The International Society for Bipolar Disorders (ISBD) is a non-profit organisation based in Pittsburgh, Pennsylvania, where it was founded 17 June 1999. The society focuses on research and education in bipolar disorders.
The society has a membership consisting of mental health professionals and patients and their family members representing 50 countries. The mission of the society is to advance the treatment of all aspects of bipolar disorder, thereby improving patient outcomes and quality of life, through fostering international collaboration in education and research. The society hosts biennial professional meetings and offers educational programmes. The official journal of the society is Bipolar Disorders and a subscription is included with membership.
Brief History
The ISBD was founded at the 3rd International Conference on Bipolar Disorder, in Pittsburgh, Pennsylvania, in June 1999 by David J. Kupfer and Thomas Detre (University of Pittsburgh Medical Centre). In September 1999, the official peer-reviewed society journal, Bipolar Disorders, published its first issue.
The ISBD held its first meeting in Sydney, Australia, in February 2004 with over 400 participants in attendance. The society held its second meeting in August 2006 in Edinburgh, Scotland, with over 600 attendees. As of 2013, the society has over 800 members in 50 countries with an elected board representing 15 countries.
Educational Programmes
The society supports the following educational initiatives:
The Psychiatric Trainee Support programme:
Offers psychiatric trainees a free two-year membership in the society in order to enhance knowledge of bipolar disorder among this group, narrow the gap between bipolar research and clinical practice, and ultimately to improve diagnosis, treatment and outcomes for patients with bipolar disorder.
These supported memberships are open to psychiatric residents, postgraduate students and junior faculty up to the Assistant Professor or equivalent level with less than five years as faculty in their career trajectory.
The programmes seek to support 70% of trainees from developing countries.
The Samuel Gershon Awards for Junior Investigators:
Named in honour of Samuel Gershon, past ISBD President and pioneer of early lithium research, offer four awards for original research submissions.
Awards are based on the originality of the content, as well as the significance of the findings reported, and are evaluated by an international scientific panel under the auspices of the ISBD.
These awards are open to psychiatric trainees, postgraduate students and junior faculty up to the assistant professor rank from around the world.
The awards are presented in conjunction with the society’s biennial meeting where the winners present their research in a special session showcasing the work of junior people in the field.
The ISBD Research Fellowship for Junior Investigators:
Provides an opportunity for the recipient to travel to another facility to get training in a particular type of research methodology (i.e. brain imaging, genetics, clinical trials, etc.).
The fellowship is intended to cover up to six months support for salary, travel, or some combination of these costs as they are incurred in pursuit of additional training.
This could take the form of summer programs, participation in smaller prospective studies, or through some other opportunity.
Conferences
The society organises biennial meetings that provides updates on topics such as epidemiology, pharmacotherapy, psychotherapies, genetics, neurobiology, imaging research, and bipolar disorder in special populations.
The General Behavior Inventory (GBI) is a 73-question psychological self-report assessment tool designed by Richard Depue and colleagues to identify the presence and severity of manic and depressive moods in adults, as well as to assess for cyclothymia.
It is one of the most widely used psychometric tests for measuring the severity of bipolar disorder and the fluctuation of symptoms over time. The GBI is intended to be administered for adult populations; however, it has been adapted into versions that allow for juvenile populations (for parents to rate their offspring), as well as a short version that allows for it to be used as a screening test.
The GBI was originally made as a self-report instrument for college students and adults to use to describe their own history of mood symptoms. The original item set included clinical characteristics and associated features in addition to the diagnostic symptoms of manic and depressive states in the current versions of the Diagnostic and Statistical Manual (DSM) of the American Psychiatric Association. The first set of 69 items was increased to 73, with the final version having 73 mood items and 6 additional questions to check the validity of responses (but which did not figure in the scale scores). The self report version of the GBI has been used in an extensive programme of research, accruing evidence of many facets of validity. Because of its length and high reading level, there also have been many efforts to develop short forms of the GBI.
7 Up 7 Down Inventory (7U7D)
The 7 Up-7 Down (7U7D) is a 14-item measure of manic and depressive tendencies that was carved from the full length GBI. This version is designed to be applicable for both youths and adults, and to improve separation between both mania and depressive conditions. It was developed via factor analysis from nine separate samples pooled into two age groups, ensuring applicability for use in youth and adults.
A sleep scale also has been carved from the GBI, using the seven items that ask about anything directly related to sleep.
Parent Report on the GBI (P-GBI)
The P-GBI is an adaptation of the GBI, consisting of 73 Likert scale items rated on a scale from 0 (“Never or Hardly Ever”) to 3 (“Very often or Almost Constantly”). It consists of two scales: a depressive symptoms (46 items) and a hypomanic/biphasic (mixed) symptoms (28 items).
Parent Short Forms
Again, due to the length of the full version, several short forms have been built and tested in multiple samples that may be more convenient to use in clinical work. These include 10 item mania, two alternate 10 item depression forms, and the seven item Sleep scale. All have performed as well or better than the self-report version when completed by an adult familiar with the youth’s behaviour (typically a parent).
The PGBI-10M is a brief (10-item) version of the PGBI that was validated for clinical use for patients presenting with a variety of different diagnoses, including frequent comorbid conditions. It is administered to parents for them to rate their children between ages 5-17. The 10 items include symptoms such as elated mood, high energy, irritability and rapid changes in mood and energy as indicators of potential juvenile bipolar disorder. The PhenX Toolkit uses this instrument as its child protocol for Hypomania/Mania Symptoms.
Teacher Report on the GBI
One study had a large sample of teachers complete the GBI to describe the mood and behaviour of youths age 5 to 18 years old. The results indicated that there were many items that teachers did not have an opportunity to observe the behaviour (such as the items asking about sleep), and others that teachers often chose to skip. Even after shortening the item list to those that teachers could report about, the validity results were modest even though the internal consistency reliability was high. The results suggested that it was challenging for teachers to tell the difference between hypomanic symptoms and symptoms attributable to attention-deficit/hyperactivity disorder, which is much more common in the classroom. The results aligned with findings from a large meta-analysis that teacher report had the lowest average validity across all mania scales compared to adolescent or parent report on the same scales. Based on these results, current recommendations are to concentrate on parent and youth report, and not use teacher report as a way of measuring hypomanic symptoms in youths.
Psychometric Properties
The GBI has been used extensively in research, including clinical samples, college students, longitudinal, treatment, and other studies. However, no normative data exist to calibrate scores in the general population.
Reliability
The GBI has exceptionally high internal consistency because it has long scales with a large number of items. The GBI shows high reliability whether completed as a self report or as a caregiver report about youth behaviour.
Retest reliability also is good over a week or two week period, although the GBI’s length makes it tedious to complete frequently.
Interpretation
GBI Scoring
The current GBI questionnaire includes 73 Likert-type items which reflect symptoms of different moods. The original version of the GBI used case scoring where items were given values ranging from 1-4. Symptoms that were rated as 1 or 2 were considered to be absent and symptoms rated as 3 or 4 were considered to be present. However, if each item were to receive one of four scores, the authors of the GBI decided Likert scaling would be a better scoring option. The items on the GBI are now scaled from 0-3 rated as 0 (never or hardly ever present), 1 (sometimes present), 2 (often present), and 3 (very often or almost constantly present).
PGBI-10M
For the PGBI-10M, the scores from each question are added together to form a total score, with higher scores indicating a greater severity of symptoms. Scores range from 0 to 30. Low scores of 5 and below indicate a very low risk of a bipolar diagnosis. High scores of 18 and over indicate a high risk of a diagnosis of bipolar disorder, increasing the likelihood by a factor of seven or greater. Several peer-reviewed research studies support the P-GBI as a reliable and valid measure of bipolar in children and adolescents. It is recommended to be used as part of an assessment battery in the diagnosis of juvenile bipolar disorder.
Limitations
The GBI is free for use clinically and in research. The reading level and length make it challenging for some people to complete. Being a self-report questionnaire, the GBI is not known to have any adverse effects on patients beyond the potential of causing minor distress.
Research
Shorter versions of the GBI have been validated for research and clinical use. For instance, the PGBI-10M is currently being tested as part of a large longitudinal study investigating the course of early symptoms of mania in children[citation needed], with preliminary studies indicating its clinical efficacy in differentiating juvenile bipolar disorder from youth with other diagnoses.
It asks about 32 behaviours and mental states that are either aspects of hypomania or features associated with mood disorders. It uses short phrases and simple language, making it easy to read. The University of Zurich holds the copyright, and the HCL-32 is available for use at no charge. More recent work has focused on validating translations and testing whether shorter versions still perform well enough to be helpful clinically. Recent meta-analyses find that it is one of the most accurate assessments available for detecting hypomania, doing better than other options at recognising bipolar II disorder.
Development and Brief History
The Hypomania Checklist was built as a more efficient screening measure for hypomania, to be used both in epidemiological research and in clinical use. Existing measures for bipolar disorder focused on identifying personality factors and symptom severity instead of the episodic nature of hypomania or the possible negative consequences in behavioural, affective, or cognitive changes associated. These measures were mostly used in non-clinical populations to identify individuals at risk and were not used as screening instruments. The HCL-32 is a measure intended to have high sensitivity to direct clinicians from many countries to diagnosing individuals in a clinical population with bipolar disorder, specifically bipolar II disorder.
Initially developed by Jules Angst and Thomas Meyer in German, the questionnaire was translated into English and translated back to German to ensure accuracy. The English version of the HCL has been used as the basis for translation in other languages through the same process. The original study that used the HCL in an Italian and a Swiss sample noted the measure’s high sensitivity and a lower sensitivity than other used measures.
The scale includes a checklist of 32 possible symptoms of hypomania, each rated yes or no. The rating “yes” would mean the symptom is present or this trait is “typical of me,” and “no” would mean that the symptom is not present or “not typical” for the person.
