

Certificate: Scotland’s Mental Health First Aid (SMHFA)
Myth:
Only a few people get mental illnesses and they are unusual or odd, so it is obvious who they are.
Fact:
Mental health problems are common and we are often unaware of the person’s diagnosis.
Myth:
People with a diagnosis of mental illness are going to struggle for the rest of their lives.
Fact:
Most people recover from mental illness and go on to live fulfilling lives. Recovery is a unique and personal journey and often the person feels that they experienced personal growth and a new way of being through the process of recovery.
Myth:
People who attempt suicide or self-harm are doing it to get attention and are not really serious.
Fact:
All suicidal thoughts and self-harm, as well as all other forms and expressions of distress, are serious. Dismissing another person’s feelings as attention seeking only makes them withdraw from asking for help and may result in death or serious injury.
Myth:
People who have mental illnesses have brought it upon themselves, or their parents are to blame.
Fact:
Anyone can experience mental illness or experience mental distress regardless of their background or upbringing. Some people are more at risk through circumstances beyond their own control.
Mental health problems are common and can affect anyone.
People with mental health problems do not lose their personality or intelligence, although the symptoms can sometimes change the way a person behaves when they are unwell.
People with mental health problems usually recover – there is a better chance of recovery from mental health problems than from some physical illnesses.
People with mental health problems want to work and to contribute to society, but it is often other people’s attitudes that prevent them from doing so.
Two thirds of employers, when asked, said that they did not feel comfortable employing a person with a mental health problem.
Many people with mental health problems continue to live life to the full, working and enjoying positive relationships and activities.
Sometimes, having a severe and enduring mental illness has a devastating effect on people’s live. With the right treatment and support, the person has a better chance of improvement and recovery.
People with schizophrenia do not have a split personality.
People with severe and enduring mental health problems are not usually dangerous – in fact, they are more likely to be victims of crime.
People with mental health problems are not weak and they do not bring the problems on themselves.
A growing body of evidence suggests that mental health problems cannot be separated from physical health, as the mind and body are closely interrelated.
Sometimes people dismiss others’ mental health problems or distress by judging them as weak. This is no more helpful or appropriate than judging someone for having a physical illness or disability.
Ordinary members of the public can help people experiencing mental health problems and make a real difference to their recovery.
There are many different ways of explaining mental health issues, and of explaining the factors that influence our health. Different models emphasise different aspects of mental health, such as the impact society and culture have on a person’s mental health.
It is important to note that there is more to mental health than whether or not a person has a diagnosis of an illness.
For the purposes of this website, I have selected the mental health continuum as a useful model to show that mental health changes over time and that mental health issues are about everyone (I learnt about the mental health continuum as part of the Scotland’s Mental Health First Aid course).
Other models of health and mental health are briefly described below.
Dahlgren and Whitehead Model
After the mental health continuum, another popular model to give an overview of one alternative way of considering health is the model by Dahlgren and Whitehead (1991).
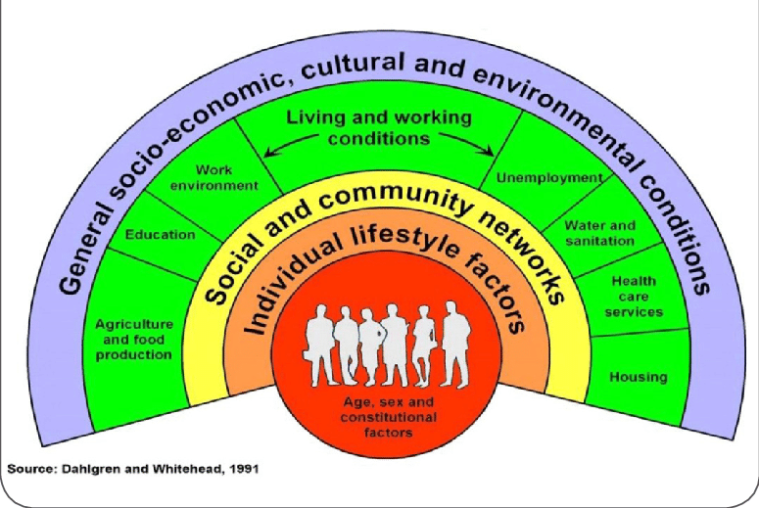
This model pays closer attention to the impact of lifestyle, social, economic circumstances, culture, and the environment. It attempts to show how these things influence an individual’s health and how they interact with one another.
The model shows that health is affected by a range of different factors, from those specific to the individual, to wider cultural and social issues.
An individual’s health will be influenced by their gender, age, by their individual personality, and relative strength or resilience. However, health is much more than individual factors. A person’s health is affected by their local community and the extent to which they have sense of belonging. Education, work, the ability to access and prepare healthy food, housing and sanitation are also significant factors, as are economic, cultural, and environmental conditions.
This model is useful for considering the extent to which a person has control over their own health, and how much health improvement needs to be driven by policy that recognises the impact of all these factors.
The model also acts as an important reminder that health is not purely about the individual. It is therefore unhelpful and misguided to blame those who are experiencing poor health.
Kinderman’s Psychological Model of Mental Disorder
