The Altman Self-Rating Mania Scale (ASRM) is a 5-item self-reported diagnostic scale which can be used to assess the presence and severity manic and hypomanic symptoms, most commonly in patients diagnosed with bipolar disorder.
Effectiveness
The ASRM scale has been shown to be an effective self-reported questionnaire for screening patients with acute mania as well as measuring anti-manic treatment effects. Though only a 5-question instrument, the scale’s compatibility with the clinician administered Young Mania Rating Scale and the DSM-IV criteria give substantial diagnostic power for such a brief instrument.
Format
The Altman Self-Rating Mania Scale assess differences in “normal” or baseline levels in five subjective and behavioural areas:
Positive mood.
Self-confidence.
Sleep patterns.
Speech patterns and amount.
Motor activity.
Each of these areas has five statements which correspond to scores 0 through 4; with 0 being unchanged from “normal” or baseline, to 4 being overtly manic thoughts or behaviour. The subject is asked to choose one statement from each of the five areas that best describes the way they have been feeling over the past week.
Scoring
Scores above a 5 are indicative of mania, or hypomania, with the severity of symptoms increasing with higher scores. Examining score changes over time is also used to determine the efficacy of a particular treatment in a clinical setting and to qualify whether the severity a manic episode is increasing or decreasing.
Mania, also known as manic syndrome, is a mental and behavioural disorder defined as a state of abnormally elevated arousal, affect, and energy level, or “a state of heightened overall activation with enhanced affective expression together with lability of affect.”
During a manic episode, an individual will experience rapidly changing emotions and moods, highly influenced by surrounding stimuli. Although mania is often conceived as a “mirror image” to depression, the heightened mood can be either euphoric or dysphoric. As the mania intensifies, irritability can be more pronounced and result in anxiety or anger.
The symptoms of mania include elevated mood (either euphoric or irritable), flight of ideas and pressure of speech, increased energy, decreased need and desire for sleep, and hyperactivity. They are most plainly evident in fully developed hypomanic states. However, in full-blown mania, they undergo progressively severe exacerbations and become more and more obscured by other signs and symptoms, such as delusions and fragmentation of behaviour.
The nosology of the various stages of a manic episode has changed over the decades. The word derives from the Ancient Greek μανία (manía), “madness, frenzy” and the verb μαίνομαι (maínomai), “to be mad, to rage, to be furious”.
Causes and Diagnosis
Mania is a syndrome with multiple causes. Although the vast majority of cases occur in the context of bipolar disorder, it is a key component of other psychiatric disorders (such as schizoaffective disorder, bipolar type) and may also occur secondary to various general medical conditions, such as multiple sclerosis; certain medications may perpetuate a manic state, for example prednisone; or substances prone to abuse, especially stimulants, such as caffeine and cocaine. In the current DSM-5, hypomanic episodes are separated from the more severe full manic episodes, which, in turn, are characterised as either mild, moderate, or severe, with certain diagnostic criteria (e.g. catatonia, psychosis). Mania is divided into three stages:
Hypomania, or stage I;
Acute mania, or stage II; and
Delirious mania (delirium), or stage III.
This “staging” of a manic episode is useful from a descriptive and differential diagnostic point of view.
Mania varies in intensity, from mild mania (hypomania) to delirious mania, marked by such symptoms as disorientation, florid psychosis, incoherence, and catatonia. Standardised tools such as Altman Self-Rating Mania Scale and Young Mania Rating Scale can be used to measure severity of manic episodes. Because mania and hypomania have also long been associated with creativity and artistic talent, it is not always the case that the clearly manic/hypomanic bipolar patient needs or wants medical help; such persons often either retain sufficient self-control to function normally or are unaware that they have “gone manic” severely enough to be committed or to commit themselves. Manic persons often can be mistaken for being under the influence of drugs.
Classification
Mixed States
Refer to Mixed Affective State.
In a mixed affective state, the individual, though meeting the general criteria for a hypomanic (discussed below) or manic episode, experiences three or more concurrent depressive symptoms. This has caused some speculation, among clinicians, that mania and depression, rather than constituting “true” polar opposites, are, rather, two independent axes in a unipolar – bipolar spectrum.
A mixed affective state, especially with prominent manic symptoms, places the patient at a greater risk for suicide. Depression on its own is a risk factor but, when coupled with an increase in energy and goal-directed activity, the patient is far more likely to act with violence on suicidal impulses.
Hypomania, which means “less than mania”, is a lowered state of mania that does little to impair function or decrease quality of life. It may, in fact, increase productivity and creativity. In hypomania, there is less need for sleep and both goal-motivated behaviour and metabolism increase. Some studies exploring brain metabolism in subjects with hypomania, however, did not find any conclusive link; while there are studies that reported abnormalities, some failed to detect differences. Though the elevated mood and energy level typical of hypomania could be seen as a benefit, true mania itself generally has many undesirable consequences including suicidal tendencies, and hypomania can, if the prominent mood is irritable as opposed to euphoric, be a rather unpleasant experience. In addition, the exaggerated case of hypomania can lead to problems. For instance, trait-based positivity for a person could make them more engaging and outgoing, and cause them to have a positive outlook in life. When exaggerated in hypomania, however, such a person can display excessive optimism, grandiosity, and poor decision making, often with little regard to the consequences.
Associated Disorders
A single manic episode, in the absence of secondary causes, (i.e. substance use disorders, pharmacologics, or general medical conditions) is often sufficient to diagnose bipolar I disorder. Hypomania may be indicative of bipolar II disorder. Manic episodes are often complicated by delusions and/or hallucinations; and if the psychotic features persist for a duration significantly longer than the episode of typical mania (two weeks or more), a diagnosis of schizoaffective disorder is more appropriate. Certain obsessive-compulsive spectrum disorders as well as impulse control disorders share the suffix “-mania,” namely, kleptomania, pyromania, and trichotillomania. Despite the unfortunate association implied by the name, however, no connection exists between mania or bipolar disorder and these disorders. Furthermore, evidence indicates a B12 deficiency can also cause symptoms characteristic of mania and psychosis.
