1990 – Bruno Bettelheim, Austrian-American psychologist and author (b. 1903).
Bruno Bettelheim
Bruno Bettelheim (28 August 1903 to 13 March 1990) was an Austrian-born psychologist, scholar, public intellectual and author who spent most of his academic and clinical career in the US. An early writer on autism, Bettelheim’s work focused on the education of emotionally disturbed children, as well as Freudian psychology more generally. In the US, he later gained a position as professor at the University of Chicago and director of the Sonia Shankman Orthogenic School for Disturbed Children, and after 1973 taught at Stanford University.
Bettelheim’s ideas, which grew out of those of Sigmund Freud, theorised that children with behavioural and emotional disorders were not born that way, and could be treated through extended psychoanalytic therapy, treatment that rejected the use of psychotropic drugs and shock therapy. During the 1960s and 1970s he had an international reputation in such fields as autism, child psychiatry, and psychoanalysis.
Much of his work was discredited after his death due to fraudulent academic credentials, allegations of patient abuse, accusations of plagiarism, and lack of oversight by institutions and the psychological community.
1864 – W.H.R. Rivers, English anthropologist, neurologist, ethnologist, and psychiatrist (d. 1922).
W.H.R. Rivers
William Halse Rivers Rivers FRS FRAI (12 March 1864 to 04 June 1922) was an English anthropologist, neurologist, ethnologist and psychiatrist, best known for his work treating First World War officers who were suffering from shell shock in order to return them to combat. Rivers’ most famous patient was the war poet Siegfried Sassoon, with whom he remained close friends until his own sudden death.
During the early years of the 20th century, Rivers developed many new lines of psychological research. In addition, he was the first to use a type of double-blind procedure in investigating physical and psychological effects of consumption of tea, coffee, alcohol, and drugs. For a time he directed centres for psychological studies at two colleges, and he was made a Fellow of St John’s College, Cambridge. He is also notable for having participated in the Torres Strait Islands expedition of 1898 and his consequent seminal work on the subject of kinship.
Light therapy – or phototherapy, classically referred to as heliotherapy – is a method recognised by scientific medicine for the treatment of various diseases. It includes exposure to outdoor daylight or specific indoor artificial light sources.
Example of light therapy for winter depression.
The care guideline for unipolar depression recommends light therapy especially for depression that follows a seasonal pattern (seasonal affective disorder). There is tentative evidence to support its use to treat depressive disorders that are not seasonally dependent. As a treatment for disorders of the skin, the second kind of light therapy, called ultraviolet light therapy, is meant to treat neurodermatitis, psoriasis, acne vulgaris, eczema and neonatal jaundice.
Brief History
Many ancient cultures practiced various forms of heliotherapy, including people of Ancient Greece, Ancient Egypt, and Ancient Rome. The Inca, Assyrian and early German settlers also worshipped the sun as a health bringing deity. Indian medical literature dating to 1500 BCE describes a treatment combining herbs with natural sunlight to treat non-pigmented skin areas. Buddhist literature from about 200 CE and 10th-century Chinese documents make similar references.
The Faroese physician Niels Finsen is believed to be the father of modern phototherapy. He developed the first artificial light source for this purpose. Finsen used short wavelength light to treat lupus vulgaris, a skin infection caused by Mycobacterium tuberculosis. He thought that the beneficial effect was due to ultraviolet light killing the bacteria, but recent studies showed that his lens and filter system did not allow such short wavelengths to pass through, leading instead to the conclusion that light of approximately 400 nanometers generated reactive oxygen that would kill the bacteria. Finsen also used red light to treat smallpox lesions. He received the Nobel Prize in Physiology or Medicine in 1903. Scientific evidence for some of his treatments is lacking, and later eradication of smallpox and development of antibiotics for tuberculosis rendered light therapy obsolete for these diseases.
From the late nineteenth century until the early 1930s, light therapy was considered an effective and mainstream medical therapy in the UK for conditions such as varicose ulcer, ‘sickly children’ and a wide range of other conditions. Controlled trials by the medical scientist Dora Colebrook, supported by the Medical Research Council, indicated that light therapy was not effective for such a wide range of conditions.
Medical Uses
Skin Conditions
Light therapy treatments for the skin usually involve exposure to ultraviolet light. The exposures can be to a small area of the skin or over the whole body surface, as in a tanning bed. The most common treatment is with narrowband UVB, which has a wavelength of approximately 311-313 nanometers. Exposure to photons (light) at these specific wavelengths enables the body to produce vitamin D. Full body phototherapy can be delivered at a doctor’s office or at home using a large high-power UVB booth. Tanning beds, however, generate mostly UVA light, and only 4% to 10% of tanning bed light is in the UVB spectrum.
Atopic Dermatitis
Light therapy is considered one of the best monotherapy treatments for atopic dermatitis (AD) when applied to patients who have not responded to traditional topical treatments. The therapy offers a wide range of options: UVA1 for acute AD, NB-UVB for chronic AD, and balneophototherapy have proven their efficacy. Patients tolerate the therapy safely but, as in any therapy, there are potential adverse effects and care must be taken in its application, particularly to children.
Psoriasis
For psoriasis, UVB phototherapy has been shown to be effective. A feature of psoriasis is localised inflammation mediated by the immune system. Ultraviolet radiation is known to suppress the immune system and reduce inflammatory responses. Light therapy for skin conditions like psoriasis usually use 313 nanometer UVB though it may use UVA (315-400 nm wavelength) or a broader spectrum UVB (280-315 nm wavelength). UVA combined with psoralen, a drug taken orally, is known as PUVA treatment. In UVB phototherapy the exposure time is very short, seconds to minutes depending on intensity of lamps and the person’s skin pigment and sensitivity.
Vitiligo
About 1% of the human population suffers from vitiligo which causes painless distinct light-coloured patches of the skin on the face, hands, and legs. Phototherapy is an effective treatment because it forces skin cells to manufacture melanin to protect the body from UV damage. Prescribed treatment is generally 3 times a week in a clinic or daily at home. About 1 month usually results in re-pigmentation in the face and neck, and 2-4 months in the hands and legs. Narrowband UVB is more suitable to the face and neck and PUVA is more effective at the hands and legs.]
Acne Vulgaris
As of 2012 evidence for light therapy and lasers in the treatment of acne vulgaris was not sufficient to recommend them. There is moderate evidence for the efficacy of blue and blue-red light therapies in treating mild acne, but most studies are of low quality. While light therapy appears to provide short-term benefit, there is a lack of long-term outcome data or data in those with severe acne.
Cancer
According to the American Cancer Society, there is some evidence that ultraviolet light therapy may be effective in helping treat certain kinds of skin cancer, and ultraviolet blood irradiation therapy is established for this application. However, alternative uses of light for cancer treatment – light box therapy and coloured light therapy – are not supported by evidence. Photodynamic therapy (often with red light) is used to treat certain superficial non-melanoma skin cancers.