Limitations
The HCL suffers from the same problems as other self-report inventories, in that scores can be easily exaggerated or minimised by the person completing them. Like all questionnaires, the way the instrument is administered can influence the final score. If a patient is asked to fill out the form in front of other people in a clinical environment, for instance, social expectations may elicit a different response compared to administration via a postal survey.
Similar reliability scores were found when only using 16 item assessments versus the traditional 32-item format of the HCL-32. A score of at least 8 items was found valid and reliable for distinguishing Bipolar Disorder and Major Depressive Disorder. In a study, 73% of patients who completed the HCL-32 R1 were true bipolar cases identified as potential bipolar cases. However, the HCL-32 R1 does not accurately differentiate between Bipolar I and Bipolar II. However, the 16-item HCL has not been tested as a standalone section in a hospital setting. In addition, while the HCL-32 is a sensitive instrument for hypomanic symptoms, it does not distinguish between bipolar I and bipolar-II disorders. The HCL-32 has not been compared with other commonly used screening tools for bipolar disorder, such as the Young Mania Rating Scale (YMRS)and the General Behaviour Inventory (GBI). The online version of the HCL has been shown to be as reliable as the paper version.
Bipolar disorder in children, or paediatric bipolar disorder (PBD), is a controversial mental disorder in children and adolescents that is mainly diagnosed in the United States, and is hypothesized to be like bipolar disorder (BD) in adults, thus is proposed as an explanation for extreme changes in mood and behaviour accompanying periods of depressed or irritable moods and periods of elevated moods so called manic or hypomanic episodes.
These shifts are sometimes quick, but usually are gradual. The average age of onset of paediatric bipolar disorder is unclear, but the risk increases with the onset of puberty. Bipolar disorder is rare in childhood. Paediatric bipolar disorder is typically more severe and has a poorer prognosis than bipolar disorder with onset in late-adolescence or adulthood.
The DSM has specified that the criteria for bipolar disorder can be applied to children since 1980. However, the exact criteria for diagnosing paediatric bipolar disorder remains controversial and heavily debated. There are big differences in how commonly it is diagnosed across clinics and in different countries. There has been a rapid increase in research on the topic, but training and clinical practice lag behind.
Identifying bipolar disorder in youth is challenging. Children often exhibit chronic rather than episodic mania periods. Almost always, these chronic problems have causes other than bipolar disorder. The criteria for paediatric bipolar disorder can also often be masked by developmental differences. Comorbid disorders make determining what symptoms are signs of bipolar disorder and which are due to other disorders (e.g. OCD, ADHD, disruptive behaviour problems) difficult, leading to complications in treatment. For example, a common treatment for OCD are serotonin re-uptake inhibitors (SRIs), however, SRIs can lead to mood instability and worsening bipolar disorder.[5] The most common misdiagnosis for ADHD in the USA is paediatric bipolar disorder due to hyperactivity being described as prolonged periods of mania. Empirical research conducted in 2004 found that “bipolar disorder (in preadolescence) was initially misdiagnosed in 12 out of 24 youths” (Mahoney, 2004). This is a dangerous misdiagnosis due to the vastly different treatment forms. Firstly, ADHD does not require mood stabilisers like paediatric bipolar disorder. Secondly, the stimulants given to treat ADHD have been shown to cause psychosis and exacerbate mania in paediatric bipolar disorder (Wendling, 2009). This misuse of medication can lead to mood episodes, suicidality, and hospitalisation.
Brief History
Descriptions of children with symptoms similar to contemporary concepts of mania date back to the 18th century. In 1898, a detailed psychiatric case history was published about a 13-year-old that met Jean-Pierre Falret and Jules Baillarger’s criteria for folie circulaire, which is congruent to the modern conception of bipolar I disorder.
In Emil Kraepelin’s descriptions of bipolar disorder in the 1920s, which he called “manic depressive insanity”, he noted the rare possibility that it could occur in children. In addition to Kraepelin, Adolf Meyer, Karl Abraham, and Melanie Klein were some of the first to document bipolar disorder symptoms in children in the first half of the 20th century. It was not mentioned much in English literature until the 1970s when interest in researching the subject increased. It became more accepted as a diagnosis in children in the 1980s after the DSM-III (1980) specified that the same criteria for diagnosing bipolar disorder in adults could also be applied to children.
Recognition came twenty years after, with epidemiological studies showing that approximately 20% of adults with bipolar disorder already had symptoms in childhood or adolescence. Nevertheless, onset before age 10 was thought to be rare, below 0.5% of the cases. During the second half of the century misdiagnosis with schizophrenia was not rare in the non-adult population due to common co-occurrence of psychosis and mania, this issue diminishing with an increased following of the DSM criteria in the last part of the 20th century.
Epidemiology
The prevalence of bipolar in youth is estimated at 2%.
Diagnosis
Diagnosis is made based on a clinical interview by a psychiatrist or other licensed mental health practitioner. There are no blood tests or brain scans to diagnose bipolar disorder. Obtaining information on family history and the use of questionnaires and checklists are helpful in making an accurate diagnosis. Commonly used assessment tools include the:
In both the American Psychiatric Association’s DSM-5 and the World Health Organisation’s ICD-10, the same criteria used to diagnose bipolar disorder in adults are used to make the diagnosis in children with some adjustments to account for differences in age and developmental stage. For example, the DSM-5 specifies that in children, depressive episodes can manifest as persistently irritable moods.
In diagnosing manic episodes, it is important to compare the changes in mood and behaviour to the child’s normal mood and behaviours at baseline instead of to other children or adults. For example, grandiosity (i.e. unrealistic overestimation of one’s intelligence, talent, or abilities) is normal at varying degrees during childhood and adolescence. Therefore, grandiosity is only considered symptomatic of mania in children when the beliefs are held despite being presented with concrete evidence otherwise or when they lead to a child attempting activities that are clearly dangerous, and most importantly, when the grandiose beliefs are an obvious change from that particular child’s normal self-view in between episodes.
Controversy
The diagnosis of childhood bipolar disorder is controversial, although it is recognised that bipolar disorder typical symptoms are dysfunctional and have negative consequences for minors suffering them. Main discussion is centred on whether what is called bipolar disorder in children refers to the same disorder than when diagnosing adults, and the related question on whether adults’ criteria for diagnosis are useful and accurate when applied to children. More specifically, main discussion over diagnosis in children circles around mania symptomatology and its differences between children and adults.
Diagnostic criteria may not correctly separate children with bipolar disorder from other problems such as ADHD, and emphasize fast mood cycles.
Treatment
Medications can produce important side effects, so interventions have been recommended to be closely monitored and families of patients to be informed of the different possible problems that can arise. Atypical antipsychotics are more effective than mood stabilizers, but have more side effects. Typical antipsychotics may produce weight gains as well as other metabolic problems, including diabetes mellitus type 2 and hyperlipidaemia. Extrapyramidal secondary effects may appear with these medications. These include tardive dyskinesia, a difficult-to-treat movement disorder (dyskinesia) that can appear after long-term use of antipsychotics. Liver and kidney damage are a possibility with mood stabilisers.
Psychological treatment usually includes some combination of education on the disease, group therapy and cognitive behavioural therapy (CBT). Children with bipolar disorder and their families are informed, in ways accordingly to their age and family role, about the different aspects of bipolar disorder and its management including causes, signs and symptoms and treatments. Group therapy aims to improve social skills and manage group conflicts, with role-playing as a critical tool. Finally, cognitive-behavioural training is directed towards the participants having a better understanding and control over their emotions and behaviours.
Lithium or Divalproex is recommended for first-line treatment.
Partial (minimal to moderate) improvement with monotherapy, augment with another of the first-line recommendations.
Stage 2: Monotherapy with an alternative drug, then augmentation.
Stage 3: Possible medication combinations – lithium plus Divalproex, lithium plus atypical, or Divalproex plus atypical.
Stage 4: Combination of 2-3 mood stabilisers.
Stage 5: Alternate monotherapy with oxcarbazepine, ziprasidone, or aripiprazole (all Level D).
Stage 6: For nonresponse or intolerable side effects – clozapine for children or adolescents, or electroconvulsive therapy (ECT) for adolescents only.
BPD I, manic or mixed, with psychosis:
Stage 1: Same as BPD I without psychosis except for first-line treatment warrants a combination of mood stabiliser and an atypical antipsychotic.
Stages 2-4: Varying combinations and augmentations.
Stage 5: Alternate monotherapy (oxcarbazepine) plus an atypical antipsychotic.
Prognosis
Chronic medication is often needed, with relapses of individuals reaching rates over 90% in those not following medication indications and almost to 40% in those complying with medication regimens in some studies. Compared to adults, a juvenile onset has in general a similar or worse course, although age of onset predicts the duration of the episodes more than the prognosis. A risk factor for a worse outcome is the existence of additional (comorbid) pathologies.
Children with bipolar disorder are more likely to suicide than other children.
The Schedule for Affective Disorders and Schizophrenia (SADS) is a collection of psychiatric diagnostic criteria and symptom rating scales originally published in 1978.
It is organised as a semi-structured diagnostic interview. The structured aspect is that every interview asks screening questions about the same set of disorders regardless of the presenting problem; and positive screens get explored with a consistent set of symptoms. These features increase the sensitivity of the interview and the inter-rater reliability (or reproducibility) of the resulting diagnoses. The SADS also allows more flexibility than fully structured interviews: Interviewers can use their own words and rephrase questions, and some clinical judgment is used to score responses.
There are three versions of the schedule:
The regular SADS;
The lifetime version (SADS-L); and
A version for measuring the change in symptomology (SADS-C).
Although largely replaced by more structured interviews that follow diagnostic criteria such as DSM-IV and DSM-5, and specific mood rating scales, versions of the SADS are still used in some research papers today.
Relationship with the Research Diagnostic Criteria
The SADS was developed by the same group of researchers as the Research Diagnostic Criteria (RDC). While the RDC is a list of diagnostic criteria for psychiatric disorders, the SADS interview allows diagnoses based on RDC criteria to be made, and also rates subject’s symptoms and level of functioning.