Hyperthyroidism can produce similar symptoms to those of mania, such as agitation, elevated mood, increased energy, hyperactivity, sleep disturbances and sometimes, especially in severe cases, psychosis.
Signs and Symptoms
A manic episode is defined in the American Psychiatric Association’s diagnostic manual as a “distinct period of abnormally and persistently elevated, expansive, or irritable mood and abnormally and persistently increased activity or energy, lasting at least 1 week and present most of the day, nearly every day (or any duration, if hospitalisation is necessary),” where the mood is not caused by drugs/medication or a non-mental medical illness (e.g. hyperthyroidism), and: (a) is causing obvious difficulties at work or in social relationships and activities, or (b) requires admission to hospital to protect the person or others, or (c) the person is suffering psychosis.
To be classified as a manic episode, while the disturbed mood and an increase in goal-directed activity or energy is present, at least three (or four, if only irritability is present) of the following must have been consistently present:
Inflated self-esteem or grandiosity.
Decreased need for sleep (e.g. feels rested after 3 hours of sleep).
More talkative than usual, or acts pressured to keep talking.
Flights of ideas or subjective experience that thoughts are racing.
Increase in goal-directed activity, or psychomotor acceleration.
Distractibility (too easily drawn to unimportant or irrelevant external stimuli).
Excessive involvement in activities with a high likelihood of painful consequences.(e.g. extravagant shopping, improbable commercial schemes, hypersexuality).
Though the activities one participates in while in a manic state are not always negative, those with the potential to have negative outcomes are far more likely.
If the person is concurrently depressed, they are said to be having a mixed episode.
The World Health Organisation’s classification system defines a manic episode as one where mood is higher than the person’s situation warrants and may vary from relaxed high spirits to barely controllable exuberance, is accompanied by hyperactivity, a compulsion to speak, a reduced sleep requirement, difficulty sustaining attention, and/or often increased distractibility. Frequently, confidence and self-esteem are excessively enlarged, and grand, extravagant ideas are expressed. Behaviour that is out-of-character and risky, foolish or inappropriate may result from a loss of normal social restraint.
Some people also have physical symptoms, such as sweating, pacing, and weight loss. In full-blown mania, often the manic person will feel as though their goal(s) are of paramount importance, that there are no consequences, or that negative consequences would be minimal, and that they need not exercise restraint in the pursuit of what they are after. Hypomania is different, as it may cause little or no impairment in function. The hypomanic person’s connection with the external world, and its standards of interaction, remain intact, although intensity of moods is heightened. But those who suffer from prolonged unresolved hypomania do run the risk of developing full mania, and may cross that “line” without even realising they have done so.
One of the signature symptoms of mania (and to a lesser extent, hypomania) is what many have described as racing thoughts. These are usually instances in which the manic person is excessively distracted by objectively unimportant stimuli. This experience creates an absent-mindedness where the manic individual’s thoughts totally preoccupy them, making them unable to keep track of time, or be aware of anything besides the flow of thoughts. Racing thoughts also interfere with the ability to fall asleep.
Manic states are always relative to the normal state of intensity of the afflicted individual; thus, already irritable patients may find themselves losing their tempers even more quickly, and an academically gifted person may, during the hypomanic stage, adopt seemingly “genius” characteristics and an ability to perform and articulate at a level far beyond that which they would be capable of during euthymia. A very simple indicator of a manic state would be if a heretofore clinically depressed patient suddenly becomes inordinately energetic, enthusiastic, cheerful, aggressive, or “over-happy”. Other, often less obvious, elements of mania include delusions (generally of either grandeur or persecution, according to whether the predominant mood is euphoric or irritable), hypersensitivity, hypervigilance, hypersexuality, hyper-religiosity, hyperactivity and impulsivity, a compulsion to over explain (typically accompanied by pressure of speech), grandiose schemes and ideas, and a decreased need for sleep (for example, feeling rested after only 3 or 4 hours of sleep). In the case of the latter, the eyes of such patients may both look and seem abnormally “wide open”, rarely blinking, and may contribute to some clinicians’ erroneous belief that these patients are under the influence of a stimulant drug, when the patient, in fact, is either not on any mind-altering substances or is actually on a depressant drug. Individuals may also engage in out-of-character behaviour during the episode, such as questionable business transactions, wasteful expenditures of money (e.g. spending sprees), risky sexual activity, abuse of recreational substances, excessive gambling, reckless behaviour (such as extreme speeding or other daredevil activity), abnormal social interaction (e.g. over-familiarity and conversing with strangers), or highly vocal arguments. These behaviours may increase stress in personal relationships, lead to problems at work, and increase the risk of altercations with law enforcement. There is a high risk of impulsively taking part in activities potentially harmful to the self and others.
Although “severely elevated mood” sounds somewhat desirable and enjoyable, the experience of mania is ultimately often quite unpleasant and sometimes disturbing, if not frightening, for the person involved and for those close to them, and it may lead to impulsive behaviour that may later be regretted. It can also often be complicated by the sufferer’s lack of judgment and insight regarding periods of exacerbation of characteristic states. Manic patients are frequently grandiose, obsessive, impulsive, irritable, belligerent, and frequently deny anything is wrong with them. Because mania frequently encourages high energy and decreased perception of need or ability to sleep, within a few days of a manic cycle, sleep-deprived psychosis may appear, further complicating the ability to think clearly. Racing thoughts and misperceptions lead to frustration and decreased ability to communicate with others.
Mania may also, as earlier mentioned, be divided into three “stages”. Stage I corresponds with hypomania and may feature typical hypomanic characteristics, such as gregariousness and euphoria. In stages II and III mania, however, the patient may be extraordinarily irritable, psychotic or even delirious. These latter two stages are referred to as acute and delirious (or Bell’s), respectively.