Other Skin Conditions
Some types of phototherapy may be effective in the treatment of polymorphous light eruption, cutaneous T-cell lymphoma and lichen planus. Narrowband UVB between 311-313 nanometers is the most common treatment.
Wound Healing
Low level laser therapy has been studied as a potential treatment for chronic wounds, and higher-power lasers have sometimes been successfully used to close acute wounds as an alternative to stitching. However, as of 2012 and due to inconsistent results and the low quality of extant research, reviews in the scientific literature have not supported its widespread application.
Retinal Conditions
There is preliminary evidence that light therapy is an effective treatment for diabetic retinopathy and diabetic macular oedema.
Mood and Sleep Related
Seasonal Affective Disorder
The effectiveness of light therapy for treating seasonal affective disorder (SAD) may be linked to the fact that light therapy makes up for lost sunlight exposure and resets the body’s internal clock. Studies show that light therapy helps reduce the debilitating and depressive behaviours of SAD, such as excessive sleepiness and fatigue, with results lasting for at least 1 month. Light therapy is preferred over antidepressants in the treatment of SAD because it is a relatively safe and easy therapy. Two methods of light therapy, bright light and dawn simulation, have similar success rates in the treatment of SAD.
It is possible that response to light therapy for SAD could be season dependent. Morning therapy has provided the best results because light in the early morning aids in regulating the circadian rhythm. People affected by SAD have low levels of energy and have difficulty concentrating. They usually have a change in appetite and experience trouble sleeping.
A 2007 systematic review by the Swedish agency SBU found insufficient evidence that light therapy was able to alleviate symptoms of depression or seasonal affective disorder. The report recommended that: “Approximately 100 participants are required to establish whether the therapy is moderately more effective than placebo”. Although treatment in light therapy rooms was well established in Sweden, no satisfactory, controlled studies had been published on the subject. This led to the closure of a number of clinics offering light therapy in Sweden.
A Cochrane review conducted in 2019 states the evidence that light therapy’s effectiveness as a treatment for the prevention of seasonal affective disorder is limited, although the risk of adverse effects are minimal. Therefore, the decision to use light therapy should be based on a person’s preference of treatment.
Non-Seasonal Depression
Light therapy has also been suggested in the treatment of non-seasonal depression and other psychiatric mood disturbances, including major depressive disorder, bipolar disorder and postpartum depression. A meta-analysis by the Cochrane Collaboration concluded that “for patients suffering from non-seasonal depression, light therapy offers modest though promising antidepressive efficacy.” A 2008 systematic review concluded that “overall, bright light therapy is an excellent candidate for inclusion into the therapeutic inventory available for the treatment of nonseasonal depression today, as adjuvant therapy to antidepressant medication, or eventually as stand-alone treatment for specific subgroups of depressed patients.” A 2015 review found that supporting evidence for light therapy was limited due to serious methodological flaws.
A 2016 meta-analysis showed that bright light therapy appeared to be efficacious, particularly when administered for 2-5 weeks’ duration and as monotherapy.
Chronic Circadian Rhythm Sleep Disorders (CRSD)
In the management of circadian rhythm disorders such as delayed sleep phase disorder (DSPD), the timing of light exposure is critical. Light exposure administered to the eyes before or after the nadir of the core body temperature rhythm can affect the phase response curve. Use upon awakening may also be effective for non-24-hour sleep-wake disorder. Some users have reported success with lights that turn on shortly before awakening (dawn simulation). Evening use is recommended for people with advanced sleep phase disorder. Some, but not all, totally blind people whose retinae are intact, may benefit from light therapy.
Light therapy has been tested for individuals with shift work sleep disorder and for jet lag.
Sleep Disorder in Parkinson’s Disease
Light therapy has been trialled in treating sleep disorders experienced by patients with Parkinson’s disease.
Sleep Disorder in Alzheimer’s Disease
Studies have shown that daytime and evening light therapy for nursing home patients with Alzheimer’s disease, who often struggle with agitation and fragmented wake/rest cycles effectively led to more consolidated sleep and an increase in circadian rhythm stability.
Neonatal Jaundice (Postnatal Jaundice)
Light therapy is used to treat cases of neonatal jaundice. Bilirubin, a yellow pigment normally formed in the liver during the breakdown of old red blood cells, cannot always be effectively cleared by a neonate’s liver causing neonatal jaundice. Accumulation of excess bilirubin can cause central nervous system damage, and so this buildup of bilirubin must be treated. Phototherapy uses the energy from light to isomerize the bilirubin and consequently transform it into compounds that the newborn can excrete via urine and stools. Bilirubin is most successful absorbing light in the blue region of the visible light spectrum, which falls between 460-490 nm. Therefore light therapy technologies that utilise these blue wavelengths are the most successful at isomerising bilirubin.
Techniques
Photodynamic Therapy
Photodynamic therapy is a form of phototherapy using nontoxic light-sensitive compounds that are exposed selectively to light, whereupon they become toxic to targeted malignant and other diseased cells.
One of the treatments is using blue light with aminolevulinic acid for the treatment of actinic keratosis. This is not a U.S. FDA-approved treatment for acne vulgaris.
Light Boxes
The production of the hormone melatonin, a sleep regulator, is inhibited by light and permitted by darkness as registered by photosensitive ganglion cells in the retina. To some degree, the reverse is true for serotonin, which has been linked to mood disorders. Hence, for the purpose of manipulating melatonin levels or timing, light boxes providing very specific types of artificial illumination to the retina of the eye are effective.
Light therapy uses either a light box which emits up to 10,000 lux of light at a specified distance, much brighter than a customary lamp, or a lower intensity of specific wavelengths of light from the blue (460 nm) to the green (525 nm) areas of the visible spectrum. A 1995 study showed that green light therapy at doses of 350 lux produces melatonin suppression and phase shifts equivalent to 10,000 lux white light therapy, but another study published in May 2010 suggests that the blue light often used for SAD treatment should perhaps be replaced by green or white illumination, because of a possible involvement of the cones in melatonin suppression.
Child patients with external forms of tuberculosis, especially of the bones and joints, laying on beds on a terrace outside Treloar Hospital in Alton, Hampshire, England, in sunlight as part of their light therapy, ca. first half of the 20th century.
Risks and Complications
Ultraviolet
Ultraviolet light causes progressive damage to human skin and erythema even from small doses. This is mediated by genetic damage, collagen damage, as well as destruction of vitamin A and vitamin C in the skin and free radical generation. Ultraviolet light is also known to be a factor in formation of cataracts. Ultraviolet radiation exposure is strongly linked to incidence of skin cancer.