A coherent conceptualisation of the role of psychological factors is of great importance in understanding mental disorder (Kinderman, 2005). Academic articles and professional reports alluding to psychological models of the aetiology of mental disorder are becoming increasingly common, and there is evidence of a marked policy shift toward the provision of psychological therapies and interventions.
This article discusses the relationship between biological, social, and psychological factors in the causation and treatment of mental disorder. It argues that simple biological reductionism is not scientifically justified, and also that the specific role of psychological processes within the biopsychosocial model requires further elaboration. The biopsychosocial model is usually interpreted as implying that biological, psychological, and social factors are co-equal partners in the aetiology of mental disorder.
The psychological model of mental disorder presented here suggests that disruption or dysfunction in psychological processes is a final common pathway in the development of mental disorder. These processes include, but are not limited to, cognitive processes.
The model proposes that biological and social factors, together with a person’s individual experiences, lead to mental disorder through their conjoint effects on those psychological processes. Implications for research, interventions, and policy are discussed.
The Biopsychosocial Model
The biopsychosocial approach was developed at Rochester decades ago by Dr’s. George Engel and John Romano, and published in 1977 (Engel, 1977; Frankel et al., 2003). While traditional biomedical models of clinical medicine focus on pathophysiology and other biological approaches to disease, the biopsychosocial approach emphasises the importance of understanding human health and illness in their fullest contexts. The biopsychosocial approach systematically considers biological, psychological, and social factors and their complex interactions in understanding health, illness, and health care delivery.
To apply the biopsychosocial approach to clinical practice, the clinician should (Engel, 1980):
Rethinking the Biopsychosocial Model of Health
In 2017, Lehman colleagues suggested that the biopsychosocial model had dominated research and theory in health psychology. Their 2017 article expanded the biopsychosocial model by applying systems theories proposed by developmental scholars, including Bronfenbrenner’s ecological models and Sameroff’s transactional model, as well as contemporary philosophical work on dynamic systems. The proposed dynamic biopsychosocial model construed human health as a product of the reciprocal influences of biological, psychological, interpersonal, and macrosystem contextual dynamics that unfold over personal and historical time. The importance, or centrality, of these influences varies within a person over time. The model is explicated using two hypothetical case studies derived from existing interdisciplinary health research. Implications for health, theory, research, and policy are discussed.
The Biomedical Model of Mental Disorder
Deacon (2013) states that the biomedical model posits that mental disorders are brain diseases and emphasises pharmacological treatment to target presumed biological abnormalities.
A biologically-focused approach to science, policy, and practice has dominated the American healthcare system for more than three decades. During this time, the use of psychiatric medications has sharply increased and mental disorders have become commonly regarded as brain diseases caused by chemical imbalances that are corrected with disease-specific drugs.
However, despite widespread faith in the potential of neuroscience to revolutionise mental health practice, the biomedical model era has been characterised by a broad lack of clinical innovation and poor mental health outcomes.
In addition, the biomedical paradigm has profoundly affected clinical psychology via the adoption of drug trial methodology in psychotherapy research. Although this approach has spurred the development of empirically supported psychological treatments for numerous mental disorders, it has neglected treatment process, inhibited treatment innovation and dissemination, and divided the field along scientist and practitioner lines.
The neglected biopsychosocial model represents an appealing alternative to the biomedical approach, and an honest and public dialog about the validity and utility of the biomedical paradigm is urgently needed.
References
Dahlgren, G. & Whitehead, M. (1991) Policies and Strategies to Promote Social Equality in Health. Stockholm: Institute for Future Studies.
Deacon, B.J. (2013) The Biomedical Model of Mental Disorder: A Critical Analysis of its Validity, Utility, and Effects on Psychotherapy Research. Clinical Psychology Review. 33, pp.846-861.
Engel, G.L. (1977) The Need for a New Medical Model: A Challenge for Biomedicine. Science. 196, pp.129-136.
Engel, G.L. (1980) The Clinical Application of the Biopsychosocial Model. American Journal of Psychiatry. 137, pp.535-544.
Frankel, R.M., Quill, T.E. & McDaniel, S.H. (Eds). (2003) The Biopsychosocial Approach: Past, Present, Future. Rochester, New York: University of Rochester Press.
Kinderman, P. (2005) A Psychological Model of Mental Disorder. Harvard Review of Psychiatry. 13(4), pp.206-217.
Lehman, B.J., David, D.M. & Gruber, J.A. (2017) Rethinking the Biopsycholosocial Model of Health: Understanding Health as a Dynamic System. Social and Personality Psychology Compass. 11(8).