K-SADS
The K-SADS (or Kiddie-SADS) is a version of the SADS adapted for school-aged children of 6–18 years. There are various different versions of the K-SADS, each varying slightly in terms of disorders and specific symptoms covered, as well as the scale range used. All of the variations are still semi-structured interviews, giving the interviewer more flexibility about how to phrase and probe items, while still covering a consistent set of disorders.
The K-SADS-E (Epidemiological version) was developed for epidemiological research. It focused on current issues and episodes only. Most of the items used a four point rating scale.
The K-SADS-PL (Present and Lifetime version) is administered by interviewing the parent(s), the child, and integrating them into a summary rating that includes parent report, child report, and clinical observations during the interview. The interview covers both present issues (i.e., the reason the family is seeking an evaluation) as well as past episodes of the disorders. Most items use a three point rating scale for severity (not present, subthreshold, and threshold – which combines both moderate and severe presentations). It has been used with preschool as well as school-aged children. A 2009 working draft removed all reference to the DSM-III-R criteria (which were replaced with the publication of the DSM-IV in 1994) and made some other modifications. A DSM-5 version is being prepared and validated.
The WASH-U K-SADS (Washington University version) added items to the depression and mania modules and used a six point severity rating for severity.
The Research Diagnostic Criteria (RDC) are a collection of influential psychiatric diagnostic criteria published in late 1970s under auspices of Statistics Section NY Psychiatric Institute, authors were Spitzer, R L; Endicott J; Robins E. PMID 1153649; As psychiatric diagnoses widely varied especially between the USA and Europe, the purpose of the criteria was to allow diagnoses to be consistent in psychiatric research.
Some of the criteria were based on the earlier Feighner Criteria, although many new disorders were included; “The historical record shows that the small group of individuals who created the Feighner criteria instigated a paradigm shift that has had profound effects on the course of American and, ultimately, world psychiatry.”
The RDC is important in the history of psychiatric diagnostic criteria as the DSM-III was based on many of the RDC descriptions, head of DSM III Edition was R L Spitzer.
The Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS) is a semi-structured interview aimed at early diagnosis of affective disorders such as depression, bipolar disorder, and anxiety disorder. There are currently four different versions of the test that are structured to include interviews with both the child and the parents or guardians.
The K-SADS serves to diagnose childhood mental disorders in school-aged children 6-18. The different adaptations of the K-SADS were written by different researchers and are used to screen for many affective and psychotic disorders. Versions of the K-SADS are semi-structured interviews administered by health care providers or highly trained clinical researchers, which gives more flexibility to the interviewer about how to phrase and probe items, while still covering a consistent set of disorders. Due to its semi-structured interview format, time to complete the administration varies based on the youth/adult being interviewed. Most versions of the K-SADS also include “probes”, if these are endorsed, another diagnostic category will be reviewed. If the probe is not endorsed, additional symptoms for that particular disorder will not be queried.
The K-SADS has been found to be reliable and valid in multiple research and treatment settings.
The Schedule for Affective Disorders and Schizophrenia for School Aged Children, or K-SADS, was originally created as an adapted version of the Schedule for Affective Disorders and Schizophrenia, a measure for adults. The K-SADS was written by Chambers, Puig-Antich, et al. in the late 1970s. The K-SADS was developed to promote earlier diagnosis of affective disorders and schizophrenia in children in a way that incorporates reports by both the child and parent and a “summary score” by the interviewer based on observations and teacher ratings.
The first version of the K-SADS differed from other tests on children because it relied on answers to interview questions rather than observances during games and interactions. The 1990s led to the creation of different versions of the K-SADS for different purposes, such as ascertaining lifetime diagnoses (K-SADS-E) or focusing on current episodes (K-SADS-P).
Versions
KSADS-Present Version (KSADS-P)
The KSADS-P was the first version of the K-SADS, developed by Chambers and Puig-Antich in 1978 as a version of the Schedule for Affective Disorders and Schizophrenia adapted for use with children and adolescents 6-19 years old. This version rephrased the SADS to make the wording of the questionnaire pertain to a younger age group. For example, mania symptoms in children might be manifest differently than in adulthood (e.g. children might have not have the same opportunity to spend money impulsively, nor would they likely have access to credit cards or checking accounts; instead, they might give away all their favourite toys or empty their parent’s wallet to gain spending money). The KSADS-P is a structured interview given by trained clinicians or clinical researchers who interview both the child and the parent. This original version assesses symptoms that have occurred in the most current episode (within the week preceding the interview), as well as symptoms that have occurred within the last 12 months. The KSADS-P has many limitations: it does not assess lifetime symptoms and history, does not include many psychiatric diagnoses of interest in childhood (such as autistic spectrum disorders), and does not include diagnosis specific impairment ratings.
KSADS-Present and Lifetime Version (KSADS-PL)
The K-SADS-PL is used to screen for affective and psychotic disorders as well as other disorders, including, but not limited to Major Depressive Disorder, Mania, Bipolar Disorders, Schizophrenia, Schizoaffective Disorder, Generalized Anxiety, Obsessive Compulsive Disorder, Attention Deficit Hyperactivity Disorder, Conduct Disorder, Anorexia Nervosa, Bulimia, and Post-Traumatic Stress Disorder. This semi-structured interview takes 45-75 minutes to administer. It was written by Joan Kaufman, Boris Birmaher, David Brent, Uma Rao, and Neal Ryan. The majority of items in the K-SADS-PL are scored using a 0-3 point rating scale. Scores of 0 indicate no information is available; scores of 1 suggest the symptom is not present; scores of 2 indicate sub-threshold presentation and scores of 3 indicate threshold presentation of symptoms. The KSADS-PL has six components:
Component
Description
Unstructured Introductory Interview – Developmental History
The first part of the interview asks about developmental history and the history of the presenting problem. The interviewer takes detailed notes on the record sheet. Prompts cover basic demographic information, physical and mental health history and prior treatments, current complaints, and the youth’s relations with friends, family, school, and hobbies. This section allows flexibility for the interviewer to collect more information on questions that need elaboration.
Diagnostic Screening Interview
The diagnostic screening interview reviews the most severe current and past symptoms. There are probes and scoring criteria for each symptom presented. Symptoms of disorders are grouped into modules. If the patient does not display any current or past symptoms for the screening questions, then the rest of the module’s questions do not need to be asked.
Completion Checklist Supplement
A supplemental checklist is used to screen for additional disorders.
Appropriate Diagnostic Supplements
These supplements review presence/absence of symptoms for other disorders, including anxiety disorders, behavioural disorders, and substance abuse.
Summary Lifetime Diagnosis Checklist
Based on the previous sections, this section summarises which disorders have been present from first episode to now.
Children’s Global Assessment Scale (C-GAS)
Scores the child’s level of functioning.
KSADS-Epidemiological (KSADS-E)
The KSADS-E, which is the epidemiological version of the KSADS, is a tool to interview parents about possible psychopathology in children from preschool onward. It was developed by Puig-Antich, Orvaschel, Tabrizi, and Chambers in 1980 as a structured interview. The tool examines both past and current episodes, focusing on the most severe past episode and the most current episode. However, this tool does not rate symptom severity; it should only be used to assess presence or absence of symptomatology. This version of the K-SADS introduced screening questions, which, if negative, allowed skipping the remaining diagnostic probes. Furthermore, the K-SADS-E also includes “skip out” criteria when assessing other diagnostic disorders (ADHD, PTSD, etc.), allowing those that screen positive to immediately be interviewed for all of the symptoms regarding that diagnosis, and those that screened negative could “skip out” of being interviewed on the remaining symptoms.
WASH-U-KSADS
The WASH-U version of the K-SADS was written by Barbara Geller and colleagues in 1996. It is a modified version of the 1986 K-SADS. This version is like many other versions of the K-SADS in that it is semi-structured, administered by clinicians to both parent and child separately, and assesses present episodes. However, this version specifically expands the mania section in order to be more applicable to pre-pubertal mania. In particular, it queries presence/absence of rapid cycling. It also includes a section on multiple other DSM-IV diagnoses, and examines both present and lifetime symptoms as well as symptom onset and offset items. These modifications made this specific version particularly useful for phenomenology studies.
KSADS Mania Rating Scale (KMRS) and Depression Rating Scale (KDRS) It also is possible to use the items in the mania and depression modules of some versions of the KSADS to get an interview-based rating of the severity of mood problems. The KMRS and KDRS use a 1 to 6 rating format (the same as in the WASH-U, -P, and PL-Plus versions). Adding up the items provides a measure of the total symptom burden. The KMRS assess 21 symptoms related to mania, hypomania, and rapid cycling. Each item is rated on a 0-6 rating scale. Scores of 0 suggest no information is available (missing data); scores of 1 suggest the symptom is not present at all; scores of 2 suggest the symptom is slightly present; scores of 3 suggest the symptom is mildly severe; scores of 4 suggest the symptom is moderately severe; scores of 5 suggest the symptom is severe; and scores of 6 suggest the symptom is extremely severe. Items with scores of 4 or higher are clinically significant/problematic. Trained clinicians or clinical researchers administer the assessment to both the child and the parent, which each provide their own separate score for each item (P and C), and the total score encompasses the sum of all of the items (S).
The KMRS is an alternative to the Young Mania Rating Scale designed by Young et al. (frequently referred to as the YMRS). The YMRS is more well-known and widely used, but because it was written in 1978, it does not include all of the symptoms of mania from ICD-9 or ICD-10 (nor DSM-IV or DSM-5), as it predated them all. The YMRS was also designed for completion by nurses at the end of their eight-hour shift on an inpatient unit, observing adult patients. The KMRS has several advantages in comparison: It covers all the symptoms used in current versions of ICD and DSM, it was designed for use with children and teenagers, and it was written and validated as an interview. Studies have found excellent internal consistency and inter-rater reliability, as well as exceptionally high correlation with the YMRS. Similarly, the KDRS would be analogous to the Child Depression Rating Scale-Revised. The CDRS-R was also designed to be done as an interview, but the item content predates the current ICD and DSM and omits some important symptoms. The KDRS also shows strong reliability (internal consistency and inter-rater) and exceptionally high correlations with the KDRS.