Visible Light
Optical radiation of any kind with enough intensity can cause damage to the eyes and skin including photoconjunctivitis and photokeratitis. Researchers have questioned whether limiting blue light exposure could reduce the risk of age-related macular degeneration. According to the American Academy of Ophthalmology, there is no scientific evidence showing that exposure to blue light emitting devices result in eye damage. According to Harriet Hall, blue light exposure is reported to suppress the production of melatonin, which affects our body’s circadian rhythm and can decrease sleep quality. It is reported that bright light therapy may activate the production of reproductive hormones, such as testosterone, luteinizing hormone, follicle-stimulating hormone, and estradiol.
Modern phototherapy lamps used in the treatment of seasonal affective disorder and sleep disorders either filter out or do not emit ultraviolet light and are considered safe and effective for the intended purpose, as long as photosensitising drugs are not being taken at the same time and in the absence of any existing eye conditions. Light therapy is a mood altering treatment, and just as with drug treatments, there is a possibility of triggering a manic state from a depressive state, causing anxiety and other side effects. While these side effects are usually controllable, it is recommended that patients undertake light therapy under the supervision of an experienced clinician, rather than attempting to self-medicate.
Contraindications to light therapy for seasonal affective disorder include conditions that might render the eyes more vulnerable to phototoxicity, tendency toward mania, photosensitive skin conditions, or use of a photosensitising herb (such as St. John’s wort) or medication. Patients with porphyria should avoid most forms of light therapy. Patients on certain drugs such as methotrexate or chloroquine should use caution with light therapy as there is a chance that these drugs could cause porphyria.
Side effects of light therapy for sleep phase disorders include jumpiness or jitteriness, headache, eye irritation and nausea. Some non-depressive physical complaints, such as poor vision and skin rash or irritation, may improve with light therapy.
1915 – J.C.R. Licklider, American computer scientist and psychologist (d. 1990).
People (Deaths)
1999 – Herbert Jasper, Canadian psychologist, anatomist, and neurologist (b. 1906).
1999 – Camille Laurin, Canadian psychiatrist and politician (b. 1922).
J.C.R. Licklider
Joseph Carl Robnett Licklider (11 March 1915 to 26 June 1990), known simply as J.C.R. or “Lick”, was an American psychologist and computer scientist who is considered among prominent figures in computer science development and general computing history.
He is particularly remembered for being one of the first to foresee modern-style interactive computing and its application to all manner of activities; and also as an Internet pioneer with an early vision of a worldwide computer network long before it was built. He did much to initiate this by funding research which led to much of it, including today’s canonical graphical user interface, and the ARPANET, the direct predecessor to the Internet.
He has been called “computing’s Johnny Appleseed”, for planting the seeds of computing in the digital age; Robert Taylor, founder of Xerox PARC’s Computer Science Laboratory and Digital Equipment Corporation’s Systems Research Center, noted that “most of the significant advances in computer technology – including the work that my group did at Xerox PARC – were simply extrapolations of Lick’s vision. They were not really new visions of their own. So he was really the father of it all”.
Herbert Jasper
Herbert Henri Jasper OC GOQ FRSC (27 July 1906 to 11 March 1999) was a Canadian psychologist, physiologist, neurologist, and epileptologist (neurologist who specialises in the treatment of epilepsy).
Born in La Grande, Oregon, he attended Reed College in Portland, Oregon and received his PhD in psychology from the University of Iowa in 1931 and earned a Doctor of Science degree from the University of Paris for research in neurobiology.
From 1946 to 1964 he was Professor of Experimental Neurology at the Montreal Neurological Institute, McGill University and then from 1965 to 1976 he was Professor of Neurophysiology, Université de Montréal. He did his most important research with Wilder Penfield at McGill University. He was a member of the American Academy of Neurology and the American Association for the Advancement of Science. He was also a member of the Canadian Neurological Society and the Royal Society of Medicine. He wrote more than 350 scientific publications.
Camille Laurin
Camille Laurin (06 May 1922 to 11 March 1999) was a psychiatrist and Parti Québécois (PQ) politician in the Canadian province of Quebec. A MNA member for the riding of Bourget, he is considered the father of Quebec’s language law known informally as “Bill 101”.
Obtained a degree in psychiatry from the Université de Montréal.
In clinical and abnormal psychology, institutionalisation or institutional syndrome refers to deficits or disabilities in social and life skills, which develop after a person has spent a long period living in psychiatric hospitals, prisons or other remote institutions.
In other words, individuals in institutions may be deprived (whether unintentionally or not) of independence and of responsibility, to the point that once they return to “outside life” they are often unable to manage many of its demands; it has also been argued that institutionalised individuals become psychologically more prone to mental health problems.
The term institutionalisation can also be used to describe the process of committing an individual to a mental hospital or prison, or to describe institutional syndrome; thus the phrase “X is institutionalised” may mean either that X has been placed in an institution or that X is suffering the psychological effects of having been in an institution for an extended period of time.
Background
In Europe and North America, the trend of putting the mentally ill into mental hospitals began as early as the 17th century, and hospitals often focused more on “restraining” or controlling inmates than on curing them, although hospital conditions improved somewhat with movements for human treatment, such as moral management. By the mid-20th century, overcrowding in institutions, the failure of institutional treatment to cure most mental illnesses, and the advent of drugs such as Thorazine prompted many hospitals to begin discharging patients in large numbers, in the beginning of the deinstitutionalisation movement (the process of gradually moving people from inpatient care in mental hospitals, to outpatient care).
Deinstitutionalisation did not always result in better treatment, however, and in many ways it helped reveal some of the shortcomings of institutional care, as discharged patients were often unable to take care of themselves, and many ended up homeless or in jail. In other words, many of these patients had become “institutionalised” and were unable to adjust to independent living. One of the first studies to address the issue of institutionalisation directly was British psychiatrist Russell Barton’s 1959 book Institutional Neurosis, which claimed that many symptoms of mental illness (specifically, psychosis) were not physical brain defects as once thought, but were consequences of institutions’ “stripping” (a term probably first used in this context by Erving Goffman) away the “psychological crutches” of their patients.
Since the middle of the 20th century, the problem of institutionalisation has been one of the motivating factors for the increasing popularity of deinstitutionalisation and the growth of community mental health services, since some mental healthcare providers believe that institutional care may create as many problems as it solves.
Romanian children who suffered from severe neglect at a young age were adopted by families. Research reveals that the post-institutional syndrome occurring in these children gave rise to symptoms of autistic behaviour. Studies done on eight Romanian adoptees living in the Netherlands revealed that about one third of the children exhibited behavioural and communication problems resembling that of autism.
Issues for Discharged Patients
Individuals who suffer from institutional syndrome can face several kinds of difficulties upon returning to the community. The lack of independence and responsibility for patients within institutions, along with the ‘depressing’ and ‘dehumanising’ environment, can make it difficult for patients to live and work independently. Furthermore, the experience of being in an institution may often have exacerbated individuals’ illness: proponents of labelling theory claim that individuals who are socially “labelled” as mentally ill suffer stigmatisation and alienation that lead to psychological damage and a lessening of self-esteem, and thus that being placed in a mental health institution can actually cause individuals to become more mentally ill.
