 to 60% of cases. Its use carries the risk of side effects in the thyroid or kidneys. Antipsychotics and benzodiazepines can help alleviate psychotic and anxiety related symptoms, respectively. Carbamazepine has been reported to be less effective than lithium but more effective than some drugs in its class. Electroconvulsive therapy is not effective and worsens symptoms.
KLS patients generally do not need to be admitted to hospitals. It is recommended that caregivers reassure them and encourage them to maintain sleep hygiene. It may also be necessary for patients to be prevented from putting themselves in dangerous situations, such as driving.
Prognosis
The frequency of KLS episodes can vary from attacks one week in length occurring twice a year to dozens of episodes that follow each other in close succession. The median duration of KLS episodes is about ten days, but some last several weeks or months. A study of 108 patients found an average of 19 episodes over the duration of the disease. Another study found a median of 3.5 months between episodes. Outside of episodes, there is no disturbance in patients’ sleep patterns and they are generally asymptomatic. Patients do not experience the same symptoms in each episode.
About 80% of patients are adolescents when they first experience KLS. On some occasions though, its first occurrence comes in childhood or adulthood. In most adolescent-onset patients, symptoms cease by the time they are 30 years old. A French study of 108 patients found a median duration of 13 years, but a review of 186 cases found a median duration of 8 years. Unusually young or old patients and those who experience hypersexuality tend to have a more severe course. Patients who initially have frequent attacks generally see the disease cease earlier than others. The condition spontaneously resolves, and the patient is considered to be cured if there have been no symptoms for six years.
The concept has its origins as far back as the year 1889, when the German psychiatrist Emil Kraepelin first used the term of “periodic mania” to refer to people with recurrent manic episodes and no depression. One year later, Carl Wernicke proposed that mania and depression should be viewed as separate disorders. As the time went on, unipolar mania became an invalid diagnosis due to its variations across different patients. Currently patients with symptoms of mania, even in the absence of any depressive symptoms, would get the bipolar 1 diagnosis.
Symptoms
Symptoms of unipolar mania are similar to those of bipolar mania. They can include:
Excessive involvement in activities with a high likelihood of painful consequences.(e.g. extravagant shopping, improbable commercial schemes, hypersexuality).
The episode generally have a stronger tendency to present with psychosis or/and need psychiatric assistance.
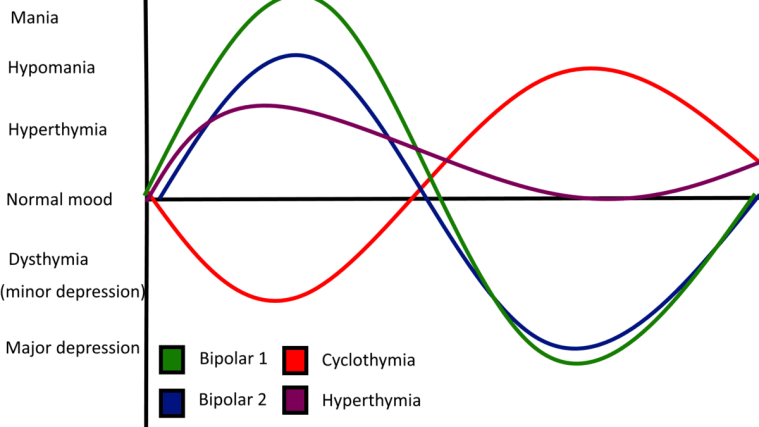
Hyperthymic temperament, or hyperthymia, from Ancient Greek ὑπέρ (“over”, meaning here excessive) + θυμός (“spirited”), is a proposed personality type characterised by an exceptionally, or in some cases, abnormally positive mood and disposition.
Also known as Hyperthymic Personality-Type and Chronic Hypomania.
Graph showing showing hyperthymia in comparison to other bipolar spectrum disorders.
Background
It is generally defined by increased energy, vividness and enthusiasm for life activities, as opposed to dysthymia. Hyperthymia is similar to but more stable than hypomania.
Characteristics of the hyperthymic temperament include:
Increased energy and productivity.
Short sleep patterns.
Vividness, activity extroversion.
Self-assurance, self-confidence.