Impact
The K-SADS is used to measure previous and current symptoms of affective, anxiety, psychotic, and disruptive behaviour disorders. The K-SADS has become one of the most widely used diagnostic interviews in research, particular for projects focused on mood disorders.
The K-SADS-PL has been written and translated into 16 different languages, including Korean, Hebrew, Turkish, Icelandic, and Persian. The K-SADS-PL is also available in several Indian dialects including Kannada, Marathi, Tamil and Telugu.
Limitations
One limitation of the K-SADS is that it requires extensive training to give properly, including observation techniques, score calibration, and re-checks to test inter-rater reliability.
The cause and mechanism of bipolar disorder is not yet known, and the study of its biological origins is ongoing. Although no single gene causes the disorder, a number of genes are linked to increase risk of the disorder, and various gene environment interactions may play a role in predisposing individuals to developing bipolar disorder. Neuroimaging and post-mortem studies have found abnormalities in a variety of brain regions, and most commonly implicated regions include the ventral prefrontal cortex and amygdala. Dysfunction in emotional circuits located in these regions have been hypothesized as a mechanism for bipolar disorder. A number of lines of evidence suggests abnormalities in neurotransmission, intracellular signalling, and cellular functioning as possibly playing a role in bipolar disorder.
Studies of bipolar disorder, particularly neuroimaging studies, are vulnerable to the confounding effects such as medication, comorbidity, and small sample size, leading to underpowered independent studies, and significant heterogeneity.
Brain imaging studies have revealed differences in the volume of various brain regions between patients with bipolar disorder and healthy control subjects.
Aetiology
Genetic
The etiology of bipolar disorder is unknown. The overall heritability of bipolar is estimated at 79%-93%, and first degree relatives of bipolar probands have a relative risk of developing bipolar around 7-10. While the heritability is high, no specific genes have been conclusively associated with bipolar, and a number of hypothesis have been posited to explain this fact. “The polygenic common rare variant” hypothesis suggests that a large number of risk conferring genes are carried in a population, and that a disease manifests when a person has a sufficient number of these genes. The “multiple rare variant” model suggests that multiple genes that are rare in the population are capable of causing a disease, and that carrying one or a few can lead to disease. The familial transmission of mania and depression are largely independent of each other. This raises the possibility that bipolar is actually two biologically distinct but highly comorbid conditions.
A number of genome wide associations have been reported, including CACNA1C and ODZ4, and TRANK1. Less consistently reported loci include ANK3 and NCAN, ITIH1, ITIH3 and NEK4. Significant overlaps with schizophrenia have been reported at CACNA1C, ITIH, ANK3, and ZNF804A. This overlap is congruent with the observation that relatives of probands with schizophrenia are at higher risk for bipolar disorder and vice versa.
In light of associations between bipolar and circadian abnormalities (such as decreased need for sleep and increased sleep latency), polymorphisms in the CLOCK gene have been tested for association, although findings have been inconsistent, and one meta analysis has reported no association with either bipolar or major depressive disorder. Other circadian genes associated with bipolar at relaxed significance thresholds include ARTNL, RORB, and DEC1. One meta analysis reported a significant association of the short allele of the serotonin transporter, although the study was specific to European populations. Two polymorphisms in the tryptophan hydroxylase 2 gene have been associated with bipolar disorder. NFIA has been linked with seasonal patterns of mania.
One particular SNP located on CACNA1C that confers risk for bipolar disorder is also associated with elevated CACNA1C mRNA expression in the prefrontal cortex, and increased calcium channel expression in neurons made from patient induced pluripotent stem cells.
No significant association exists for the BDNF Val66Met allele and bipolar disorder, except possibly in a subgroup of bipolar II cases, and suicide.
Due to the inconsistent findings in GWAS, multiple studies have undertaken the approach of analysing SNPs in biological pathways. Signalling pathways traditionally associated with bipolar disorder that have been supported by these studies include CRH signalling, cardiac β-adrenergic signalling, phospholipase C signalling, glutamate receptor signalling, cardiac hypertrophy signalling, Wnt signalling, notch signalling, and endothelin 1 signalling. Of the 16 genes identified in these pathways, three were found to be dysregulated in the dorsolateral prefrontal cortex portion of the brain in post-mortem studies, CACNA1C, GNG2, and ITPR2.
Advanced paternal age has been linked to a somewhat increased chance of bipolar disorder in offspring, consistent with a hypothesis of increased new genetic mutations.
A meta-analysis was performed to determine the association between bipolar disorder and oxidative DNA damage measured by 8-hydroxy-2′-8-deoxyguanosine (8-OHdG) or 8-oxo-7,8-dihydro-2′-deoxyguanosine (8-oxodG). Levels of 8-OHdG and 8-oxodG are widely used as measures of oxidative stress in mental illnesses. It was determined from this meta-analysis that oxidative DNA damage was significantly increased in bipolar disorder.
Environmental
Manic episodes can be produced by sleep deprivation in around 30% of people with bipolar. While not all people with bipolar demonstrate seasonality of affective symptoms, it is a consistently reported feature that supports theories of circadian dysfunction in bipolar.
Risk factors for bipolar include obstetric complications, abuse, drug use, and major life stressors.
The “kindling model” of mood disorders suggests that major environmental stressors trigger initial mood episodes, but as mood episodes occur, weaker and weaker triggers can precipitate an affective episode. This model was initially created for epilepsy, to explain why weaker and weaker electrical stimulation was necessary to elicit a seizure as the disease progressed. While parallels have been drawn between bipolar disorder and epilepsy, supporting the kindling hypothesis, this model is generally not supported by studies directly assessing it in bipolar subjects.
Neurological Disorders
Mania occurs secondary to neurological conditions between a rate of 2% to 30%. Mania is most commonly seen in right sided lesions, lesions that disconnect the prefrontal cortex, or excitatory lesions in the left hemisphere.
Diseases associated with “secondary mania” include Cushing’s disease, dementia, delirium, meningitis, hyperparathyroidism, hypoparathyroidism, thyrotoxicosis, multiple sclerosis, Huntington’s disease, epilepsy, neurosyphilis, HIV dementia, uraemia, as well as traumatic brain injury and vitamin B12 deficiency.
Pathophysiology
Neurobiological and Neuroanatomical Models
The main loci of neuroimaging and neuropathological findings in bipolar have been proposed to constitute dysfunction in a “visceromotor” network, composed of the mPFC, anterior cingulate cortex (ACC), orbitofrontal cortex (OFC), hippocampus, amygdala, hypothalamus, striatum and thalamus.
A model of functional neuroanatomy produced by a workgroup led by Stephen M. Strakowski concluded that bipolar was characterized by reduced connectivity, due to abnormal pruning or development, in the prefrontal-striatal-pallidal-thalamic-limbic network leading to dysregulated emotional responses. This model was supported by a number of common neuroimaging findings. Dysregulation of limbic structures is evinced by the fact that hyperactivity in the amygdala in response to facial stimuli has been consistently reported in mania. While amygdala hyperactivity is not a uniform finding, a number of methodological challenges could explain discrepancies. As most studies utilize fMRI to measure blood-oxygen-level dependent signal, excess baseline activity could result in null findings due to subtraction analysis. Furthermore, heterogenous study design could mask consistent hyperactivity to specific stimuli. Regardless of directionality of amygdala abnormalities, as the amygdala plays a central role in emotional systems, these findings support dysfunctional emotional circuits in bipolar. A general reduction in ventrolateral prefrontal cortex activity is observed in bipolar, and is lateralised with regard to mood (i.e. left-depression, right-mania), and may underlie amygdala abnormalities. The dorsal ACC is commonly under-activated in bipolar, and is generally implicated in cognitive functions, while the ventral ACC is hyperactived and implicated in emotional functions. Combined, these abnormalities support the prefrontal-striatal-pallidial-thalamic limbic network underlying dysfunction in emotional regulation in bipolar disorder. Strakowski, along with DelBello and Adler have put forward a model of “anterior limbic” dysfunction in bipolar disorder in a number of papers.
In 2007, Green and colleagues suggested a model of bipolar disorder based on the convergence of cognitive and emotional processing on certain structures. For example, the dACC and sgACC were cognitively associated with impairment of inhibition of emotional responses and self monitoring, which could translate to emotional stimuli having excessive impact on mood. Deficits in working memory associated with abnormal dlPFC function could also translate to impaired ability to represent emotional stimuli, and therefore the impaired ability to reappraise emotional stimuli. Dysfunction in the amygdala and striatum has been associated with attentional biases, and may represent a bottom up mechanism of dysfunctional emotional processing.
Blond et al. proposed a model centred on dysfunction in an “amygdala-anterior paralimbic” system. This model was based on the consistent functional and structural abnormalities in the ventral prefrontal cortex and amygdala. The model also proposes a developmental component of bipolar disorder, wherein limbic abnormalities are present early on, but rostral prefrontal abnormalities develop later in the course. The importance of limbic dysfunction early in development is highlighted by the observation that amygdala lesions early in adulthood produce emotional abnormalities that are not present in people who develop amygdala damage in adulthood.
Lateralised seizure sequelae similar to bipolar has been reported in people with mesial temporal lobe seizures, and provides support for kindling hypotheses about bipolar. This observation led to the first experiments with anticonvulsants in bipolar, which are effective in stabilising mood. Studies reporting reduced markers of inhibitory interneurons post-mortem link the analogy with epilepsy to a possible reduction in inhibitory activity in emotional circuits. Overlap with epilepsy extends to include abnormalities in intracellular signalling, biochemistry in the hippocampus and prefrontal cortex, and structure and function of the amygdala.