Infantilisation is the prolonged treatment of one who has a mental capacity greater than that of a child as though they are a child.
Background
When used in reference to teenagers or adolescents, the term typically suggests that teenagers and their potential are underestimated in modern society, and/or that adolescents are often regarded as though they are younger than their actual age.
Studies have shown that an individual, when infantilised, is overwhelmingly likely to feel disrespected. Such individuals may report a sense of transgression akin to dehumanisation.
There can be an overlap between the terms “infantilisation” and “patronisation”, although infantilisation derives more specifically from a sense of age group or hierarchical seniority on the part of those responsible for infantilisation. The act of infantilising others has been associated with narcissists.
Infantilisation may also refer to a process when a child is being treated in a manner appropriate only for younger children.
In property law, infantilisation is defined as “the restriction of an individual’s or group’s autonomy based on the failure to recognize and respect their full capacity to reason.” When infantilisation is coupled with property takeover, the result is a dignity taking.
There are several examples of dignity takings, including wage theft from undocumented workers where the power imbalance allows employers to rob workers of their agency and avenues for redress; the dispossession of property from African Americans in the South Carolina sea islands by predatory tax buyers who routinely infantilised their victims by overwhelming them with paperwork and timelines to accelerate foreclosures; and the unequal division of matrimonial property in southern Nigeria following divorce that assumes women are less capable of managing property and thus infantilises them.
Historical trauma (HT), as used by social workers, historians, and psychologists, refers to the cumulative emotional harm of an individual or generation caused by a traumatic experience or event. Historical Trauma Response (HTR) refers to the manifestation of emotions and actions that stem from this perceived trauma.
According to its advocates, HTR is exhibited in a variety of ways, most prominently through substance abuse, which is used as a vehicle for attempting to numb pain. This model seeks to use this to explain other self-destructive behaviour, such as suicidal thoughts and gestures, depression, anxiety, low self-esteem, anger, violence and difficulty recognising and expressing emotions. Many historians and scholars believe the manifestations of violence and abuse in certain communities are directly associated with the unresolved grief that accompanies continued trauma.
Historical trauma, and its manifestations, are seen as an example of Transgenerational trauma (though the existence of transgenerational trauma itself is disputed). For example, a pattern of maternal abandonment of a child might be seen across three generations, or the actions of an abusive parent might be seen in continued abuse across generations. These manifestations can also stem from the trauma of events, such as the witnessing of war, genocide, or death. For these populations that have witnessed these mass level traumas (e.g. war, genocide, colonialism), several generations later these populations tend to have higher rates of disease.
Maria Yellow Horse Brave Heart first developed the concept of historical trauma while working with Lakota communities in the 1980s. Since then, many other researchers have developed the concept and applied it to other populations, such as African Americans and Holocaust survivors.
Brief History of Research
First used by social worker and mental health expert Maria Yellow Horse Brave Heart in the 1980s, scholarship surrounding historical trauma has expanded to fields outside of the Lakota communities Yellow Horse Brave Heart studied. Yellow Horse Brave Heart’s scholarship focused on the ways in which the psychological and emotional traumas of colonisation, relocation, assimilation, and American Indian boarding schools have manifested within generations of the Lakota population. Yellow Horse Brave Heart’s article “Wakiksuyapi: Carrying the Historical Trauma of the Lakota,” published in 2000, compares the effects and manifestations of historical trauma on Holocaust survivors and Native American peoples. Her scholarship concluded that the manifestations of trauma, although produced by different events and actions, are exhibited in similar ways within each afflicted community.
Other significant original research on the mechanisms and transmission of intergenerational trauma has been done by scholars such as Daniel Schechter, whose work builds on the pioneers in this field such as: Judith Kestenberg, Dori Laub, Selma Fraiberg, Alicia Lieberman, Susan Coates, Charles Zeanah, Karlen Lyons-Ruth, Yael Danieli, Rachel Yehuda and others. Although each scholar focuses on a different population – such as Native Americans, African Americans, or Holocaust Survivors – all have concluded that the mechanism and transmission of intergenerational trauma is abundant within communities that experience traumatic events. Daniel Schechter’s work has included the study of experimental interventions that may lead to changes in trauma-associated mental representation and may help in the stopping of intergenerational cycles of violence.
Joy DeGruy’s book, Post Traumatic Slave Syndrome, analyses the manifestation of historical trauma in African-American populations, and its correlation to the lingering effects of slavery. In 2018, Dodging Bullets – Stories from Survivors of Historical Trauma, the first documentary film to chronicle historical trauma in Indian Country, was released. It included interviews with scientist Rachel Yehuda, sociologist Melissa Walls, and Anton Treuer along with first hand testimonies of Dakota, Lakota, Ojibwe and Blackfeet tribal members.
Indigenous Historical Trauma
Maria Yellow Horse Brave Heart first coined the term Indigenous Historical Trauma (IHT) in the 1990s, to characterise the psycho-social legacy of European colonisation in North American Indigenous communities. The broader concept of Historical Trauma was developed from this, and gained footing in the clinical and health science literatures in the first two decades of the 21st century. In 2019, a team of psychologists at the University of Michigan published a systematic review of the literature so far on the relationship between IHT and adverse health outcomes for Indigenous peoples in the United States and Canada.
An example of IHT is the ”Indian boarding schools” created in the 19th century to acculturate Native Americans to European culture. According to one of their advocates Richard Henry Pratt, the intention of these schools was to literally “kill the indian” in the student, “and save the man”. These schools attempted to strip children of their cultural identity by practices such as cutting off their long hair, or forbidding them to speak their native language. After the school year was over, some indigenous children were hired to work for “non-Indian families” and many did not return home to their families.
The fear and loneliness caused by such schools can be readily imagined. But scientific research has consistently found that the stress caused by Indian boarding schools resulted in depression, sexual abuse, and suicidality. Descendants of boarding school survivors may carry this historical trauma for generations, and in the present day, Native American students still face challenges related to their lack of awareness of “psychological injury or harm from ancestral experiences with colonial violence and oppression”. Indeed, people who are unaware of the traumatic experiences their ancestors endured may find themselves involved in continued patterns of substance abuse, violence, physical abuse, verbal abuse, and suicide attempts.
Therefore, the term IHT can be useful to explain emotions and other psychological phenomena experienced by Native Americans today. Identifying IHT helps with recognising the “psychological distress and health disparities” linked to current Indigenous communities.
Manifestation
HT, or HTR, can manifest itself in a variety of psychological ways. However, it is most commonly seen through high rates of substance abuse, alcoholism, depression, anxiety, suicide, domestic violence, and abuse within afflicted communities. The effects and manifestations of trauma are extremely important in understanding the present-day conditions of afflicted populations.