Cause
Various triggers have been associated with switching from euthymic or depressed states into mania. One common trigger of mania is antidepressant therapy. Studies show that the risk of switching while on an antidepressant is between 6-69%. Dopaminergic drugs such as reuptake inhibitors and dopamine agonists may also increase risk of switch. Other medication possibly include glutaminergic agents and drugs that alter the hypothalamic-pituitary-adrenal (HPA) axis. Lifestyle triggers include irregular sleep-wake schedules and sleep deprivation, as well as extremely emotional or stressful stimuli.
Various genes that have been implicated in genetic studies of bipolar have been manipulated in preclinical animal models to produce syndromes reflecting different aspects of mania. CLOCK and DBP polymorphisms have been linked to bipolar in population studies, and behavioural changes induced by knockout are reversed by lithium treatment. Metabotropic glutamate receptor 6 has been genetically linked to bipolar, and found to be under-expressed in the cortex. Pituitary adenylate cyclase-activating peptide has been associated with bipolar in gene linkage studies, and knockout in mice produces mania like-behaviour. Targets of various treatments such as GSK-3, and ERK1 have also demonstrated mania like behaviour in preclinical models.
Mania may be associated with strokes, especially cerebral lesions in the right hemisphere.
Deep brain stimulation of the subthalamic nucleus in Parkinson’s disease has been associated with mania, especially with electrodes placed in the ventromedial STN. A proposed mechanism involves increased excitatory input from the STN to dopaminergic nuclei.
Mania can also be caused by physical trauma or illness. When the causes are physical, it is called secondary mania.
Mechanism
Refer to Biology of Bipolar Disorder.
The mechanism underlying mania is unknown, but the neurocognitive profile of mania is highly consistent with dysfunction in the right prefrontal cortex, a common finding in neuroimaging studies. Various lines of evidence from post-mortem studies and the putative mechanisms of anti-manic agents point to abnormalities in GSK-3, dopamine, Protein kinase C and Inositol monophosphatase.
Meta analysis of neuroimaging studies demonstrate increased thalamic activity, and bilaterally reduced inferior frontal gyrus activation. Activity in the amygdala and other subcortical structures such as the ventral striatum tend to be increased, although results are inconsistent and likely dependent upon task characteristics such as valence. Reduced functional connectivity between the ventral prefrontal cortex and amygdala along with variable findings supports a hypothesis of general dysregulation of subcortical structures by the prefrontal cortex. A bias towards positively valenced stimuli, and increased responsiveness in reward circuitry may predispose towards mania. Mania tends to be associated with right hemisphere lesions, while depression tends to be associated with left hemisphere lesions.
Post-mortem examinations of bipolar disorder demonstrate increased expression of Protein Kinase C (PKC). While limited, some studies demonstrate manipulation of PKC in animals produces behavioural changes mirroring mania, and treatment with PKC inhibitor tamoxifen (also an anti-oestrogen drug) demonstrates antimanic effects. Traditional antimanic drugs also demonstrate PKC inhibiting properties, among other effects such as GSK3 inhibition.
Manic episodes may be triggered by dopamine receptor agonists, and this combined with tentative reports of increased VMAT2 activity, measured via PET scans of radioligand binding, suggests a role of dopamine in mania. Decreased cerebrospinal fluid levels of the serotonin metabolite 5-HIAA have been found in manic patients too, which may be explained by a failure of serotonergic regulation and dopaminergic hyperactivity.
Limited evidence suggests that mania is associated with behavioural reward hypersensitivity, as well as with neural reward hypersensitivity. Electrophysiological evidence supporting this comes from studies associating left frontal EEG activity with mania. As left frontal EEG activity is generally thought to be a reflection of behavioural activation system activity, this is thought to support a role for reward hypersensitivity in mania. Tentative evidence also comes from one study that reported an association between manic traits and feedback negativity during receipt of monetary reward or loss. Neuroimaging evidence during acute mania is sparse, but one study reported elevated orbitofrontal cortex activity to monetary reward, and another study reported elevated striatal activity to reward omission. The latter finding was interpreted in the context of either elevated baseline activity (resulting in a null finding of reward hypersensitivity), or reduced ability to discriminate between reward and punishment, still supporting reward hyperactivity in mania. Punishment hyposensitivity, as reflected in a number of neuroimaging studies as reduced lateral orbitofrontal response to punishment, has been proposed as a mechanism of reward hypersensitivity in mania.
Diagnosis
In the ICD-10 there are several disorders with the manic syndrome:
Organic manic disorder (F06.30).
Mania without psychotic symptoms (F30.1).
Mania with psychotic symptoms (F30.2).
Other manic episodes (F30.8).
Unspecified manic episode (F30.9).
Manic type of schizoaffective disorder (F25.0).
Bipolar affective disorder, current episode manic without psychotic symptoms (F31.1).
Bipolar affective disorder, current episode manic with psychotic symptoms (F31.2).
Treatment
Before beginning treatment for mania, careful differential diagnosis must be performed to rule out secondary causes.
The acute treatment of a manic episode of bipolar disorder involves the utilisation of either a mood stabiliser (Carbamazepine, valproate, lithium, or lamotrigine) or an atypical antipsychotic (olanzapine, quetiapine, risperidone, or aripiprazole). The use of antipsychotic agents in the treatment of acute mania was reviewed by Tohen and Vieta in 2009.
When the manic behaviours have gone, long-term treatment then focuses on prophylactic treatment to try to stabilise the patient’s mood, typically through a combination of pharmacotherapy and psychotherapy. The likelihood of having a relapse is very high for those who have experienced two or more episodes of mania or depression. While medication for bipolar disorder is important to manage symptoms of mania and depression, studies show relying on medications alone is not the most effective method of treatment. Medication is most effective when used in combination with other bipolar disorder treatments, including psychotherapy, self-help coping strategies, and healthy lifestyle choices.