The phenomenology and neuroanatomy of mania secondary to neurological disorders is consistent with findings in primary mania and bipolar disorder. While the diversity of lesions and difficulty in ruling out premorbid psychiatric conditions limit the conclusions that can be drawn, a number of findings are fairly consistent. Structurally, secondary mania is associated with destructive lesions that tend to occur in the right hemisphere, particularly the frontal cortex, mesial temporal lobe and basal ganglia. Functionally hyperactivity in the left basal ganglia and subcortical structures, and hypoactivity in the right ventral prefrontal and basotemporal cortex have been reported in cases of secondary mania. The destruction of right hemisphere or frontal areas is hypothesized to lead to a shift to excessive left sided or subcortical reward processing.
John O. Brooks III put forward a model of bipolar disorder involving dysregulation of a circuit called the “corticolimbic system”. The model was based on more or less consistent observations of reduced activity in the mOFC, vlPFC, and dlPFC, as well as the more or less consistent observations of increased activity in the amygdala, parahippocampal gyrus, cerebellar vermis, anterior temporal cortex, sgACC, and ACC. This pattern of abnormal activity was suggested to contribute to disrupted cognitive and affective processes in bipolar disorder.
Neurocognition
During acute mood episodes, people with bipolar demonstrate mood congruent processing biases. Depressed patients are quicker to react to negatively valenced stimuli, while manic patients are quicker to react to positively valenced stimuli. Acute mood episodes are also associated with congruent abnormalities during decision making tasks. Depressed bipolar is associated with conservative responding, while manic bipolar is associated with liberal responses. Both depression and mania are associated with similar and broad cognitive impairments, including on tests of attention, processing speed, working memory, executive functions, and reaction time.
Clinically, mania is characterised by spending sprees, poor judgement, and inappropriate speech and behaviour. Congruent with this, mania is associated impulsivity on Go-No Go tasks, deficits in emotional decision making, poor probabilistic reasoning, impaired ability on continuous performance tasks, set shifting, and planning. The clinical phenomenology and neurocognitive deficits are similar to those seen in patients with damage to the orbitofrontal cortex (OFC), which has been reported in functional neuroimaging studies to be abnormal in bipolar mania. Specifically, reduced blood flow to the lateral OFC has been reported, and may reflect dysfunction that leads to the neurocognitive deficits.
In novel environments, both bipolar manic and bipolar euthymic people demonstrate increased activity, exploration and linear movement that is greater than controls, people with ADHD and people with schizophrenia. Using this behavioural pattern in “reverse translational” studies, this behavioural abnormality has been associated with the cholinergic-aminergic hypothesis, which postulates elevated dopaminergic signalling in mania. Reducing the function of DAT using pharmacological or genetic means produces a similar behavioural pattern in animal models. Pharmacological data is consistent with dysfunction of dopamine in bipolar as some studies have reported hypersensitivity to stimulants (however, some studies have found that stimulants effectively attenuate manic behaviour, and co-morbid ADHD and bipolar are effectively treated with stimulants), and the mechanism of antimanic drugs may involve attenuating dopamine signalling.
Hypersensitivity of reward systems is consistent across mood states in bipolar, and is evident in the prodrome. Increases in goal directed behaviour, risk taking, positive emotions in response to reward, ambitious goal setting and inflexibility in goal directed behaviours are present in euthymia. Neuroimaging studies are consistent with trait hypersensitivity in reward systems, as both mania and depression is associated with elevated resting activity in the striatum, and elevated activity in the striatum and OFC during emotional processing, receipt of reward, and anticipation of reward. Increased activity in the striatum and OFC has also been reported in euthymia during anticipation and receipt of reward, although this finding is extremely inconsistent. These abnormalities may be related to circadian rhythm dysfunction in bipolar, including increased sleep latency, evening preference and poor sleep quality, as the neural systems responsible for both processes are functionally linked. A few lines of evidence suggest that elevated dopamine signalling, possibly due to reduced functionality in DAT, underlie abnormalities in reward function. Dopaminergic drugs such as L-DOPA can precipitate mania, and drugs that attenuate dopaminergic signalling extracellularly (antipsychotics) and intracellularly (lithium) can be efficacious in treating mania. While a large body of translational evidence exists to support DAT hypofunction, in vivo evidence is limited to one study reporting reduced DAT binding in the caudate.
Neuroimaging
Structural
In a review of structural neuroimaging in bipolar disorder, Strakowski proposed dysfunction in an iterative emotional network called the “anterior limbic network”, composed of the thalamus, globus pallidus, striatum, vlPFC, vmPFC, ACC, amygdala, dlPFC, and cerebellar vermis. Structural imaging studies frequently find abnormalities in these regions which are putatively involved in emotional and cognitive functions that are disrupted in bipolar disorder. For example, while structural neuroimaging studies do not always find abnormal PFC volume in bipolar disorder, when they do, PFC volume is reduced. Furthermore, reduced PFC volume is associated with response inhibition deficits and duration of illness. When the PFC at large is not examined and the focus is narrowed to the OFC/vPFC, results more consistently observed reductions, although not in bipolar youth. The sgACC volume is observed to be reduced not only in bipolar disorder, but also in unipolar disorder, as well as people with a family history of affective disorders. Enlargement of the striatum and globus pallidus are commonly found, and although some studies fail to observe this, at least one study has reported no volumetric but subtle morphometric abnormalities.
Structural neuroimaging studies consistently report increased frequency of white matter hyperintensities in people with bipolar. However, whether or not the lesions play a causative role is unknown. It is possible that they are a result of secondary factors, such as the processes underlying an increased risk of cardiovascular disease in bipolar. On the other hand, the observation of reduced white matter integrity in frontal-subcortical regions makes it possible that these hyperintensities play a role dysfunction between limbic and cortical regions. Global brain volume and morphology are normal in bipolar. Regional deficits in volume have been reported in ventrolateral and dorsolateral prefrontal regions. Based on this, it has been suggested that reduced limbic regulation by prefrontal regions plays a role in bipolar. Findings related to the volume of the basal ganglia have been inconsistent.
In healthy controls, amygdala volume is inversely related to age. This relationship is reversed in bipolar disorder, and meta analyses have found reduced amygdala volume in paediatric bipolar disorder, and increased amygdala volume in adulthood. This is hypothesized to reflect abnormal development of amygdala, possibly involving impaired synaptic pruning, although this may reflect medication or compensatory effects; that is, these abnormalities may not be involved in the mechanism of bipolar, and may instead be a consequence.
A 2016 meta analysis reported that bipolar disorder was associated with grey matter reductions bilaterally in the ACC, vmPFC, and insula extending to the temporal lobe. When compared with grey matter reductions in unipolar depression, significant overlap occurred in the insular and medial prefrontal regions. Although unipolar depression was associated with reductions in the ventral most and dorsal most regions of the mPFC and bipolar with a region near the genu of the corpus callosum, the overlap was still statistically significant. Similar to the overlap with major depression, a significant overlap of bipolar disorder with schizophrenia in grey matter volume reduction occurs in the anterior cingulate cortex, medial prefrontal cortex, lateral prefrontal cortex and bilateral insula.
A 2010 meta analysis of differences in regional grey matter volume between controls and bipolar disorder reported reductions bilaterally in the inferior frontal cortex and insula, which extended more prominently in the right side to include the precentral gyrus, as well as grey matter reductions in the pregenual anterior cingulate cortex (BA24) and anterior cingulate cortex (BA32). One meta analysis reported enlargement of the lateral ventricles and globus pallidus, as well as reductions in hippocampus volume and cross sectional area of the corpus callosum. Another meta analysis reported a similar increase volumes of the globus pallidus and lateral ventricles, as well as increased amygdala volume relative to people with schizophrenia. Reductions have also been reported in the right inferior frontal gyrus, insula, pars triangularis, pars opercularis, and middle and superior temporal gyrus. Structural neuroimaging in people who are susceptible to bipolar disorder (i.e. have a number of relatives with bipolar disorder) have produced few consistent results. Consistent abnormalities in adult first degree relatives include larger insular cortex volumes, while offspring demonstrate increased right inferior frontal gyrus volumes.
The ENIGMA bipolar disorder working group reported cortical thinning in the left Pars opercularis (BA44-inferior frontal gyrus), left fusiform gyrus, left rostral middle frontal cortex, right inferior parietal cortex, along with an increase in the right entorhinal cortex. Duration of illness was associated with reductions bilaterally in the pericalcarine gyrus, left rostral anterior cingulate and right cuneus, along with increases in the right entorhinal cortex. Treatment with lithium was associated with increased cortical thickness bilaterally in the superior parietal gyrus, left paracentral gyrus, and left paracentral lobule. A history of psychosis was associated with reduced surface area in the right frontal pole. Another study on subcortical abnormalities by the same research group reported reductions in the hippocampus, amygdala, and thalamus, along with ventricular enlargement.
One meta analysis reported that when correcting for lithium treatment, which was associated with increased hippocampal volume, people with bipolar demonstrate reduced hippocampus volume.
White matter is reduced in the posterior corpus callosum, regions adjacent to the anterior cingulate, the left optic radiation, and right superior longitudinal tract, and increased in the cerebellum and lentiform nuclei.
Functional
Studies examining resting blood flow, or metabolism generally observed abnormalities dependent upon mood state. Bipolar depression is generally associated with dlPFC and mOFC hypometabolism. Less consistent associations include reduced temporal cortex metabolism, increased limbic metabolism and reduced ACC metabolism. Mania is also associated with dlPFC and OFC hypometabolism. Limbic hypermetabolism is more consistent than in bipolar depression, but the overall study quality is low due to limitations associated with neuroimaging in acutely manic patients. Another review reported that mania is generally associated with frontal/ventral hypoactivation, while depression is generally associated with the opposite. A degree of lateralization with regard to abnormalities has been reported, with mania being associated with the right hemisphere, and depression the left. Trait abnormalities in euthymic patients have been observed, including hypoactivity in the ventral prefrontal cortex, and hyperactivity in the amygdala.