Most people know that it is not appropriate to deliberately treat someone with mental health problems badly.
This awareness means that stigma is often expressed in less obvious ways, such as unkind jokes or ignoring a person.
Stigma and the fear of stigma is a serious issue that has an effect on people’s ability to cope with and recover from a mental health problem.
There is a lot of evidence to show that people are treated differently when they experience a mental health problem.
Stigma is based on myths and false assumptions about mental health problems.
Therefore, it is best addressed by gaining knowledge and an understanding of the facts.
Research has found that attitudes towards people with mental health problems have improved significantly in the United Kingdom (UK) since anti-stigma campaigns like ‘See Me’ were introduced.
We can make a difference to people’s mental health by gaining understanding and knowledge, and sharing it with others.
We can also make a difference by treating people with mental health problems as equals, and offering kindness and support when they are unwell.

The World Health Organisation (WHO) defines health as:
“…a state of (complete) physical, mental and social wellbeing and not merely the absence of disease or infirmity.”
Health is a positive concept that relates to every part of our lives. We cannot easily separate our physical and mental health, both of which can be influenced by other factors in our lives.
The term ‘mental health’ is often misunderstood. When asked about mental health people often assume it to be a negative term that means mental illness.
“Mental health means our ability to enjoy life and cope with its challenges. In a nutshell, are we able to get on and do the things we want to do? It’s not a by-word for ‘mental illness’. A mental illness is a problem that affects mental health (just like a broken leg affects physical health).”
Just as physical health refers to everything related to the health of our bodies, mental health refers to the health of our minds and emotions. Mental health influences how we think and feel about ourselves and about others, as well as how we respond to things that happen to us. It affects our work, learning, relationships, and the way we cope with ordinary life events such as moving house, having children or experiencing bereavement.
Mental health is about everyone. Our physical health changes over time and so does our mental health. Some days we feel better than other days, and at some times in our lives we experience more stress and distress than in others. Some of life’s most challenging events cause us to experience poor mental health, but over time we recover. All of this is normal, and all of it is about our mental health.
“Everyone has mental health needs, whether or not they have a diagnosis. These needs are met, or not met, at home, in families, at work, on the streets, in schools and neighbourhoods, in prisons and hospitals, where people feel respected, included and safe, or on the margins, in fear and excluded.”
Sometimes people develop more sever mental health problems that need professional treatment. When this happens it is a good idea to remember that the same thing happens in physical health. At times we develop an illness that requires medical or other treatment. In some cases there are things we can do to protect ourselves from getting a physical or mental illness. It can also happen for no obvious reason. Any one of us could become unwell in our lifetimes. In this website, you will find information about how people can care for their own mental health as well as how to respond if a person becomes very distressed or unwell.
If a person appears to be experiencing a mental health problem and is distressed it is important to get help as quickly as possible. Left untreated, some mental health problems will get worse, causing major changes to a person’s thinking, emotions, and behaviour. These changes can seriously disrupt the person’s work, home, and social life.
“Mental health is sometimes described as underpinning all health and wellbeing, because of growing research evidence of the impact of how people think and feel on their physical health.”