Lithium is the classic mood stabiliser to prevent further manic and depressive episodes. A systematic review found that long term lithium treatment substantially reduces the risk of bipolar manic relapse, by 42%. Anticonvulsants such as valproate, oxcarbazepine and carbamazepine are also used for prophylaxis. More recent drug solutions include lamotrigine and topiramate, both anticonvulsants as well.
In some cases, long-acting benzodiazepines, particularly clonazepam, are used after other options are exhausted. In more urgent circumstances, such as in emergency rooms, lorazepam, combined with haloperidol, is used to promptly alleviate symptoms of agitation, aggression, and psychosis.
Antidepressant monotherapy is not recommended for the treatment of depression in patients with bipolar disorders I or II, and no benefit has been demonstrated by combining antidepressants with mood stabilisers in these patients. Some atypical antidepressants, however, such as mirtazepine and trazodone have been occasionally used after other options have failed.
Society and Culture
In Electroboy: A Memoir of Mania by Andy Behrman, he describes his experience of mania as “the most perfect prescription glasses with which to see the world… life appears in front of you like an oversized movie screen”. Behrman indicates early in his memoir that he sees himself not as a person suffering from an uncontrollable disabling illness, but as a director of the movie that is his vivid and emotionally alive life. There is some evidence that people in the creative industries suffer from bipolar disorder more often than those in other occupations. Winston Churchill had periods of manic symptoms that may have been both an asset and a liability.
English actor Stephen Fry, who suffers from bipolar disorder, recounts manic behaviour during his adolescence: “When I was about 17 … going around London on two stolen credit cards, it was a sort of fantastic reinvention of myself, an attempt to. I bought ridiculous suits with stiff collars and silk ties from the 1920s, and would go to the Savoy and Ritz and drink cocktails.” While he has experienced suicidal thoughts, he says the manic side of his condition has had positive contributions on his life.
The following is a quick overview of and topical guide to bipolar disorder (you can find a detailed article on Bipolar Disorder here and an Overview of Bipolar Disorder in Children here).
Bipolar disorder is characterised by episodes of depression and mania.
Bipolar disorder is a mental disorder with periods of depression and periods of elevated mood. The elevated mood is significant and is known as mania or hypomania, depending on its severity, or whether symptoms of psychosis are present. During mania, an individual behaves or feels abnormally energetic, happy, or irritable. Individuals often make poorly thought out decisions with little regard to the consequences. The need for sleep is usually reduced during manic phases. During periods of depression, there may be crying, a negative outlook on life, and poor eye contact with others. The risk of suicide among those with the illness is high at greater than 6% over 20 years, while self-harm occurs in 30-40%. Other mental health issues such as anxiety disorders and substance use disorder are commonly associated. Also known as manic depression.
What is Bipolar Disorder?
Bipolar disorder can be described as all of the following:
Mental disorder.
Functional abnormality or disturbance characterised by a behavioural or mental pattern that may cause suffering or a poor ability to function in life.
Such features may be persistent, relapsing and remitting, or occur as a single episode.
You can find an overview of the Biology of Bipolar Disorder here.
A state of hyperactivity, heightened mood (euphoric or irritable), low sleep, pressured speech, grandiosity, and/or racing thoughts; may include psychotic features like delusions or hallucinations.
Bipolar disorder, previously known as manic depression, is a mood disorder characterised by periods of depression and periods of abnormally-elevated mood that last from days to weeks each. If the elevated mood is severe or associated with psychosis, it is called mania; if it is less severe, it is called hypomania. During mania, an individual behaves or feels abnormally energetic, happy or irritable, and they often make impulsive decisions with little regard for the consequences. There is usually also a reduced need for sleep during manic phases. During periods of depression, the individual may experience crying and have a negative outlook on life and poor eye contact with others. The risk of suicide is high; over a period of 20 years, 6% of those with bipolar disorder died by suicide, while 30-40% engaged in self-harm. Other mental health issues, such as anxiety disorders and substance use disorders, are commonly associated with bipolar disorder.
Bipolar disorder is characterised by episodes of depression and mania.
While the causes of bipolar disorder are not clearly understood, both genetic and environmental factors are thought to play a role. Many genes, each with small effects, may contribute to the development of the disorder. Genetic factors account for about 70-90% of the risk of developing bipolar disorder. Environmental risk factors include a history of childhood abuse and long-term stress. The condition is classified as bipolar I disorder if there has been at least one manic episode, with or without depressive episodes, and as bipolar II disorder if there has been at least one hypomanic episode (but no full manic episodes) and one major depressive episode. If these symptoms are due to drugs or medical problems, they are not diagnosed as bipolar disorder. Other conditions that have overlapping symptoms with bipolar disorder include attention deficit hyperactivity disorder, personality disorders, schizophrenia, and substance use disorder as well as many other medical conditions. Medical testing is not required for a diagnosis, though blood tests or medical imaging can rule out other problems.
Mood stabilisers – lithium and certain anticonvulsants such as valproate and carbamazepine as well as atypical antipsychotics such as aripiprazole – are the mainstay of long-term pharmacologic relapse prevention. Antipsychotics are additionally given during acute manic episodes as well as in cases where mood stabilisers are poorly tolerated or ineffective. In patients where compliance is of concern, long-acting injectable formulations are available. There is some evidence that psychotherapy improves the course of this disorder. The use of antidepressants in depressive episodes is controversial: they can be effective but have been implicated in triggering manic episodes. The treatment of depressive episodes, therefore, is often difficult. Electroconvulsive therapy (ECT) is effective in acute manic and depressive episodes, especially with psychosis or catatonia (a syndrome characterised by profound unresponsiveness or stupor with abnormal movements in a person who is otherwise awake). Admission to a psychiatric hospital may be required if a person is a risk to themselves or others; involuntary treatment is sometimes necessary if the affected person refuses treatment.