During cognitive or emotional tasks, functional neuroimaging studies, consistently find hyperactivation of the basal ganglia, amygdala, and thalamus. Prefrontal abnormalities are less consistently reported, although hyperactivation in the ventral prefrontal cortex is a fairly consistent finding. Hyperactivity in the amygdala and hypoactivity in the medial and ventral prefrontal cortex during exposure to emotional stimuli has been interpreted as reflecting dysfunction in emotional regulation circuits. Increased effective connectivity between the amygdala and orbitofrontal cortex, and elevated striatal responsiveness during reward tasks have been interpreted as hyper-responsiveness in positive emotion and reward circuitry. The abnormal activity in these circuits has been observed in non-emotional tasks, and is congruent with changes in grey and white matter in these circuits. Neural response during reward tasks differentiates unipolar depression from bipolar depression, with the former being associated with reduced neural response and the latter being associated with elevated neural response. An ALE meta analysis of functional neuroimaging comparing adults and adolescents found a larger degree of hyperactivity in the inferior frontal gyrus and precuneus, as well as a larger degree of hypoactivity in the anterior cingulate cortex in adolescents relative to adults.
Regardless of mood state, during response inhibition tasks, people with bipolar disorder underactivate the right inferior frontal gyrus. Changes specific on euthymia include hyperactivations in the left superior temporal gyrus and hypoactivations in the basal ganglia, and changes specific to mania include hyperactivation in the basal ganglia. A meta analysis of fMRI studies reported underactivations in the inferior frontal gyrus and putamen and hyperactivation of the parahippocampus, hippocampus, and amygdala. State specific abnormalities were reported for mania and euthymia. During mania, hypoactivation was significant in the inferior frontal gyrus, while euthymia was associated with hypoactivation of the lingual gyrus and hyperactivation of the amygdala.
A meta analysis using region of interest (as opposed to statistical parametric mapping) analysis reported abnormalities across paradigms for euthymic, depressed, and manic subjects. In bipolar mania, reduced activity was reported in the superior, middle, and inferior frontal gyri, while increased activity was reported in the parahippocampal, superior temporal, middle temporal, and inferior temporal gyri. In bipolar depression, reduced activity was reported in the sgACC, ACC, and middle frontal gyrus. In euthymia, reduced activity was reported in the dlPFC, vlPFC, and ACC, while increased activity was reported in the amygdala. During studies examining response to emotional faces, both mania and euthymia were reported to be associated with elevated amygdala activity.
An activation likelihood estimate meta analysis of bipolar studies that used paradigms involving facial emotions reported a number of increases and decreases in activation compared to healthy controls. Elevated activity was reported in the parahippocampal gyrus, putamen, and pulvinar nuclei, while reduced activity was reported bilaterally in the inferior frontal gyrus. Compared to major depressive disorder, bipolar patients overactivated the vACC, pulvinar nucleus, and parahippocampus gyrus/amygdala to a greater degree, while underactivating the dACC. Bipolar subjects overactivated parahippocampus for both fearful and happy expressions, while the caudate and putamen were overactived for happiness and fear respectively. Bipolar subjects also underactivated the ACC for both fearful and happy expressions, while the IFG was underactivated for fearful expressions only. These results were interpreted as reflecting increased engagement with emotionally salient stimuli in bipolar disorder.
Specific symptoms have been linked to various neuroimaging abnormalities in bipolar disorder, as well as schizophrenia. Reality distortion, disorganisation, and psychomotor poverty have been linked to prefrontal, thalamic, and striatal regions in both schizophrenia and bipolar (Table below).
Symptom Dimension
Implicated Regions in Bipolar
Implicated Regions in Schizophrenia
Disorganisation
1. Hypofunction in the ventrolateral prefrontal cortex (vlPFC). 2. Hypofunction in the medial prefrontal cortex (mPFC)/ACC.
1. Hypofunction in the medial prefrontal cortex (mPFC). 2. Hypofunction in the dorsolateral prefrontal cortex (dlPFC). 3. Hypofunction in the cerebellum. 4. Hypofunction in the insula. 5. Hypofunction in the temporal cortex.
Reality Distortion
1. Functional abnormalities in prefrontal and thalamic regions.
1. Reduced grey matter in perisylvian and thalamic regions. 2. Hypofunction of the amygdala, mPFC and hippocampus/parahippocampus.
Psychomotor Poverty
1. Functional abnormalities in the vlPFC and ventral striatum.
1. Reduced grey matter in the vlPFC, mPFC and dlPFC. 2. Reduced grey matter in the striatum, thalamus, amygdala and temporal cortices.
Frontal Cortex
Different regions of the ACC have been studied in the literature, with the subgenual (sgACC) and rostral (rACC) parts being largely separated. Grey matter volume in the sgACC has been, albeit with some exceptions, found to be reduced in bipolar. Along with this, bipolar is associated with increased blood flow in the sgACC that normalises with treatment. Congruent with these abnormalities is a reduction in glial cells observed in post mortem studies, and reduced integrity of white matter possibly involving a hemispheric imbalance. Findings in the rACC are largely the same as the sgACC (reduced GM, increased metabolism), although more studies have been carried out on protein expression and neuronal morphology. The rACC demonstrates reduced expression NMDA, kainate and GABA related proteins. These findings may be compensating for increased glutaminergic afferents, evidenced by increased Glx in MRS studies. One VBM study reported reduced grey matter in the dACC. Inconsistent results have been found during functional neuroimaging of cognitive tasks, with both decreased and increased activation being observed. Decreased neuron volume and a congruent increase in neural density have been found in the dACC. Reduced expression of markers of neural connectivity have been reported (e.g. synaptophysin, GAP-43), which is congruent with the abnormal structural connectivity observed in the region.
The orbitofrontal cortex demonstrates reduced grey matter, functional activity, GAD67 mRNA, neuronal volume in layer I, and microstructural integrity in people with bipolar.
Although the role of acute mood states is unknown, grey matter volume is generally reported as reduced in the dlPFC, along with resting and task evoked functional signals. Signals of myelination and density of GABAegic neurons is also reduced in the dlPFC, particularly in layers II-V.
Neurochemistry
Magnetic Resonance Spectroscopy (MRS)
Increased combined glutamine and glutamate (Glx) have been observed globally, regardless of medication status. Increased Glx has been associated with reduced frontal mismatch negativity, interpreted as dysfunction in NMDA signalling. N-acetyl aspartate levels in the basal ganglia are reduced in bipolar disorder, and trends towards increased in the dorsolateral prefrontal cortex. NAA to creatine ratios are reduced in the hippocampus.
One review of magnetic resonance spectroscopy studies reported increased choline in the basal ganglia, and cingulate as well as a decreased in NAA in the dlPFC and hippocampus. State specific findings were reported to include elevated phosphomonoesters during acute mood states, and reduced inositol with treatment. Another review reported inositol abnormalities in the basal ganglia, and frontal, temporal and cingulate regions. The finding of a trend towards increased NAA concentrations in the dlPFC may be due to medication status, as treatment with lithium or valproate has been noted to lead to null findings, or even elevated levels of NAA in the frontal cortex. In unmedicated populations, reduced NAA consistently found in the prefrontal cortex, particularly the dlPFC.
Various hypotheses related to monoamines have been proposed. The biogenic amine hypothesis posits general dysregulation of monoamines underlies bipolar and affective disorders. The cholinergic aminergic balance hypothesis posits that an increased ratio of cholinergic activity relative to adrenergic signalling underlies depression, while increased adrenergic signalling relative to cholinergic signalling underlies mania. The permissive hypothesis suggests that serotonin is necessary but not sufficient for affective symptoms, and that reduced serotonergic tone is common to both depression and mania.
Studies of the binding potential of dopamine receptor D2 and dopamine transporter have been inconsistent but dopamine receptor D1’s binding potential has been observed to be decreased. Drugs that release dopamine produce effects similar to mania, leading some to hypothesize that mania involves increased catecholaminergic signalling. Dopamine has also been implicated through genetic “reverse translational” studies demonstrating an association between reduced DAT functionality and manic symptoms. The binding potential of muscarinic receptors are reduced in vivo during depression, as well as in post mortem studies, supporting the cholinergic aminergic balance hypothesis.
The role of monoamines in bipolar have been studied using neurotransmitter metabolites. Reduced concentration of homovanillic acid, the primary metabolite of dopamine, in the cerebrospinal fluid (CSF) of people with depression is consistently reported. This finding is related to psychomotor retardation and anhedonia. Furthermore, parkinson’s disease is associated with high rates of depression, and one case study has reported the abolishment of parkinson’s symptoms during manic episodes. The binding potential of VMAT2 is also elevated in bipolar I patients with a history of psychosis, although this finding is inconsistent with finding that valproate increases VMAT2 expression in rodents. One study on DAT binding in acutely depressed people with bipolar reported reductions in the caudate but not putamen.
Studies of serotonin’s primary metabolite 5-HIAA have been inconsistent, although limited evidence points towards reduced central serotonin signalling in a subgroup of aggressive or suicidal patients. Studies assessing the binding potential of the serotonin transporter or serotonin receptors have also been inconsistent, but generally point towards abnormal serotonin signalling. One study reported both increased SERT binding in the insula, mPFC, ACC and thalamus, and decreased SERT binding in the raphe nuclei in acutely depressed bipolar. Serotonin may play a role in mania by increasing the salience of stimuli related to reward.
One more line of evidence that suggests a role of monoamines in bipolar is the process of antidepressant related affective switches. Selective serotonin reuptake inhibitors and more frequently, tricyclic antidepressants (TCAs) are associated with between a 10%-70% risk of affective switch from depression to mania or hypomania, depending upon the criteria used. The more robust association between TCAs and affective switches, as opposed to more selective drugs, has been interpreted as indicating that more extensive perturbation in monoamine systems is associated with more frequent mood switching.