Within Native American communities, high rates of alcoholism and suicide have direct correlation to the violence, mistreatment, and abuses experienced at boarding schools, and the loss of cultural heritage and identity these institutions facilitated. Although many present-day children never experienced these schools first-hand, the “injuries inflicted at Indian boarding schools are continuous and ongoing,” affecting generations of Native peoples and communities.
Countries like Australia and Canada have issued formal apologies for their involvement in the creation and implementation of boarding schools that facilitated and perpetuated historical trauma. Australia’s Bringing Them Home report and Canada’s Truth and Reconciliation Commission (Canada) both detailed the “experiences, impacts, and consequences” of government-sponsored boarding schools on Indigenous communities and children. Both reports also detail the problems facing Indigenous populations today, such as economic and health disparities, and their connection to the historical trauma of colonisation, removal, and forced assimilation.
Author and teacher Thomas Hübl, documenting his experiences working with Germans and Israelis to engage in dialogue around their shared historical and intergenerational trauma, writes:
Whether we refer to a person as victim or victimiser, oppressor or oppressed, it appears that no one, given time, remains untouched by collective suffering. Historical traumas impart their consequences indiscriminately upon child and family, institution and society, custom and culture, value and belief. Collective traumas distort social narratives, rupture national identities, and hinder the development of institutions, communities, and cultures, just as personally experienced trauma has the power to disrupt the psychological development of a growing child.
Treatment
Treatment of HT must repair the afflicted person or communities’ connection with their culture, values, beliefs, and self-image. It takes the forms of individual counselling or therapy, spiritual help, and group or entire community gatherings, which are all important aspects in the foundations of the healing process. Treatment should be aimed at a renewal of destroyed culture, spiritual beliefs, customs, and family connections, and a focus on reaffirming one’s self-image and place within a community. Cultural revitalisation initiatives for treating historical trauma among Native groups in North America include “culture camps,” where individuals live or camp out on their tribe’s traditional lands in order to learn cultural practices that have been lost to them as a result of colonial practices.
Due to the collective and identity-based nature of HT, treatment approaches should be more than solutions to one individual’s problems. Healing must also entail revitalisation of practices and ways of being that are necessary not just for individuals but for the communities they exist within. Relieving personal distress and promoting individual coping are important treatment goals, but successful treatment of HT also depends upon community-wide efforts to ending intergenerational transmission of collective trauma.
Particular attention should be given to the needs and empowerment of peoples who are vulnerable, oppressed, and living in poverty. Social workers and activists should promote social justice and social change with and on behalf of clients, individuals, families, groups, and communities. In order for advocacy to be accurate and helpful to the afflicted populations, social workers should understand the cultural diversity, history, culture, and contemporary realities of clients.
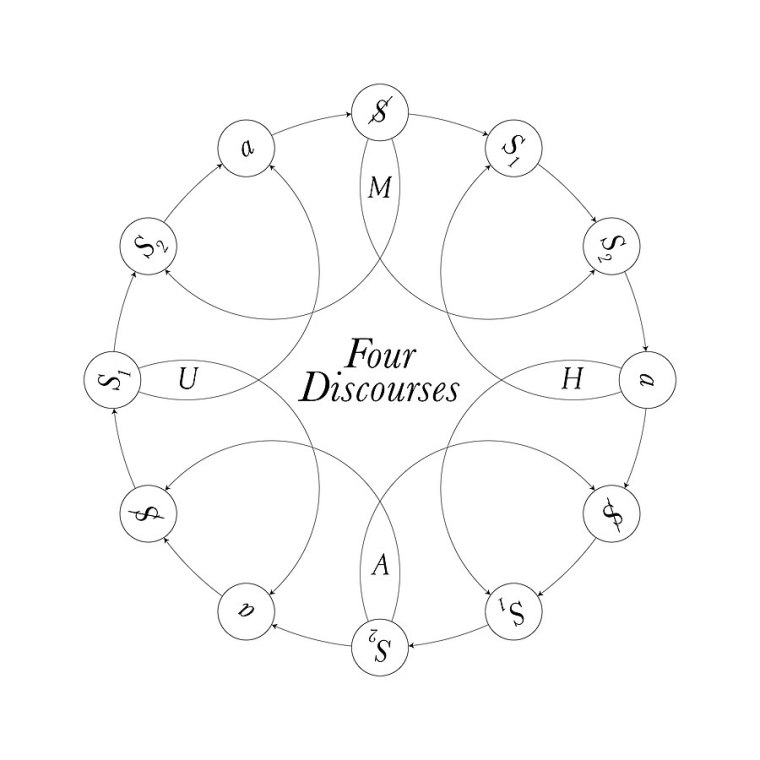
Four discourses is a concept developed by French psychoanalyst Jacques Lacan. He argued that there were four fundamental types of discourse. He defined four discourses, which he called Master, University, Hysteric and Analyst, and suggested that these relate dynamically to one another.
Diagram depicting all four discourses as a single system.
Lacan’s theory of the four discourses was initially developed in 1969, perhaps in response to the events of social unrest during May 1968 in France, but also through his discovery of what he believed were deficiencies in the orthodox reading of the Oedipus complex. The four discourses theory is presented in his seminar L’envers de la psychanalyse and in Radiophonie, where he starts using “discourse” as a social bond founded in intersubjectivity. He uses the term discourse to stress the transindividual nature of language: speech always implies another subject.
Necessity of Formalising Psychoanalysis
Prior to the development of the four discourses, the primary guideline for clinical psychoanalysis was Freud‘s Oedipus complex. In Lacan’s Seminar of 1969-1970, Lacan argues that the terrifying Oedipal father that Freud invoked was already castrated at the point of intervention. The castration was symbolic rather than physical. In an effort to stem analysts’ tendency to project their own imaginary readings and neurotic fantasies onto psychoanalysis, Lacan worked to formalise psychoanalytic theory with mathematical functions with renewed focus on the semiology of Ferdinand de Saussure. This would ensure only a minimum of teaching is lost when communicated and also provide the conceptual architecture to limit the associations of the analyst.