Bipolar disorder occurs in approximately 1% of the global population. In the United States, about 3% are estimated to be affected at some point in their life; rates appear to be similar in females and males. Symptoms most commonly begin between the ages of 20 and 25 years old; an earlier onset in life is associated with a worse prognosis. Interest in functioning in the assessment of patients with bipolar disorder is growing, with an emphasis on specific domains such as work, education, social life, family, and cognition. Around one-quarter to one-third of people with bipolar disorder have financial, social or work-related problems due to the illness. Bipolar disorder is among the top 20 causes of disability worldwide and leads to substantial costs for society. Due to lifestyle choices and the side effects of medications, the risk of death from natural causes such as coronary heart disease in people with bipolar disorder is twice that of the general population.
Other Names
Bipolar affective disorder (BPAD).
Bipolar illness.
Manic depression.
Manic depressive disorder.
Manic-depressive illness (historical).
Manic-depressive psychosis.
Circular insanity (historical).
Bipolar disease.
In Brief
Specialty: Psychiatry.
Symptoms: Periods of depression and elevated mood.
Complications: Suicide, self-harm.
Usual onset: 25 years old.
Types: Bipolar I disorder, bipolar II disorder, others.
Causes: Environmental and genetic.
Risk factors: Family history, childhood abuse, long-term stress.
In the early 1800s, French psychiatrist Jean-Étienne Dominique Esquirol’s lypemania, one of his affective monomanias, was the first elaboration on what was to become modern depression. The basis of the current conceptualisation of bipolar illness can be traced back to the 1850s. In 1850, Jean-Pierre Falret described “circular insanity” (la folie circulaire; the lecture was summarised in 1851 in the “Gazette des hôpitaux” (“Hospital Gazette”). Three years later, in 1854, Jules-Gabriel-François Baillarger (1809-1890) described to the French Imperial Académie Nationale de Médecine a biphasic mental illness causing recurrent oscillations between mania and melancholia, which he termed folie à double forme, “madness in double form”). Baillarger’s original paper, “De la folie à double forme,” appeared in the medical journal Annales médico-psychologiques (Medico-psychological annals) in 1854.
These concepts were developed by the German psychiatrist Emil Kraepelin (1856-1926), who, using Kahlbaum’s concept of cyclothymia, categorised and studied the natural course of untreated bipolar patients. He coined the term manic depressive psychosis, after noting that periods of acute illness, manic or depressive, were generally punctuated by relatively symptom-free intervals where the patient was able to function normally.
The term “manic-depressive reaction” appeared in the first version of the DSM in 1952, influenced by the legacy of Adolf Meyer. Subtyping into “unipolar” depressive disorders and bipolar disorders has its origin in Karl Kleist’s concept – since 1911 – of unipolar and bipolar affective disorders, which was used by Karl Leonhard in 1957 to differentiate between unipolar and bipolar disorder in depression. These subtypes have been regarded as separate conditions since publication of the DSM-III. The subtypes bipolar II and rapid cycling have been included since the DSM-IV, based on work from the 1970s by David Dunner, Elliot Gershon, Frederick Goodwin, Ronald Fieve, and Joseph Fleiss.
Signs and Symptoms
Late adolescence and early adulthood are peak years for the onset of bipolar disorder. The condition is characterised by intermittent episodes of mania and/or depression, with an absence of symptoms in between. During these episodes, people with bipolar disorder exhibit disruptions in normal mood, psychomotor activity (the level of physical activity that is influenced by mood) – e.g. constant fidgeting during mania or slowed movements during depression – circadian rhythm and cognition. Mania can present with varying levels of mood disturbance, ranging from euphoria, which is associated with “classic mania”, to dysphoria and irritability. Psychotic symptoms such as delusions or hallucinations may occur in both manic and depressive episodes; their content and nature are consistent with the person’s prevailing mood.
Bipolar mood shifts.
According to the DSM-5 criteria, mania is distinguished from hypomania by length: hypomania is present if elevated mood symptoms persist for at least four consecutive days, while mania is present if such symptoms persist for more than a week. Unlike mania, hypomania is not always associated with impaired functioning. The biological mechanisms responsible for switching from a manic or hypomanic episode to a depressive episode, or vice versa, remain poorly understood.
Manic Episodes
Also known as a manic episode, mania is a distinct period of at least one week of elevated or irritable mood, which can range from euphoria to delirium. The core symptom of mania involves an increase in energy of psychomotor activity. Mania can also present with increased self-esteem or grandiosity, racing thoughts, pressured speech that is difficult to interrupt, decreased need for sleep, disinhibited social behaviour, increased goal-oriented activities and impaired judgement, which can lead to exhibition of behaviours characterised as impulsive or high-risk, such as hypersexuality or excessive spending. To fit the definition of a manic episode, these behaviours must impair the individual’s ability to socialise or work. If untreated, a manic episode usually lasts three to six months.
In severe manic episodes, a person can experience psychotic symptoms, where thought content is affected along with mood. They may feel unstoppable, or as if they have a special relationship with God, a great mission to accomplish, or other grandiose or delusional ideas. This may lead to violent behaviour and, sometimes, hospitalisation in an inpatient psychiatric hospital. The severity of manic symptoms can be measured by rating scales such as the Young Mania Rating Scale, though questions remain about the reliability of these scales.
The onset of a manic or depressive episode is often foreshadowed by sleep disturbance. Manic individuals often have a history of substance abuse developed over years as a form of “self-medication”.
Hypomanic Episodes
Hypomania is the milder form of mania, defined as at least four days of the same criteria as mania, but which does not cause a significant decrease in the individual’s ability to socialise or work, lacks psychotic features such as delusions or hallucinations, and does not require psychiatric hospitalisation. Overall functioning may actually increase during episodes of hypomania and is thought to serve as a defence mechanism against depression by some. Hypomanic episodes rarely progress to full-blown manic episodes. Some people who experience hypomania show increased creativity, while others are irritable or demonstrate poor judgment.