Hypothalamic Pituitary Adrenal Axis
Bipolar disorder is associated with elevated basal and dexamethasone elicited cortisol and adrenocorticotropic hormone (ACTH). These abnormalities are particularly prominent in mania, and are inversely associated with antipsychotic use. The incidence of psychiatric symptoms associated with corticosteroids is between 6% and 32%. Corticosteroids may precipitate mania, supporting the role of the HPA axis in affective episodes. Measures from urinary versus salivary cortisol have been contradictory, with one study of the former concluding that HPA hyperactivity was a trait marker, while a study of the latter concluded that no difference in HPA activity exists in remission. Measurement during the morning are thought to be more sensitive due to the cortisol awakening response. Studies are generally more consistent, and observe HPA hyperactivity.
Neurotrophic Factors
Brain derived neurotrophic factor levels are peripherally reduced in both manic and depressive phases.
Intracellular Signalling
The levels of Gαs but not other G proteins is increased in the frontal, temporal and occipital cortices. The binding of serotonin receptors to G proteins is also elevated globally. Leukocyte and platelet levels of Gαs and Gαi is also elevated in those with bipolar disorder. Downstream targets of G protein signalling is also altered in bipolar disorder. Increased levels of adenylyl cyclase, protein kinase A (PKA), and cyclic adenosine monophosphate induced PKA activity are also reported. Phosphoinositide signalling is also altered, with elevated levels of phospholipase C, protein kinase C, and Gαq being reported in bipolar. Elevated cAMP stimulated phosphorylation or Rap1 (a substrate of PKA), along with increased levels of Rap1 have been reported in peripherally collected cells of people with bipolar. Increased coupling of serotonin receptors to G proteins has been observed. While linkage studies performed on genes related to G protein signalling, as well as studies on post mortem mRNA concentration fail to report an association with bipolar disorder, the overall evidence suggests abnormal coupling of neurotransmission systems with G proteins.
Mania may be specifically associated with protein kinase C hyperactivity, although most evidence for this mechanism is indirect. The gene DGKH has been reported in genome wide association studies to be related to bipolar disorder, and it is known to be involved in PKC regulation. Manipulation of PKC in animals produces behavioural phenotypes similar to mania, and PKC inhibition is a plausible mechanism of action for mood stabilisers. Overactive PKC signalling may lead to long term structural changes in the frontal cortex as well, potentially leading to progression of manic symptoms.
Glycogen synthase kinase 3 has been implicated in bipolar disorder, as bipolar medications lithium and valproate have been shown to increase its phosphorylation, thereby inhibiting it. However, some postmortem studies have not shown any differences in GSK-3 levels or the levels of a downstream target β-catenin. In contrast, one review reported a number of studies observing reduced expression of β-catenin and GSK3 mRNA in the prefrontal and temporal cortex.
Excessive response of arachidonic acid signalling cascades in response to stimulation by dopamine receptor D2 or NMDA receptors may be involved in bipolar mania. The evidence for this is primarily pharmacological, based on the observation that drugs that are effective in treating bipolar reduced AA cascade magnitude, while drugs that exacerbate bipolar do the opposite.
Calcium homeostasis may be impaired across all mood states. Elevated basal intracellular, and provoked calcium concentrations in platelets and transformed lymphoblasts are found in people with bipolar. Serum concentrations of calcium are also elevated, and abnormal calcium concentrations in response to stimulation of olfactory neurons is also observed. These findings are congruent with the genetic association of bipolar with CACNAC1, an L-type calcium channel, as well as the efficacy of anti-epileptic agents. Normal platelets placed in plasma from people with bipolar disorder do not demonstrate elevated levels of intracellular calcium, indicating that dysfunction lies intracellularly. One possible mechanism is that elevated inositol triphosphate (IP3) caused by hyperactive neuronal calcium sensor 1 causes excessive calcium release. Serum levels of S100B (a calcium binding protein) are elevated in bipolar mania.
Mitochondrial Dysfunction
Some researchers have suggested bipolar disorder is a mitochondrial disease. Some cases of familial chronic progressive external ophthalmoplegia demonstrate increased rates of bipolar disorder before the onset of CPEO, and the higher rate of maternal inheritance patterns support this hypothesis. Downregulation of genes encoding for mitochondrial subunits, decreased concentration of phosphocreatine, decreased brain pH, and elevated lactate concentrations have also been reported. Mitochondrial dysfunction may be related to elevated levels of the lipid peroxidation marker thiobarbituric acid reactive substances, which are attenuated by lithium treatment.
Neuropathology
A number of abnormalities in GABAergic neurons have been reported in people with bipolar disorder. People with bipolar demonstrate reduced expression of GAD67 in CA3/CA2 subregion of the hippocampus. More extensive reductions of other indicators of GABA function have been reported in the CA4 and CA1. Abnormal expression of kainate receptors on GABAergic cells have been reported, with reductions in GRIK1 and GRIK2 mRNA in the CA2/CA3 being found in people with bipolar. Decreased levels of HCN channels have also been reported, which, along with abnormal glutamate signalling, could contribute to reduced GABAergic tone in the hippocampus.
The observation of increased Glx in the prefrontal cortex is congruent with the observation of reduced glial cell counts and prefrontal cortex volume, as glia play an important role in glutamate homeostasis. Although the number and quality of studies examining NMDA receptor subunits is poor, evidence for reduced NMDA signalling and reduced contribution from the NR2A subunit is consistent.
Decreased neuron density and soma size in the ACC and dlPFC has been observed. The dlPFC also demonstrates reduced glial density, a finding that is less consistent in the ACC. The reduction in cell volume may be due to early stage apoptosis, a mechanism that is supported by studies observing reduced anti-apoptotic gene expression in both peripheral cells and neurons, as well as the reduction in BDNF that is consistently found in bipolar. Reductions in cortical glia are not found across the whole cortex (e.g. somatosensory areas demonstrate normal glial density and counts), indicating that systematic dysfunction in glial cells is not likely; rather, abnormal functionality of connectivity in specific regions may result in abnormal glia, which may in turn exacerbate dysfunction.
Dendritic atrophy and loss of oligodendrocytes is found in the medial prefrontal cortex, and is possibly specific to GABAergic neurons.
Immune Dysfunction
Elevated levels of IL-6, C-reactive protein (CRP) and TNFα have been reported in bipolar. Levels of some (IL-6 and CRP) but not all (TNFα) may be reduced by treatment. Increases in IL-6 have been reported in mood episodes, regardless of polarity. Inflammation has been consistently reported in bipolar disorder, and the progressive nature lies in dysregulation of NF-κB.
2016 – Frances Cress Welsing, American psychiatrist and author (b. 1935).
Frances Cress Welsing
Frances Luella Welsing (née Cress; 18 March 1935 to 02 January 2016) was an American psychiatrist and well-known proponent of the Black supremacist melanin theory. Her 1970 essay, The Cress Theory of Colour-Confrontation and Racism (White Supremacy), offered her interpretation of what she described as the origins of white supremacy culture.
She was the author of The Isis Papers: The Keys to the Colours (1991).
The Child Mania Rating Scales (CMRS) is a 21-item diagnostic screening measure designed to identify symptoms of mania in children and adolescents aged 9-17 using diagnostic criteria from the DSM-IV, developed by Pavuluri and colleagues.
There is also a 10-item short form. The measure assesses the child’s mood and behaviour symptoms, asking parents or teachers to rate how often the symptoms have caused a problem for the youth in the past month. Clinical studies have found the CMRS to be reliable and valid when completed by parents in the assessment of children’s bipolar symptoms. The CMRS also can differentiate cases of paediatric bipolar disorder from those with ADHD or no disorder, as well as delineating bipolar subtypes. A meta-analysis comparing the different rating scales available found that the CMRS was one of the best performing scales in terms of telling cases with bipolar disorder apart from other clinical diagnoses. The CMRS has also been found to provide a reliable and valid assessment of symptoms longitudinally over the course of treatment. The combination of showing good reliability and validity across multiple samples and clinical settings, along with being free and brief to score, make the CMRS a promising tool, especially since most other checklists available for youths do not assess manic symptoms.
Background
The Child Mania Rating Scale (CMRS) was created as a complement already existing measures like the Altman Self-Rating Mania Scale and the Young Mania Rating Scale, which were formulated for adults. The purpose of the CMRS is to both assess the symptoms of mania in paediatric bipolar disorder, and to accurately discriminate the symptoms of mania from symptoms of ADHD. It is important that the CMRS accurately discriminate from symptoms of ADHD because core symptoms of adolescent Bipolar Disorder and ADHD are shared between the two disorders: hyperactivity, impulsivity, and distractibility. The CMRS was designed specifically for younger children who may or may not have the ability to accurately answer questions about their behaviour. As a result, the questionnaire is filled out by parents are/or caregivers who work with the children on a daily basis. Previous mania scales were designed for use by either the clinician or the patient. Therefore, the CMRS is unique in that it allows parents and caregivers to contribute information about their child’s symptoms. This is especially important in cases where the child may be too young to fill out the questionnaires themselves.
Historically, effective rating and diagnosis of mania has been limited. Though many mania scales have been tested on adult populations, the Young Mania Rating Scale (YMRS) – which was tested against the child version (CMRS) as standard measure for screening mania- is the only adult scale that has also been studied for validity and reliability in prepubertal children. Previous attempts include the Beigel Scale/Manic State Rating Scale (MSRS) and the Patterson Scale, which used nurse and clinician reports to rate levels of mania. Neither scale effectively and consistently captured levels of mania in patients. Other measures of paediatric mania are generally limited because they are completed by the clinician, introducing potential for bias, and because they lack the depth necessary to differentiate between patient-specific ways in which symptoms are presented. The CMRS Parent and Teacher versions attempt to address some of the limitations by including a checklist that can gather information about behaviour at home, school, and other settings, rather than focusing only on what a clinician could directly observe. One study examined the accuracy of a shortened version of the CMRS-P, which included only 10 items, and found that its accuracy was similar to the full scale.