Mental health first aid (MHFA) is the first step in helping a person experiencing a mental health crisis, and is intended to be used until other help arrives.
Just like physical first aid, the first aim of MHFA is to preserve life.
Evidence shows that many people experiencing a mental health crisis have thoughts of suicide, and some people act on these thoughts. This is why asking about suicide is the first step in offering help.
The current model of MHFA is known by the five-step acronym A.L.G.E.E.
Step 1: Ask About Suicide
This does not mean that you should ask everyone you meet about suicide, regardless of their situation.
What it does mean is that when you suspect that a person may be having suicidal thoughts, because of their level of pain or distress, or because of their situation, or even because you have a gut feeling that they may be considering suicide, you should ask them.
This may seem very challenging and difficult to begin with, but the MHFA course covers the skills and practice that will make this step feel more natural.
Once we are sure that the person is not in immediate danger we can put the next step into practice.
Step 2: Listen and Communicate Non-Judgmentally
People who are feeling distressed or experiencing mental health problems can feel that no one is able to listen to them, or to accept their feelings without judging them as weak or inferior.
Being able to listen to the person, and offering them the simple human kindness of the time to talk about how they feel, can help them realise that they are not alone.
Step 3: Give Reassurance and Information
This is not about offering advice or solving the person’s problems. It is about reassuring them that there is effective help available and that there are things we can do immediately to help the situation.
Step 4: Encourage the Person to get Professional Help
This is essential to their recovery.
Help may be in the form of their general practitioner (GP), other support groups, or therapy.
The help they need will depend on the type of problem(s) they are experiencing.
The MHFA course provides you with the information on where different types of help can be found quickly.
Step 5: Encourage Self-Help Strategies
When a person is experiencing mental health problems, there are things that can be done in the short-term to alleviate their distress.
Similarly, when treatment is underway there are often things a person can do to help recovery.

The mental health first-aider must always put their own well-being and safety first. Taking care of one’s own health and safety can mean a variety of things depending on the situation.
Sometimes people are worried that being trained as a mental health first-aider will mean that they have to take responsibility for others even when this is too emotionally demanding or time consuming.
This is an understandable concern, but it is based on misconception.

People trained in mental health first aid (MHFA) are ordinary people who have been trained in what to do during a mental health crisis.
However, their role is only essential in the very short term, until other help can be found.
That other help can come in a variety of forms – from the person’s family or friends, a general practitioner (GP), a telephone helpline, a hospital accident and emergency department, or an ambulance.
A key thing to remember is that although the first-aider has been trained how to respond, they are never obliged to intervene.
There are many reasons for people to train in mental health first aid (MHFA).
Mental health problems are very common. As many as 1 in 4 people will experience mental health problems in any year. This means that most people know someone who has personal experience of mental health problems.

Currently, 1 in 20 people have depression. Around 80% of mental health problems are anxiety and depression. General practitioners (GP’s) are likely to diagnose 60% of mental health problems, and 90% of those will be treated by their GP’s. Almost 40% of absences from work are caused by mental health problems. Of all GP appointments, 70% will be patients with depression and anxiety.
Mental illness and distress has been a taboo subject in our society. This taboo is due to the stigma that surrounds mental health issues. In Western countries, people with mental health problems have been ridiculed or treated differently. For this reason, there is often a fear of speaking about such experiences.
Most people know very little about mental health. Good information and understanding about where to get effective help and treatment for mental health problems is invaluable when a crisis occurs, regardless of the setting. Receiving help or treatment early gives people the best possible chance of recovery.
Having people in the community who are comfortable talking about mental health issues, and who offer kindness, support and appropriate information, helps to reduce distress and promote recovery.
Many people are fearful of a diagnosis of a mental health problem, believing that receiving such a diagnosis will ruin their lives. This fear may cause people to hold back from asking for help when they most need it. Fears are kept alive by ignorance and a lack of understanding. Gaining more knowledge about mental health helps to ease fears and encourage recovery.
People from other countries and cultures who live and work in the United Kingdom (UK) may have very different ideas about mental health and find the National Health Service (NHS) and system confusing or difficult to access. For instance, Chinese medicine does not recognise the division between the mind and the body that is common in Western medicine. Therefore, a system that has separate care for mental and physical health may be difficult for a Chinese person to accept or feel confident using. Support that recognises and respects difference can help to bridge cultural differences and encourage understanding.
Professional help is not always immediately available. A ‘mental health first-aider’ can offer comfort and support in a crisis until help arrives.
In some instances, the person experiencing a mental health problem is not aware of the problem. Some illnesses cause the person’s thinking to be affected. In other cases, the person is so distressed that they do not know how to ask for help. Others may be aware that something is wrong, but may feel afraid of judgement or rejection. A mental health first-aider is trained to approach the person, offer assistance and to listen without judgement, enabling the person to say how they feel. The first-aider can then encourage the person to get appropriate help.
Knowing how to respond in a crisis is a key part of MHFA. It gives the first-aider confidence to know that they are offering effective help and not making things worse. MHFA is based on a five-step action plan that can be applied in any situation in which a person is experiencing mental health problems or distress.

You must be logged in to post a comment.