Hypomania may feel good to some individuals who experience it, though most people who experience hypomania state that the stress of the experience is very painful. People with bipolar disorder who experience hypomania tend to forget the effects of their actions on those around them. Even when family and friends recognise mood swings, the individual will often deny that anything is wrong. If not accompanied by depressive episodes, hypomanic episodes are often not deemed problematic unless the mood changes are uncontrollable or volatile. Most commonly, symptoms continue for time periods from a few weeks to a few months.
Symptoms of the depressive phase of bipolar disorder include persistent feelings of sadness, irritability or anger, loss of interest in previously enjoyed activities, excessive or inappropriate guilt, hopelessness, sleeping too much or not enough, changes in appetite and/or weight, fatigue, problems concentrating, self-loathing or feelings of worthlessness, and thoughts of death or suicide. Although the DSM-5 criteria for diagnosing unipolar and bipolar episodes are the same, some clinical features are more common in the latter, including increased sleep, sudden onset and resolution of symptoms, significant weight gain or loss, and severe episodes after childbirth.
The earlier the age of onset, the more likely the first few episodes are to be depressive. For most people with bipolar types 1 and 2, the depressive episodes are much longer than the manic or hypomanic episodes. Since a diagnosis of bipolar disorder requires a manic or hypomanic episode, many affected individuals are initially misdiagnosed as having major depression and incorrectly treated with prescribed antidepressants.
In bipolar disorder, a mixed state is an episode during which symptoms of both mania and depression occur simultaneously. Individuals experiencing a mixed state may have manic symptoms such as grandiose thoughts while simultaneously experiencing depressive symptoms such as excessive guilt or feeling suicidal. They are considered to have a higher risk for suicidal behaviour as depressive emotions such as hopelessness are often paired with mood swings or difficulties with impulse control. Anxiety disorders occur more frequently as a comorbidity in mixed bipolar episodes than in non-mixed bipolar depression or mania. Substance (including alcohol) abuse also follows this trend, thereby appearing to depict bipolar symptoms as no more than a consequence of substance abuse.
Comorbid Conditions
The diagnosis of bipolar disorder can be complicated by coexisting (comorbid) psychiatric conditions including obsessive-compulsive disorder, substance-use disorder, eating disorders, attention deficit hyperactivity disorder, social phobia, premenstrual syndrome (including premenstrual dysphoric disorder), or panic disorder. A thorough longitudinal analysis of symptoms and episodes, assisted if possible by discussions with friends and family members, is crucial to establishing a treatment plan where these comorbidities exist. Children of parents with bipolar disorder more frequently have other mental health problems.
People with bipolar disorder often have other co-existing psychiatric conditions such as anxiety (present in about 71% of people with bipolar disorder), substance use (56%), personality disorders (36%) and attention deficit hyperactivity disorder (10-20%) which can add to the burden of illness and worsen the prognosis. Certain medical conditions are also more common in people with bipolar disorder as compared to the general population. This includes increased rates of metabolic syndrome (present in 37% of people with bipolar disorder), migraine headaches (35%), obesity (21%) and type 2 diabetes (14%). This contributes to a risk of death that is two times higher in those with bipolar disorder as compared to the general population.
Substance abuse is a common comorbidity in bipolar disorder; the subject has been widely reviewed.
Causes
The causes of bipolar disorder likely vary between individuals and the exact mechanism underlying the disorder remains unclear. Genetic influences are believed to account for 73-93% of the risk of developing the disorder indicating a strong hereditary component. The overall heritability of the bipolar spectrum has been estimated at 0.71. Twin studies have been limited by relatively small sample sizes but have indicated a substantial genetic contribution, as well as environmental influence. For bipolar I disorder, the rate at which identical twins (same genes) will both have bipolar I disorder (concordance) is around 40%, compared to about 5% in fraternal twins. A combination of bipolar I, II, and cyclothymia similarly produced rates of 42% and 11% (identical and fraternal twins, respectively). The rates of bipolar II combinations without bipolar I are lower – bipolar II at 23 and 17%, and bipolar II combining with cyclothymia at 33 and 14% – , which may reflect relatively higher genetic heterogeneity.
The cause of bipolar disorders overlaps with major depressive disorder. When defining concordance as the co-twins having either bipolar disorder or major depression, then the concordance rate rises to 67% in identical twins and 19% in fraternal twins. The relatively low concordance between fraternal twins brought up together suggests that shared family environmental effects are limited, although the ability to detect them has been limited by small sample sizes.
Genetic
Behavioural genetic studies have suggested that many chromosomal regions and candidate genes are related to bipolar disorder susceptibility with each gene exerting a mild to moderate effect. The risk of bipolar disorder is nearly ten-fold higher in first-degree relatives of those with bipolar disorder than in the general population; similarly, the risk of major depressive disorder is three times higher in relatives of those with bipolar disorder than in the general population.
Although the first genetic linkage finding for mania was in 1969, linkage studies have been inconsistent. Findings point strongly to heterogeneity, with different genes implicated in different families. Robust and replicable genome-wide significant associations showed several common single-nucleotide polymorphisms (SNPs) are associated with bipolar disorder, including variants within the genes CACNA1C, ODZ4, and NCAN. The largest and most recent genome-wide association study failed to find any locus that exerts a large effect, reinforcing the idea that no single gene is responsible for bipolar disorder in most cases. Polymorphisms in BDNF, DRD4, DAO, and TPH1 have been frequently associated with bipolar disorder and were initially associated in a meta-analysis, but this association disappeared after correction for multiple testing. On the other hand, two polymorphisms in TPH2 were identified as being associated with bipolar disorder.