Typically, the CMRS takes only 10-15 minutes to administer. The questions ask about behaviour-specific actions and tendencies the child may have exhibited within the past month. The parent rates the behaviour on a scale from 1 to 4, where 1=never/rarely, 2=sometimes, 3=often, and 4=very often. A clinician examines the total score and determines if the child has ADHD or Bipolar Disorder. If a diagnosis Bipolar Disorder is deemed to be appropriate, the clinician will also determine the sub-type.
Versions
There is a short version (10 items) of the CMRS called the Brief CMRS/Brief CMRS-P. The shorter version was created because a shorter version is preferred to longer assessments if the shorter gives similar accuracy, which it does. Additionally, there is a teacher’s version of the CMRS called the CMRS-Teacher (CMRS-T).
Reliability and Validity
Reliability
Table 1: Rubric for evaluating norms and reliability for the Child Mania Rating Scale.
Designed originally as a self-report scale; parent and youth report correlate about the same as cross-informant scores correlate in general.
Test-Retest Reliability
Adequate
r = .96 over 1 week. Data on test-retest reliability over longer periods are needed.
Repeatability
Not published
No published studies formally checking repeatability.
Construct validity analyses (Exploratory Factor Analysis and Confirmatory Factor Analysis) for the CMRS-P indicated that the scale is unidimensional. Internal consistency measured by Cronbach’s alpha was .96 in a sample consisting of ADHD, Bipolar, and healthy control participants. In a sample of participants with bipolar disorder, the cronbach’s alpha was 91. Additionally, it has the ability to accurately differentiate paediatric bipolar disorder from ADHD and healthy controls greater than 90% of the time.
The teacher version (CMRS-T) also has 21 items. The internal consistency, measured by Cronbach’s alpha, was .86. Correlations between the parent and teacher versions of the CMRS range from .23 to .27. The CMRS teacher version has not been shown to discriminate bipolar from nonbipolar cases at better than chance levels and is not recommended for use in clinical practice for diagnosing bipolar disorder in children.
Validity
Table 2: Evaluation of validity and utility for the Child Mania Rating Scale
Criterion
Rating (Adequate, Good, Excellent, Too Good)
Explanation
Content Validity
Excellent
Covers both DSM diagnostic symptoms and a range of associated features. Consistently distinguishes between PBP sub-types and comorbid disorders.
Construct Validity (e.g. Predictive, Concurrent, Convergent, and Discriminant Validity)
Excellent
Shows convergent validity with other symptom scales. Correlations between CMRS-P and other several clinician-rating scales intended to measure manic symptoms (e.g. Washington University Schedule for Affective Disorder and Schizophrenia mania module, the Schedule for Affective Disorders and Schizophrenia Mania Rating Scale, and the Young Mania Rating Scales) were excellent (.78 to .98).
Discriminative Validity
Excellent/Too Good
Preliminary studies show that CMRS scores discriminate cases with unipolar and bipolar mood disorders from other clinical disorders. AUCs of >.90 are quite high. Comparison to healthy controls might imply unrealistic performance when compared to realities of clinical practice.
Validity Generalisation
Adequate
Shown to be effective for ethnically representative samples. More research and multiple settings are needed to sufficiently determine generalization.
Treatment Sensitivity
Good
The CMRS-P has also been found to be sensitive in detecting symptom change over the course of treatment in multiple studies.
Clinical Utility
Excellent
Free (public domain), designed to be completed in 10-15 minutes, preliminary data are promising. Less research than some of the other contenders, but easier reading level than General Behaviour Inventory and more sensitive to treatment effects than Mood Disorder Questionnaire.
Development and History
The CMRS was developed as a shorter, reliable, and valid parent-report screening instrument for mania. The short form was derived from the CMRS 21 item scale which is the first original mania rating scale developed for children and adolescents. It was not developed from the Young Mania Rating Scale (YMRS) that was originally designed for adults, ‘Young’ being the name of the author than the fact that it was a scale for ‘young’ population. The YMRS was derived from the Parent-Young Mania Rating Scale (P-YMRS). This scale, developed from the YMRS, was created for use with adult inpatients. The items of the P-YMRS did not include the updated DSM-IV criteria for adolescent Bipolar Disorder, and it includes several items with poor factor loadings. Furthermore, the content is not developmentally appropriate for children, as many of the items require insight or appearance, which are irrelevant to young children. Another promising measure is the GBI as it has good psychometric properties. However, the GBI is lengthy and complicated and requires the child to have at least a 7th-grade reading ability. One of the most widely used measures of mania symptoms is the Kiddie Schedule for Affective Disorders and Schizophrenia mania section. However, this measure is extremely extensive and requires much clinical training to administer.
During the development of the CMRS, researchers found that reliable and more accurate diagnostic accuracy is found in parent reports in comparison to teacher reports or self-reports and that these other reports rarely added new information to the parent report. Furthermore, the areas under the curve (AUC) of parent-rated instruments reported modest to excellent validity. Based on the evidence, the developers of the CMRS chose to create a measure that relied mainly on parent report.
Other parent report measures have been used to screen for Paediatric Bipolar Disorder, but these measures were not developed to look specifically for mania. One such measure is the Child Behaviour Checklist (CBCL). The CBCL, in addition to providing markers of psychopathology, has been used to detect mania in children. However, on the CBCL, researchers saw a consistent pattern of elevated scores, especially on the following symptoms: aggressive behaviour, attention problems, delinquency, anxiety, and depression. This pattern may be due to the high comorbidity of ADHD, oppositional defiant disorder, conduct disorder, and anxiety disorders in children with paediatric Bipolar Disorder. And although the CBCL is a reliable and validated measure, low scores on the CBCL may only rule out mania – conversely, it would be erroneous to rule in mania using CBCL scores alone.
For these reasons, the CMRS was developed to accurately and reliably assess mania in paediatric Bipolar Disorder, and differentiate its symptoms from other disorders with high comorbidity with paediatric Bipolar Disorder.
Impact
Though there is no gold-standard screening tool for Paediatric Bipolar Disorder, the CMRS has been described as a promising and useful tool for such a purpose. For example, institutional protocols for diagnosing and evaluating Bipolar Disorder in children may use the CMRS as an initial screening tool to establish the need to further evaluation of mania symptoms. In addition, the parent version of the CMRS (the CMRS-P) has been used in research studies to detect changes in children’s mania symptoms due to pharmacotherapy or psychotherapy. The CMRS is the first measure specifically developed for the purpose of screening for Bipolar Disorder in children.[30] As such, it offers an alternative to broadband rating scales like the Child Behaviour Checklist, which has been used as a screening tool for Bipolar Disorder in children with mixed findings regarding its reliability.
Furthermore, the CMRS-P (both the brief and full versions) have shown to be effective in distinguishing between mania and ADHD. The brief version effectively retains characteristics of the original CMRS, allowing for wider application and longitudinal use. Psychometric studies of the CMRS has demonstrated that the measure has excellent reliability and validity. Internal consistency is excellent and the measure correlates with clinician-administered interview measures for diagnosing paediatric mania. The measure is also accurately able to differentiate symptoms of paediatric Bipolar Disorder from ADHD and healthy control groups more than 90% of the time. Furthermore, the use of the CMRS in pharmacological research suggests that this measure is sensitive to treatment over time, which means that you can use this measure to assess treatment effectiveness.
Limitations
The CMRS suffers from the same problems as other self-report inventories, in that scores can be easily exaggerated or minimised by the person completing them – in this case, the parent or teacher – in a phenomenon called the social desirability bias. Like all questionnaires, the way the instrument is administered can also influence the final score. If a person is asked to fill out the form in front of other people in a clinical environment, for instance, social expectations have been shown to elicit a different response compared to administration via a postal survey. The age of the youth also may matter. Although the Child Mania Rating Scale has been shown to be a valid and reliable measure of mania in children, one concern is that its validity might change as the youth becomes an adolescent, and parents or teachers have less influence and awareness about the youth’s behaviour outside of the home or school. Additionally, it is also unclear of the CMRS’s ability to assess the change in mania systems as a child cycles out of mania and into depression.
Use in Other Populations
While the CMRS has not been validated in other languages, the CBCL, YMRS, GBI, and KSADS all have. However, the CMRS has been tested and translated into Spanish. The CMRS is available in fourteen languages with back translation through native/bilingual speakers, though not tested in all languages.
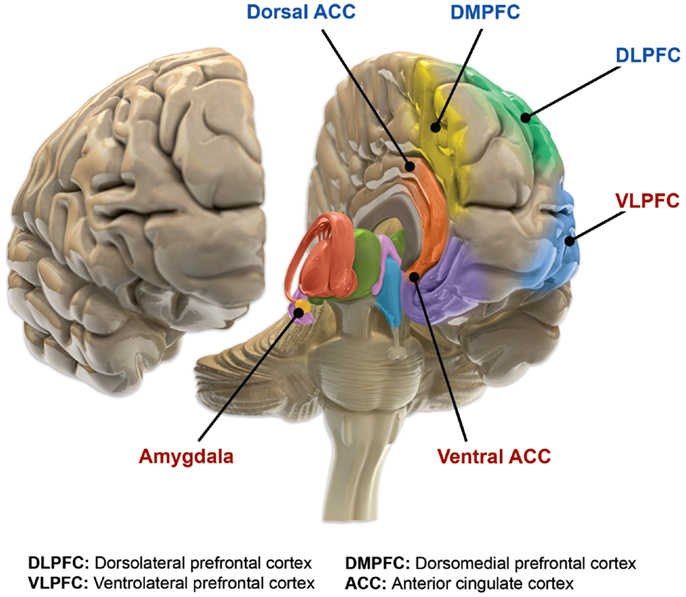

You must be logged in to post a comment.