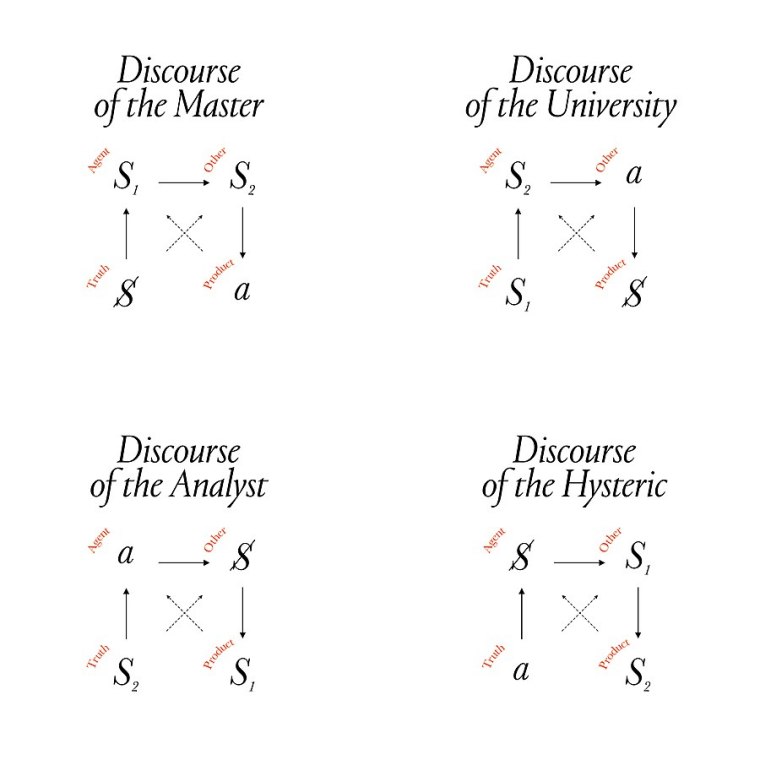
Four Discourses depicted side by side.
Structure
Discourse, in the first place, refers to a point where speech and language intersect. The four discourses represent the four possible formulations of the symbolic network which social bonds can take and can be expressed as the permutations of a four-term configuration showing the relative positions – the agent, the other, the product and the truth – of four terms, the subject, the master signifier, knowledge and objet petit a.
Positions
Agent (upper left), the speaker of the discourse.
Other (upper right), what the discourse is addressed to.
Product (lower right), what the discourse has created.
Truth (lower left), what the discourse attempted to express.
Variables
Variable
Description
S1
The dominant, ordering and sense giving signifier of a discourse as it is received by the group, community or culture. S1 refers to “the marked circle of the field of the Other,” it is the Master-Signifier. S1 comes into play in a signifying battery conforming the network of knowledge.
S2
What is ordered by or set in motion by S1. It is knowledge, the existing body of knowledge, the knowledge of the time. S2 is the “battery of signifiers, already there” at the place where “one wants to determine the status of a discourse as status of statement,” that is knowledge (savoir).
$
The subject, or person, for Lacan is always barred in the sense that it is incomplete, divided. Just as we can never know the world around us except in the partial refractions of language and the domination of identification, so, too, we can never know ourselves. $ is the subject, marked by the unbroken line (trait unaire) which represents it and is different from the living individual who is not the locus of this subject.
a
The objet petit a or surplus-jouissance. In Lacan’s psychoanalytic theory, objet petit a stands for the unattainable object of desire. It is sometimes called the object cause of desire. Lacan always insisted that the term should remain untranslated, “thus acquiring the status of an algebraic sign”. It is the object-waste or the loss of the object that occurred when the original division of the subject took place—the object that is the cause of desire: the plus-de-jouir.
Four Discourses
Discourse of the Master
We see a barred subject ($) positioned as master signifier’s truth, who’s itself positioned as discourse’s agent for all other signifiers (S2), that illustrates the structure of the dialectic of the master and the slave. The master, (S1) is the agent that puts the other, (S2) to work: the product is a surplus, objet a, that master struggles to appropriate alone. In a modern society, an example of this discourse can be found within so-called “family-like” work environments that tend to hide direct subordination under the mask of “favorable” submission to master’s truth that generates value. The Master’s reach for the truth in principle is fulfilment of his/her castratedness through subject’s work. Based on Hegel’s master–slave dialectic.
Discourse of the University
Knowledge in position of an agent is handed down by the institute which legitimises the master signifier (S1) and knowledge is positioned in the place of discourse’s truth. Impossibility to satisfy one’s need with a knowledge (which is a structural thing) produces a barred subject ($) as discourses sustain, and the cycle repeats itself through the primary subject being slavish to the institution values to fulfil the castratedness. The discourse’s truth “knowledge ” is being positioned aside of this loop and never the direct object of the subject, and the institute controls the subjects’ objet a and defines the subject’s master signifier’s. Pathological symptom of an agent in this discourse is seeking fulfilment of their castratedness through enjoying the castratedness of their subject.
Discourse of the Analyst
The position of an agent – the analyst – is occupied by objet a of the analysand. Analyst’s silence leads to reverse hysterisation, as such the analyst becomes a mirror of question himself to the analysand, thus embodies barred subject’s desire that lets his symptom speak itself through speech and thus be interpreted by the analyst. The master signifier of the analysand emerges as a product of this role. Hidden knowledge, positioned as discourse’s truth (S2) stands for both analyst interpretation technique and knowledge acquired from the subject.
Discourse of the Hysteric
Despite its pathological aura, hysteric’s discourse exhibits the most common mode of speech, blurring the line between clinical image and the otherness of social settings. Object a truth is defined by interrogative nature of subject’s address (Who am I?) as well as tryst for satisfaction of knowledge. This mutually drives the barred subject and turns on the agent’s master signifiers. It leads the agent to produce a new knowledge (discourse’s product) in a futile attempt to provide a barred subject with an answer to fulfil subject’s castratedness (Lacan in Discourse of the Analyst breaks the pathological cycle of it by purposefully leaving the question unanswered, reversing the discourse and putting an analyst in a place of hysteric’s desire). However, object a of the subject is search for the agent’s object a, thus without being a subject like in the ‘Discourse of the University’ the Hysteric ends up gathering knowledge instead of their object a truth.
Relevance for Cultural Studies
Slavoj Žižek uses the theory to explain various cultural artefacts, including Don Giovanni and Parsifal.
Functional fixedness is a cognitive bias that limits a person to use an object only in the way it is traditionally used.
The concept of functional fixedness originated in Gestalt psychology, a movement in psychology that emphasizes holistic processing. Karl Duncker defined functional fixedness as being a mental block against using an object in a new way that is required to solve a problem. This “block” limits the ability of an individual to use components given to them to complete a task, as they cannot move past the original purpose of those components. For example, if someone needs a paperweight, but they only have a hammer, they may not see how the hammer can be used as a paperweight. Functional fixedness is this inability to see a hammer’s use as anything other than for pounding nails; the person couldn’t think to use the hammer in a way other than in its conventional function.
When tested, 5-year-old children show no signs of functional fixedness. It has been argued that this is because at age 5, any goal to be achieved with an object is equivalent to any other goal. However, by age 7, children have acquired the tendency to treat the originally intended purpose of an object as special.
Examples in Research
Experimental paradigms typically involve solving problems in novel situations in which the subject has the use of a familiar object in an unfamiliar context. The object may be familiar from the subject’s past experience or from previous tasks within an experiment.