Due to the inconsistent findings in a genome-wide association study, multiple studies have undertaken the approach of analysing SNPs in biological pathways. Signalling pathways traditionally associated with bipolar disorder that have been supported by these studies include corticotropin-releasing hormone signalling, cardiac β-adrenergic signalling, Phospholipase C signalling, glutamate receptor signalling, cardiac hypertrophy signalling, Wnt signalling, Notch signalling, and endothelin 1 signalling. Of the 16 genes identified in these pathways, three were found to be dysregulated in the dorsolateral prefrontal cortex portion of the brain in post-mortem studies: CACNA1C, GNG2, and ITPR2.
Bipolar disorder is associated with reduced expression of specific DNA repair enzymes and increased levels of oxidative DNA damages.
Environmental
Psychosocial factors play a significant role in the development and course of bipolar disorder, and individual psychosocial variables may interact with genetic dispositions. Recent life events and interpersonal relationships likely contribute to the onset and recurrence of bipolar mood episodes, just as they do for unipolar depression. In surveys, 30-50% of adults diagnosed with bipolar disorder report traumatic/abusive experiences in childhood, which is associated with earlier onset, a higher rate of suicide attempts, and more co-occurring disorders such as post-traumatic stress disorder. The number of reported stressful events in childhood is higher in those with an adult diagnosis of bipolar spectrum disorder than in those without, particularly events stemming from a harsh environment rather than from the child’s own behaviour. Acutely, mania can be induced by sleep deprivation in around 30% of people with bipolar disorder.
Neurological
Less commonly, bipolar disorder or a bipolar-like disorder may occur as a result of or in association with a neurological condition or injury including stroke, traumatic brain injury, HIV infection, multiple sclerosis, porphyria, and rarely temporal lobe epilepsy.
The precise mechanisms that cause bipolar disorder are not well understood. Bipolar disorder is thought to be associated with abnormalities in the structure and function of certain brain areas responsible for cognitive tasks and the processing of emotions. A neurologic model for bipolar disorder proposes that the emotional circuitry of the brain can be divided into two main parts. The ventral system (regulates emotional perception) includes brain structures such as the amygdala, insula, ventral striatum, ventral anterior cingulate cortex, and the prefrontal cortex. The dorsal system (responsible for emotional regulation) includes the hippocampus, dorsal anterior cingulate cortex, and other parts of the prefrontal cortex. The model hypothesizes that bipolar disorder may occur when the ventral system is overactivated and the dorsal system is underactivated. Other models suggest the ability to regulate emotions is disrupted in people with bipolar disorder and that dysfunction of the ventricular prefrontal cortex (vPFC) is crucial to this disruption.
Brain imaging studies have revealed differences in the volume of various brain regions between patients with bipolar disorder and healthy control subjects.
Meta-analyses of structural MRI studies have shown that certain brain regions (e.g. the left rostral anterior cingulate cortex, fronto-insular cortex, ventral prefrontal cortex, and claustrum) are smaller in people with bipolar disorder, whereas other regions are larger (lateral ventricles, globus pallidus, subgenual anterior cingulate, and the amygdala). Additionally, these meta-analyses found that people with bipolar disorder have higher rates of deep white matter hyperintensities.
Functional MRI findings suggest that the vPFC regulates the limbic system, especially the amygdala. In people with bipolar disorder, decreased vPFC activity allows for the dysregulated activity of the amygdala, which likely contributes to labile mood and poor emotional regulation. Consistent with this, pharmacological treatment of mania returns vPFC activity to the levels in non-manic people, suggesting that vPFC activity is an indicator of mood state. However, while pharmacological treatment of mania reduces amygdala hyperactivity, it remains more active than the amygdala of those without bipolar disorder, suggesting amygdala activity may be a marker of the disorder rather than the current mood state. Manic and depressive episodes tend to be characterised by dysfunction in different regions of the vPFC. Manic episodes appear to be associated with decreased activation of the right vPFC whereas depressive episodes are associated with decreased activation of the left vPFC.
People with bipolar disorder who are in a euthymic mood state show decreased activity in the lingual gyrus compared to people without bipolar disorder. In contrast, they demonstrate decreased activity in the inferior frontal cortex during manic episodes compared to people without the disorder. Similar studies examining the differences in brain activity between people with bipolar disorder and those without did not find a consistent area in the brain that was more or less active when comparing these two groups. People with bipolar have increased activation of left hemisphere ventral limbic areas – which mediate emotional experiences and generation of emotional responses – and decreased activation of right hemisphere cortical structures related to cognition – structures associated with the regulation of emotions.
Neuroscientists have proposed additional models to try to explain the cause of bipolar disorder. One proposed model for bipolar disorder suggests that hypersensitivity of reward circuits consisting of frontostriatal circuits causes mania, and decreased sensitivity of these circuits causes depression. According to the “kindling” hypothesis, when people who are genetically predisposed toward bipolar disorder experience stressful events, the stress threshold at which mood changes occur becomes progressively lower, until the episodes eventually start (and recur) spontaneously. There is evidence supporting an association between early-life stress and dysfunction of the hypothalamic-pituitary-adrenal axis leading to its overactivation, which may play a role in the pathogenesis of bipolar disorder. Other brain components that have been proposed to play a role in bipolar disorder are the mitochondria and a sodium ATPase pump. Circadian rhythms and regulation of the hormone melatonin also seem to be altered.
Dopamine, a neurotransmitter responsible for mood cycling, has increased transmission during the manic phase. The dopamine hypothesis states that the increase in dopamine results in secondary homeostatic downregulation of key system elements and receptors such as lower sensitivity of dopaminergic receptors. This results in decreased dopamine transmission characteristic of the depressive phase. The depressive phase ends with homeostatic upregulation potentially restarting the cycle over again. Glutamate is significantly increased within the left dorsolateral prefrontal cortex during the manic phase of bipolar disorder, and returns to normal levels once the phase is over.