Strong will.
Extreme talkativeness.
Tendency to repeat oneself.
Risk-taking/sensation seeking.
Breaking social norms.
Very strong libido.
Love of attention.
Low threshold for boredom.
Generosity and tendency to overspend.
Emotion sensitivity.
Cheerfulness and joviality.
Unusual warmth.
Expansiveness.
Tirelessness.
Irrepressibility, irresistible, and infectious quality.
The clinical, psychiatric understanding of hyperthymia is evolving. Studies have shown that hyperthymic temperament promotes efficient performance of complex tasks under time pressure or extreme conditions. Despite this positive characterisation, hyperthymia can be complicated with depressive episodes manifesting as a softer form of bipolar illness, such as cyclothymia. Research also suggests a familial genetic connection of the temperament to bipolar I.
Aside from references in historical and more recent writings on the spectrum of mood disorders, further literature on the temperament is lacking. There is a lack of agreement on its definition, implications or whether it is pathological. It is not known where to place hyperthymia on the affective spectrum.
Hyperthymia manifesting intermittently or in an unusual way may mask hypomania or another psychiatric disorder. Hyperthymia can be most accurately diagnosed by a psychologist or psychiatrist with the help of a patient’s family and/or close friends.
Disorganised schizophrenia, or hebephrenia, was a subtype of schizophrenia prior to 2013. Subtypes of schizophrenia were no longer recognised as separate conditions in DSM 5 published in 2013. The disorder is no longer listed in the 11th revision of the International Classification of Diseases (ICD-11).
Disorganised schizophrenia is classified within ICD-10 the existing classification, in practice, until the 01 January 2022, as a mental and behavioural disorder, because the classification was thought to be an extreme expression of the disorganisation syndrome that has been hypothesized to be one aspect of a three-factor model of symptoms in schizophrenia, the other factors being reality distortion (involving delusions and hallucinations) and psychomotor poverty (lack of speech, lack of spontaneous movement and various aspects of blunting of emotion).
Presentation
The condition is also known as hebephrenia, named after the Greek term for “adolescence” – ἥβη (hḗbē) – and possibly the ancient-Greek goddess of youth, Hebe, daughter of Hera. The term refers to the ostensibly more prominent appearance of the disorder in persons around puberty.
The prominent characteristics of this form are disorganised behaviour and speech (see formal thought disorder), including loosened associations and schizophasia (“word salad”), and flat or inappropriate affect. In addition, psychiatrists must rule out any possible sign of catatonic schizophrenia.
The most prominent features of disorganised schizophrenia are not delusions and hallucinations, as in paranoid schizophrenia, although fragmentary delusions (unsystemised and often hypochondriacal) and hallucinations may be present. A person with disorganised schizophrenia may also experience behavioural disorganisation, which may impair his or her ability to carry out daily activities such as showering or eating.
The emotional responses of such people often seem strange or inappropriate. Inappropriate facial responses may be common, and behaviour is sometimes described as “silly”, such as inappropriate laughter. Sometimes, there is a complete lack of emotion, including anhedonia (lack of pleasure), and avolition (lack of motivation). Some of these features are also present in other types of schizophrenia, but they are most prominent in disorganised schizophrenia.
Treatment
This form of schizophrenia is typically associated with early onset (often between the ages of 15 and 25 years) and is thought to have a poor prognosis because of the rapid development of negative symptoms and decline in social functioning.
Use of electroconvulsive therapy has been proposed; however, the effectiveness after treatment is in question.
Secondary mania, also known as organic mania, is a variation of bipolar disorder that is caused by physical trauma or illness.
Bipolar disorder has a 1% prevalence rate in the United States and secondary mania is likely a small subset of that percentage. Secondary mania exhibits symptoms similar to that of mania in bipolar I and bipolar II disorders. This includes an elevated mood or affect, psychotic state, accelerated speech, increased motor activity, irritability, and flight ideas. A unique criterion for secondary mania is the lack of history of mental illness that causes mania, such as bipolar disorder. Unlike bipolar disorder, which has an average age of onset at 25 years, secondary mania has an average age of onset at 45 years. Little is known about secondary mania, as much of the research on it is case studies and retrospective accounts. However, it has been connected to several causes such as traumatic brain injury, HIV/AIDS, and stroke.
Closed-Head Injury
One of the primary documented causes of secondary mania is traumatic brain injury, also called closed-head injury. For example, Jorge and colleagues examined the effects of traumatic brain injury and its correlation with secondary mania. They collected participants that in the previous year had had traumatic brain injuries. They did 3, 6, and 12-month follow-ups with the patients where they took psychiatric interviews to measure impairment of daily life, intellectual, and social function. Within the 9% of patients that met the criteria for secondary mania, a correlation between secondary mania and temporal basal polar lesion was found. On average, the duration of secondary mania was 2 months. A second study found that out of 66 patients with a closed head injury, 9% experienced mania during the 12-month period after their injury.
In a case study a 24-year-old man complained of symptoms of mania. He had no prior mental health issues, no family history for mental health disorders, and no history of substance abuse. After a medical examination, he was diagnosed with mania and psychotic symptoms. Soon after he reported having a severe headache and after examination it was found he had a heterogeneous lesion covering most of his left thalamus. After the lesion was discovered, his diagnosis was revised to be “organic mood disorder (left cerebral AVM, Arteriovenous malformation, with secondary mania)”. Another study by Jorge and colleagues looked at the effects of traumatic brain injury and its correlation with secondary mania.
HIV/AIDS
Secondary mania has been associated with HIV/AIDS in a number of cases. According to Ellen and colleagues, secondary mania is reported in 1.2% of HIV-positive patients and 4.3% positive in those with AIDS. In one case study by Chou and colleagues, a 78-year-old man was admitted to the hospital for manic symptoms. “The symptoms included decreased sleep, elevated mood, increased energy, hyperactivity, racing thoughts, and eccentric behaviour”. The patient had no prior history of mental health problems in his family or his own medical records. He was temporarily diagnosed with bipolar one. It was later discovered that he suffered from HIV/AIDS and his diagnosis was altered to secondary mania.
Drugs
Many drugs have direct or indirect effects on neurotransmitters. Steroids are especially proficient at causing changes to the chemistry of neurotransmitters. In a study, 40 women were given steroids to help with their rheumatoid arthritis. Three subjects developed manic symptoms within the first week of taking the steroid. Two had never had a diagnosis of a mental illness, and one of the three women was noted to be “emotionally labile” and had had a suicide attempt but no hospitalisation. It was noted that the mania was not caused by an electrolyte imbalance, but the exact cause was uncertain.
According to Ogawa and Ueki, secondary mania has also been associated with caffeine consumption. A 43-year-old man, with no prior history of mental illness, reportedly switched to drinking 10 cups of coffee a day. After consuming this amount, he was reported to have manic symptoms such as elevated mood, talkativeness, hyperactivity, grandiosity, flight of ideas, and insomnia. This led to his admission into a hospital. After examination, they removed caffeine from the man’s diet, resulting in the cessation of manic symptoms. The doctors then concluded that either the caffeine had acted as a catalyst for bipolar disorder or that he had secondary mania. Unfortunately, little research is done on studying the interaction between mood disorders and caffeine.
Other
A case study by Liang and Yang was of a 75-year-old woman who was admitted to the hospital with fever, chills, headache, and vomiting. Upon doing a mental test, they discovered she had symptoms of mania. However, she had no prior history of mental illness. When speaking with the family they discovered that the symptoms had manifested two weeks prior. Eventually, she was diagnosed with enterococcal meningitis for her physical symptoms and secondary mania for her psychological symptoms. The study stated that the exact link between the secondary mania and the enterococcal meningitis is unknown.
Controversy
Since its first discovery over 30 years ago, secondary mania has been difficult to conceptualise. The primary arguments regarding its aetiology are:
Secondary mania is a form of toxic psychosis rather than actual mania; and
Secondary mania is really latent bipolar disorder that happened to coincide with an injury.
Toxic psychosis is a state which is caused by substance abuse; this could mean being in a confused state from the substance. The main argument against this theory is that mania in general has toxic origins and secondary mania is no different in this regard. However, analyses of secondary mania tend to exclude cases in which the person experienced high levels of confusion. Therefore, stating that it is a toxic state does not take away from the validity of its existence as long as the cases of secondary mania are narrowed to those without the confused state. The second argument is harder to dispute, as it is possible that secondary mania is late-onset bipolar disorder. The way this claim is disputed is through looking at the history of the patient. They check to see if there is a negative pre-morbid history, a lack of history of mental illness, age of onset, and the close proximity of the organic trauma to the mania.
Bipolar disorder in children, or paediatric bipolar disorder (PBD), is a controversial mental disorder in children and adolescents that is mainly diagnosed in the United States, and is hypothesized to be like bipolar disorder (BD) in adults, thus is proposed as an explanation for extreme changes in mood and behaviour accompanying periods of depressed or irritable moods and periods of elevated moods so called manic or hypomanic episodes.
These shifts are sometimes quick, but usually are gradual. The average age of onset of paediatric bipolar disorder is unclear, but the risk increases with the onset of puberty. Bipolar disorder is rare in childhood. Paediatric bipolar disorder is typically more severe and has a poorer prognosis than bipolar disorder with onset in late-adolescence or adulthood.
The DSM has specified that the criteria for bipolar disorder can be applied to children since 1980. However, the exact criteria for diagnosing paediatric bipolar disorder remains controversial and heavily debated. There are big differences in how commonly it is diagnosed across clinics and in different countries. There has been a rapid increase in research on the topic, but training and clinical practice lag behind.
Identifying bipolar disorder in youth is challenging. Children often exhibit chronic rather than episodic mania periods. Almost always, these chronic problems have causes other than bipolar disorder. The criteria for paediatric bipolar disorder can also often be masked by developmental differences. Comorbid disorders make determining what symptoms are signs of bipolar disorder and which are due to other disorders (e.g. OCD, ADHD, disruptive behaviour problems) difficult, leading to complications in treatment. For example, a common treatment for OCD are serotonin re-uptake inhibitors (SRIs), however, SRIs can lead to mood instability and worsening bipolar disorder.[5] The most common misdiagnosis for ADHD in the USA is paediatric bipolar disorder due to hyperactivity being described as prolonged periods of mania. Empirical research conducted in 2004 found that “bipolar disorder (in preadolescence) was initially misdiagnosed in 12 out of 24 youths” (Mahoney, 2004). This is a dangerous misdiagnosis due to the vastly different treatment forms. Firstly, ADHD does not require mood stabilisers like paediatric bipolar disorder. Secondly, the stimulants given to treat ADHD have been shown to cause psychosis and exacerbate mania in paediatric bipolar disorder (Wendling, 2009). This misuse of medication can lead to mood episodes, suicidality, and hospitalisation.
Brief History
Descriptions of children with symptoms similar to contemporary concepts of mania date back to the 18th century. In 1898, a detailed psychiatric case history was published about a 13-year-old that met Jean-Pierre Falret and Jules Baillarger’s criteria for folie circulaire, which is congruent to the modern conception of bipolar I disorder.
In Emil Kraepelin’s descriptions of bipolar disorder in the 1920s, which he called “manic depressive insanity”, he noted the rare possibility that it could occur in children. In addition to Kraepelin, Adolf Meyer, Karl Abraham, and Melanie Klein were some of the first to document bipolar disorder symptoms in children in the first half of the 20th century. It was not mentioned much in English literature until the 1970s when interest in researching the subject increased. It became more accepted as a diagnosis in children in the 1980s after the DSM-III (1980) specified that the same criteria for diagnosing bipolar disorder in adults could also be applied to children.
Recognition came twenty years after, with epidemiological studies showing that approximately 20% of adults with bipolar disorder already had symptoms in childhood or adolescence. Nevertheless, onset before age 10 was thought to be rare, below 0.5% of the cases. During the second half of the century misdiagnosis with schizophrenia was not rare in the non-adult population due to common co-occurrence of psychosis and mania, this issue diminishing with an increased following of the DSM criteria in the last part of the 20th century.
Epidemiology
The prevalence of bipolar in youth is estimated at 2%.
Diagnosis
Diagnosis is made based on a clinical interview by a psychiatrist or other licensed mental health practitioner. There are no blood tests or brain scans to diagnose bipolar disorder. Obtaining information on family history and the use of questionnaires and checklists are helpful in making an accurate diagnosis. Commonly used assessment tools include the:
In both the American Psychiatric Association’s DSM-5 and the World Health Organisation’s ICD-10, the same criteria used to diagnose bipolar disorder in adults are used to make the diagnosis in children with some adjustments to account for differences in age and developmental stage. For example, the DSM-5 specifies that in children, depressive episodes can manifest as persistently irritable moods.
In diagnosing manic episodes, it is important to compare the changes in mood and behaviour to the child’s normal mood and behaviours at baseline instead of to other children or adults. For example, grandiosity (i.e. unrealistic overestimation of one’s intelligence, talent, or abilities) is normal at varying degrees during childhood and adolescence. Therefore, grandiosity is only considered symptomatic of mania in children when the beliefs are held despite being presented with concrete evidence otherwise or when they lead to a child attempting activities that are clearly dangerous, and most importantly, when the grandiose beliefs are an obvious change from that particular child’s normal self-view in between episodes.
Controversy
The diagnosis of childhood bipolar disorder is controversial, although it is recognised that bipolar disorder typical symptoms are dysfunctional and have negative consequences for minors suffering them. Main discussion is centred on whether what is called bipolar disorder in children refers to the same disorder than when diagnosing adults, and the related question on whether adults’ criteria for diagnosis are useful and accurate when applied to children. More specifically, main discussion over diagnosis in children circles around mania symptomatology and its differences between children and adults.
Diagnostic criteria may not correctly separate children with bipolar disorder from other problems such as ADHD, and emphasize fast mood cycles.
Treatment
Medications can produce important side effects, so interventions have been recommended to be closely monitored and families of patients to be informed of the different possible problems that can arise. Atypical antipsychotics are more effective than mood stabilizers, but have more side effects. Typical antipsychotics may produce weight gains as well as other metabolic problems, including diabetes mellitus type 2 and hyperlipidaemia. Extrapyramidal secondary effects may appear with these medications. These include tardive dyskinesia, a difficult-to-treat movement disorder (dyskinesia) that can appear after long-term use of antipsychotics. Liver and kidney damage are a possibility with mood stabilisers.
Psychological treatment usually includes some combination of education on the disease, group therapy and cognitive behavioural therapy (CBT). Children with bipolar disorder and their families are informed, in ways accordingly to their age and family role, about the different aspects of bipolar disorder and its management including causes, signs and symptoms and treatments. Group therapy aims to improve social skills and manage group conflicts, with role-playing as a critical tool. Finally, cognitive-behavioural training is directed towards the participants having a better understanding and control over their emotions and behaviours.
Lithium or Divalproex is recommended for first-line treatment.
Partial (minimal to moderate) improvement with monotherapy, augment with another of the first-line recommendations.
Stage 2: Monotherapy with an alternative drug, then augmentation.
Stage 3: Possible medication combinations – lithium plus Divalproex, lithium plus atypical, or Divalproex plus atypical.
Stage 4: Combination of 2-3 mood stabilisers.
Stage 5: Alternate monotherapy with oxcarbazepine, ziprasidone, or aripiprazole (all Level D).
Stage 6: For nonresponse or intolerable side effects – clozapine for children or adolescents, or electroconvulsive therapy (ECT) for adolescents only.
BPD I, manic or mixed, with psychosis:
Stage 1: Same as BPD I without psychosis except for first-line treatment warrants a combination of mood stabiliser and an atypical antipsychotic.
Stages 2-4: Varying combinations and augmentations.
Stage 5: Alternate monotherapy (oxcarbazepine) plus an atypical antipsychotic.
Prognosis
Chronic medication is often needed, with relapses of individuals reaching rates over 90% in those not following medication indications and almost to 40% in those complying with medication regimens in some studies. Compared to adults, a juvenile onset has in general a similar or worse course, although age of onset predicts the duration of the episodes more than the prognosis. A risk factor for a worse outcome is the existence of additional (comorbid) pathologies.
Children with bipolar disorder are more likely to suicide than other children.


You must be logged in to post a comment.