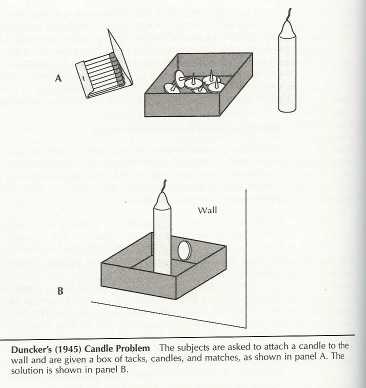
Candle Box
In a classic experiment demonstrating functional fixedness, Duncker (1945) gave participants a candle, a box of thumbtacks, and a book of matches, and asked them to attach the candle to the wall so that it did not drip onto the table below. Duncker found that participants tried to attach the candle directly to the wall with the tacks, or to glue it to the wall by melting it. Very few of them thought of using the inside of the box as a candle-holder and tacking this to the wall. In Duncker’s terms, the participants were “fixated” on the box’s normal function of holding thumbtacks and could not re-conceptualize it in a manner that allowed them to solve the problem. For instance, participants presented with an empty tack box were two times more likely to solve the problem than those presented with the tack box used as a container.
Candle box problem diagram.
More recently, Frank and Ramscar (2003) gave a written version of the candle problem to undergraduates at Stanford University. When the problem was given with identical instructions to those in the original experiment, only 23% of the students were able to solve the problem. For another group of students, the noun phrases such as “box of matches” were underlined, and for a third group, the nouns (e.g. “box”) were underlined. For these two groups, 55% and 47% were able to solve the problem effectively. In a follow-up experiment, all the nouns except “box” were underlined and similar results were produced. The authors concluded that students’ performance was contingent on their representation of the lexical concept “box” rather than instructional manipulations. The ability to overcome functional fixedness was contingent on having a flexible representation of the word box which allows students to see that the box can be used when attaching a candle to a wall.
When Adamson (1952) replicated Duncker’s box experiment, Adamson split participants into 2 experimental groups:
Preutilisation; and
No preutilisation.
In this experiment, when there is preutilisation, meaning when objects are presented to participants in a traditional manner (materials are in the box, thus using the box as a container), participants are less likely to consider the box for any other use, whereas with no preutilisation (when boxes are presented empty), participants are more likely to think of other uses for the box.
The Two-Cords Problem
Birch and Rabinowitz (1951) adapted the two-cord problem from Norman Maier (1930, 1931), where subjects would be given 2 cords hanging from the ceiling, and 2 heavy objects in the room. They are told they must connect the cords, but they are just far enough apart that one cannot reach the other easily. The solution was to tie one of the heavy objects to a cord and be a weight, and swing the cord as a pendulum, catch the rope as it swings while holding on to the other rope, and then tie them together. The participants are split into 3 groups: Group R, which completes a pre-task of completing an electrical circuit by using a relay, Group S, which completes the circuit with a switch, and Group C which is the control group given no pre-test experience. Group R participants were more likely to use the switch as the weight, and Group S were more likely to use the relay. Both groups did so because their previous experience led them to use the objects a certain way, and functional fixedness did not allow them to see the objects as being used for another purpose.
Barometer Question
The barometer question is an example of an incorrectly designed examination question demonstrating functional fixedness that causes a moral dilemma for the examinator. In its classic form, popularized by American test designer professor Alexander Calandra (1911-2006), the question asked the student to “show how it is possible to determine the height of a tall building with the aid of a barometer?” The examinator was confident that there was one, and only one, correct answer. Contrary to the examinator’s expectations, the student responded with a series of completely different answers. These answers were also correct, yet none of them proved the student’s competence in the specific academic field being tested.
Calandra presented the incident as a real-life, first-person experience that occurred during the Sputnik crisis. Calandra’s essay, “Angels on a Pin”, was published in 1959 in Pride, a magazine of the American College Public Relations Association. It was reprinted in Current Science in 1964, reprinted again in Saturday Review in 1968, and included in the 1969 edition of Calandra’s The Teaching of Elementary Science and Mathematics. In the same year (1969), Calandra’s essay became a subject of an academic discussion. The essay has been referenced frequently since, making its way into books on subjects ranging from teaching, writing skills, workplace counselling, and investment in real estate to chemical industry, computer programming, and integrated circuit design.
Current Conceptual Relevance
Is Functional Fixedness Universal?
Researchers have investigated whether functional fixedness is affected by culture.
In a recent study, preliminary evidence supporting the universality of functional fixedness was found. The study’s purpose was to test if individuals from non-industrialized societies, specifically with low exposure to “high-tech” artefacts, demonstrated functional fixedness. The study tested the Shuar, hunter-horticulturalists of the Amazon region of Ecuador, and compared them to a control group from an industrial culture.
The Shuar community had only been exposed to a limited amount of industrialised artefacts, such as machete, axes, cooking pots, nails, shotguns, and fishhooks, all considered “low-tech”. Two tasks were assessed to participants for the study: the box task, where participants had to build a tower to help a character from a fictional storyline to reach another character with a limited set of varied materials; the spoon task, where participants were also given a problem to solve based on a fictional story of a rabbit that had to cross a river (materials were used to represent settings) and they were given varied materials including a spoon. In the box-task, participants were slower to select the materials than participants in control conditions, but no difference in time to solve the problem was seen. In the spoon task, participants were slower in selection and completion of task. Results showed that Individuals from non-industrial (“technologically sparse cultures”) were susceptible to functional fixedness. They were faster to use artefacts without priming than when design function was explained to them. This occurred even though participants were less exposed to industrialised manufactured artefacts, and that the few artefacts they currently use were used in multiple ways regardless of their design.
“Following the Wrong Footsteps: Fixation Effects of Pictorial Examples in a Design Problem-Solving Task”
Investigators examined in two experiments “whether the inclusion of examples with inappropriate elements, in addition to the instructions for a design problem, would produce fixation effects in students naive to design tasks”. They examined the inclusion of examples of inappropriate elements, by explicitly depicting problematic aspects of the problem presented to the students through example designs. They tested non-expert participants on three problem conditions: with standard instruction, fixated (with inclusion of problematic design), and defixated (inclusion of problematic design accompanied with helpful methods). They were able to support their hypothesis by finding that:
Problematic design examples produce significant fixation effects; and
Fixation effects can be diminished with the use of defixating instructions.
In “The Disposable Spill-Proof Coffee Cup Problem”, adapted from Janson & Smith, 1991, participants were asked to construct as many designs as possible for an inexpensive, disposable, spill-proof coffee cup. Standard condition participants were presented only with instructions. In the fixated condition, participants were presented with instructions, a design, and problems they should be aware of. Finally, in the defixated condition, participants were presented the same as other conditions in addition to suggestions of design elements they should avoid using. The other two problems included building a bike rack, and designing a container for cream cheese.