Medications used to treat bipolar may exert their effect by modulating intracellular signalling, such as through depleting myo-inositol levels, inhibition of cAMP signalling, and through altering subunits of the dopamine-associated G-protein. Consistent with this, elevated levels of Gαi, Gαs, and Gαq/11 have been reported in brain and blood samples, along with increased protein kinase A (PKA) expression and sensitivity; typically, PKA activates as part of the intracellular signalling cascade downstream from the detachment of Gαs subunit from the G protein complex.
Decreased levels of 5-hydroxyindoleacetic acid, a byproduct of serotonin, are present in the cerebrospinal fluid of persons with bipolar disorder during both the depressed and manic phases. Increased dopaminergic activity has been hypothesized in manic states due to the ability of dopamine agonists to stimulate mania in people with bipolar disorder. Decreased sensitivity of regulatory α2 adrenergic receptors as well as increased cell counts in the locus coeruleus indicated increased noradrenergic activity in manic people. Low plasma GABA levels on both sides of the mood spectrum have been found. One review found no difference in monoamine levels, but found abnormal norepinephrine turnover in people with bipolar disorder. Tyrosine depletion was found to reduce the effects of methamphetamine in people with bipolar disorder as well as symptoms of mania, implicating dopamine in mania. VMAT2 binding was found to be increased in one study of people with bipolar mania.
Diagnosis
Bipolar disorder is commonly diagnosed during adolescence or early adulthood, but onset can occur throughout life. Its diagnosis is based on the self-reported experiences of the individual, abnormal behaviour reported by family members, friends or co-workers, observable signs of illness as assessed by a clinician, and ideally a medical work-up to rule out other causes. Caregiver-scored rating scales, specifically from the mother, have shown to be more accurate than teacher and youth-scored reports in identifying youths with bipolar disorder. Assessment is usually done on an outpatient basis; admission to an inpatient facility is considered if there is a risk to oneself or others.
The most widely used criteria for diagnosing bipolar disorder are from the American Psychiatric Association’s (APA) Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) and the World Health Organisation’s (WHO) International Statistical Classification of Diseases and Related Health Problems, 10th Edition (ICD-10). The ICD-10 criteria are used more often in clinical settings outside of the US while the DSM criteria are used within the US and are the prevailing criteria used internationally in research studies. The DSM-5, published in 2013, includes further and more accurate specifiers compared to its predecessor, the DSM-IV-TR. This work has influenced the upcoming eleventh revision of the ICD, which includes the various diagnoses within the bipolar spectrum of the DSM-V.
Several rating scales for the screening and evaluation of bipolar disorder exist, including the Bipolar spectrum diagnostic scale (BSDS), Mood Disorder Questionnaire (MDQ), the General Behaviour Inventory (GBI) and the Hypomania Checklist. The use of evaluation scales cannot substitute a full clinical interview but they serve to systematise the recollection of symptoms. On the other hand, instruments for screening bipolar disorder tend to have lower sensitivity.
Differential Diagnosis
Bipolar disorder is classified by the International Classification of Diseases as a mental and behavioural disorder. Mental disorders that can have symptoms similar to those seen in bipolar disorder include schizophrenia, major depressive disorder, attention deficit hyperactivity disorder (ADHD), and certain personality disorders, such as borderline personality disorder. A key difference between bipolar disorder and borderline personality disorder is the nature of the mood swings; in contrast to the sustained changes to mood over days to weeks or longer, those of the latter condition (more accurately called emotional dysregulation) are sudden and often short-lived, and secondary to social stressors.
Although there are no biological tests that are diagnostic of bipolar disorder, blood tests and/or imaging are carried out to investigate whether medical illnesses with clinical presentations similar to that of bipolar disorder are present before making a definitive diagnosis. Neurologic diseases such as multiple sclerosis, complex partial seizures, strokes, brain tumours, Wilson’s disease, traumatic brain injury, Huntington’s disease, and complex migraines can mimic features of bipolar disorder. An EEG may be used to exclude neurological disorders such as epilepsy, and a CT scan or MRI of the head may be used to exclude brain lesions. Additionally, disorders of the endocrine system such as hypothyroidism, hyperthyroidism, and Cushing’s disease are in the differential as is the connective tissue disease systemic lupus erythematosus. Infectious causes of mania that may appear similar to bipolar mania include herpes encephalitis, HIV, influenza, or neurosyphilis. Certain vitamin deficiencies such as pellagra (niacin deficiency), Vitamin B12 deficiency, folate deficiency, and Wernicke Korsakoff syndrome (thiamine deficiency) can also lead to mania. Common medications that can cause manic symptoms include antidepressants, prednisone, Parkinson’s disease medications, thyroid hormone, stimulants (including cocaine and methamphetamine), and certain antibiotics.
Bipolar Spectrum
Bipolar spectrum disorders include: bipolar I disorder, bipolar II disorder, cyclothymic disorder and cases where subthreshold symptoms are found to cause clinically significant impairment or distress. These disorders involve major depressive episodes that alternate with manic or hypomanic episodes, or with mixed episodes that feature symptoms of both mood states. The concept of the bipolar spectrum is similar to that of Emil Kraepelin’s original concept of manic depressive illness. Bipolar II disorder was established as a diagnosis in 1994 within DSM IV; though debate continues over whether it is a distinct entity, part of a spectrum, or exists at all.
Criteria and Subtypes
The DSM and the ICD characterise bipolar disorder as a spectrum of disorders occurring on a continuum. The DSM-5 and ICD-11 lists three specific subtypes:
Type
Description
Bipolar I Disorder
1. At least one manic episode is necessary to make the diagnosis; depressive episodes are common in the vast majority of cases with bipolar disorder I, but are unnecessary for the diagnosis. 2. Specifiers such as “mild, moderate, moderate-severe, severe” and “with psychotic features” should be added as applicable to indicate the presentation and course of the disorder.
Bipolar II Disorder
1. No manic episodes and one or more hypomanic episodes and one or more major depressive episodes. 2. