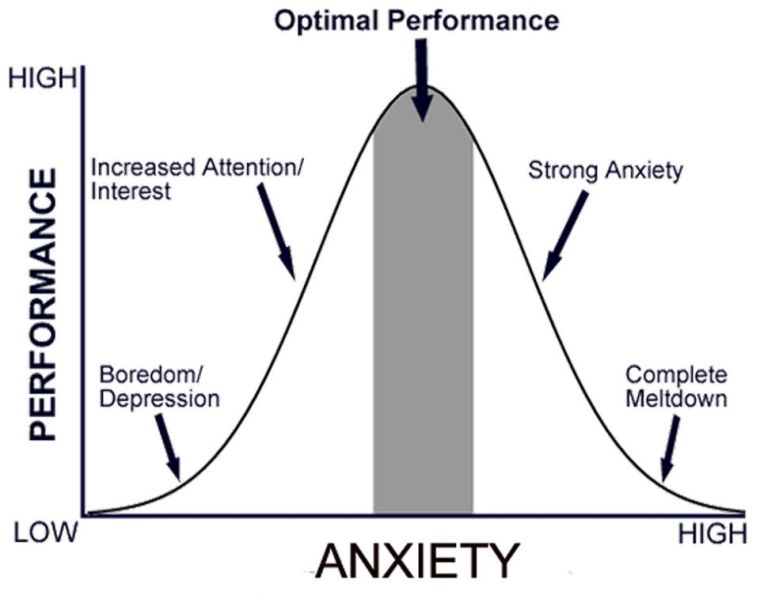
The effects of anxiety on performance can be shown on a curve.
As the level of anxiety increases, performance efficiency increases proportionately, but only up to a point.
As anxiety increases further, performance efficiency decreases.
Before the peak of the curve, anxiety is considered adaptive because it helps people prepare for a crisis and improve their functioning.
Beyond the peak of the curve, anxiety is considered maladaptive because it produces distress and impairs functioning.
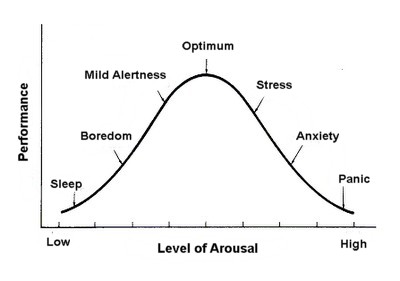
The Yerkes-Dodson Law
The Yerkes–Dodson law is an empirical relationship between arousal and performance, originally developed by psychologists Robert M. Yerkes and John Dillingham Dodson in 1908.
The law dictates that performance increases with physiological or mental arousal, but only up to a point.
Levels of Arousal (or Anxiety)
Research suggests that different tasks require different levels of arousal for optimal performance. For example:
- Difficult or intellectually demanding tasks may require a lower level of arousal (to facilitate concentration); whereas
- Tasks demanding stamina or persistence may be performed better with higher levels of arousal (to increase motivation).
Because of task differences, the shape of the curve can be highly variable (Diamond et al., 2007).
- For simple or well-learned tasks, the relationship is monotonic, and performance improves as arousal increases.
- For complex, unfamiliar, or difficult tasks, the relationship between arousal and performance reverses after a point, and performance thereafter declines as arousal increases.
What is the Relationship to Glucocorticoids?
A 2007 review of the effects of stress hormones (glucocorticoids, GC) and human cognition revealed that memory performance versus circulating levels of glucocorticoids does manifest an upside down U shaped curve and the authors noted the resemblance to the Yerkes-Dodson curve.
For example, long-term potentiation (LTP) (the process of forming long-term memories) is optimal when glucocorticoid levels are mildly elevated whereas significant decreases of LTP are observed after adrenalectomy (low GC state) or after exogenous glucocorticoid administration (high GC state).
This review also revealed that in order for a situation to induce a stress response, it has to be interpreted as one or more of the following:
- Novel;
- Unpredictable;
- Not controllable by the individual; and/or
- A social evaluative threat (negative social evaluation possibly leading to social rejection).
It has also been shown that elevated levels of glucocorticoids enhance memory for emotionally arousing events but lead more often than not to poor memory for material unrelated to the source of stress/emotional arousal (Lupien et al, 2007).
References
Diamond, D.M., Campbell, A.M., Park, C.P., Halonen, J. & Zoladz, P.R. (2007). The Temporal Dynamics Model of Emotional Memory Processing: A Synthesis on the Neurobiological Basis of Stress-Induced Amnesia, Flashbulb and Traumatic Memories, and the Yerkes–Dodson Law. Neural Plasticity. 2007: 60803. http://dx.doi.org/10.1155/2007/60803.
Lupien, S.J., Maheu, F., Tu, M., Fioco, A. & Schramek, T.E. (2007) The effects of stress and stress hormones on human cognition: Implications for the field of brain and cognition. Brain and Cognition. 65(3), pp.209-237. https://doi.org/10.1016/j.bandc.2007.02.007.
Yerkes, R.M. & Dodson, J.D. (1908) The Relation of Strength of Stimulus to Rapidity of Habit-Formation. Journal of Comparative Neurology and Psychology. 18, pp.459-482.







You must be logged in to post a comment.