Techniques to Avoid Functional Fixedness
Overcoming Functional Fixedness in Science Classrooms with Analogical Transfer
Based on the assumption that students are functionally fixed, a study on analogical transfer in the science classroom shed light on significant data that could provide an overcoming technique for functional fixedness. The findings support the fact that students show positive transfer (performance) on problem solving after being presented with analogies of certain structure and format. The present study expanded Duncker’s experiments from 1945 by trying to demonstrate that when students were “presented with a single analogy formatted as a problem, rather than as a story narrative, they would orient the task of problem-solving and facilitate positive transfer”.
A total of 266 freshmen students from a high school science class participated in the study. The experiment was a 2×2 design where conditions: “task contexts” (type and format) vs. “prior knowledge” (specific vs. general) were attested. Students were classified into 5 different groups, where 4 were according to their prior science knowledge (ranging from specific to general), and 1 served as a control group (no analogue presentation). The 4 different groups were then classified into “analogue type and analogue format” conditions, structural or surface types and problem or surface formats.
Inconclusive evidence was found for positive analogical transfer based on prior knowledge; however, groups did demonstrate variability. The problem format and the structural type of analogue presentation showed the highest positive transference to problem solving. The researcher suggested that a well-thought and planned analogy relevant in format and type to the problem-solving task to be completed can be helpful for students to overcome functional fixedness. This study not only brought new knowledge about the human mind at work but also provides important tools for educational purposes and possible changes that teachers can apply as aids to lesson plans.
Uncommitting
One study suggests that functional fixedness can be combated by design decisions from functionally fixed designs so that the essence of the design is kept (Latour, 1994). This helps the subjects who have created functionally fixed designs understand how to go about solving general problems of this type, rather than using the fixed solution for a specific problem. Latour performed an experiment researching this by having software engineers analyse a fairly standard bit of code – the quicksort algorithm – and use it to create a partitioning function. Part of the quicksort algorithm involves partitioning a list into subsets so that it can be sorted; the experimenters wanted to use the code from within the algorithm to just do the partitioning. To do this, they abstracted each block of code in the function, discerning the purpose of it, and deciding if it is needed for the partitioning algorithm. This abstracting allowed them to reuse the code from the quicksort algorithm to create a working partition algorithm without having to design it from scratch.
Overcoming Prototypes
A comprehensive study exploring several classical functional fixedness experiments showed an overlying theme of overcoming prototypes. Those that were successful at completing the tasks had the ability to look beyond the prototype, or the original intention for the item in use. Conversely, those that could not create a successful finished product could not move beyond the original use of the item. This seemed to be the case for functional fixedness categorisation studies as well. Reorganisation into categories of seemingly unrelated items was easier for those that could look beyond intended function. Therefore, there is a need to overcome the prototype in order to avoid functional fixedness. Carnevale (1998) suggests analysing the object and mentally breaking it down into its components. After that is completed, it is essential to explore the possible functions of those parts. In doing so, an individual may familiarise themselves with new ways to use the items that are available to them at the givens. Individuals are therefore thinking creatively and overcoming the prototypes that limit their ability to successfully complete the functional fixedness problem.
The Generic Parts Technique
For each object, you need to decouple its function from its form. McCaffrey (2012) shows a highly effective technique for doing so. As you break an object into its parts, ask yourself two questions. “Can I subdivide the current part further?” If yes, do so. “Does my current description imply a use?” If yes, create a more generic description involving its shape and material. For example, initially I divide a candle into its parts: wick and wax. The word “wick” implies a use: burning to emit light. So, describe it more generically as a string. Since “string” implies a use, I describe it more generically: interwoven fibrous strands. This brings to mind that I could use the wick to make a wig for my hamster. Since “interwoven fibrous strands” does not imply a use, I can stop working on wick and start working on wax. People trained in this technique solved 67% more problems that suffered from functional fixedness than a control group. This technique systematically strips away all the layers of associated uses from an object and its parts.
Nordazepam (INN; marketed under brand names Nordaz, Stilny, Madar, Vegesan, and Calmday; also known as nordiazepam, desoxydemoxepam, and desmethyldiazepam) is a 1,4-benzodiazepine derivative. Like other benzodiazepine derivatives, it has amnesic, anticonvulsant, anxiolytic, muscle relaxant, and sedative properties. However, it is used primarily in the treatment of anxiety disorders. It is an active metabolite of diazepam, chlordiazepoxide, clorazepate, prazepam, pinazepam, and medazepam.
Nordazepam is among the longest lasting (longest half-life) benzodiazepines, and its occurrence as a metabolite is responsible for most cumulative side-effects of its myriad of pro-drugs when they are used repeatedly at moderate-high doses; the nordazepam metabolite oxazepam is also active (and is a more potent, full benzodiazepine-site agonist), which contributes to nordazepam cumulative side-effects but occur too minutely to contribute to the cumulative side-effects of nordazepam pro-drugs (except when they are abused chronically in extremely supra-therapeutic doses).
Side effects
Common side effects of nordazepam include somnolence, which is more common in elderly patients and/or people on high-dose regimens. Hypotonia, which is much less common, is also associated with high doses and/or old age.
Contraindications and Special Caution
Benzodiazepines require special precaution if used in the elderly, during pregnancy, in children, alcohol- or drug-dependent individuals, and individuals with comorbid psychiatric disorders. As with many other drugs, changes in liver function associated with aging or diseases such as cirrhosis, may lead to impaired clearance of nordazepam.
Pharmacology
Nordazepam is a partial agonist at the GABAA receptor, which makes it less potent than other benzodiazepines, particularly in its amnesic and muscle-relaxing effects. Its elimination half life is between 36 and 200 hours, with wide variation among individuals; factors such as age and gender are known to impact it. The variation of reported half-lives are attributed to differences in nordazepam metabolism and that of its metabolites as nordazepam is hydroxylated to active metabolites such as oxazepam, before finally being glucuronidated and excreted in the urine. This can be attributed to extremely variable hepatic and renal metabolic functions among individuals depending upon a number of factors (including age, ethnicity, disease, and current or previous use/abuse of other drugs/medicines).
Pregnancy and Nursing Mothers
Nordazepam, like other benzodiazepines, easily crosses the placental barrier, so the drug should not be administered during the first trimester of pregnancy. In case of serious medical reasons, nordazepam can be given in late pregnancy, but the foetus, due to the pharmacological action of the drug, may experience side effects such as hypothermia, hypotonia, and sometimes mild respiratory depression. Since nordazepam and other benzodiazepines are excreted in breast milk, the substance should not be administered to mothers who are breastfeeding. Discontinuing of breast-feeding is indicated for regular intake by the mother.
Nordazepam and other sedative-hypnotic drugs are detected frequently in cases of people suspected of driving under the influence of drugs. Many drivers have blood levels far exceeding the therapeutic dose range, suggesting benzodiazepines are commonly used in doses higher than the recommended doses.





You must be logged in to post a comment.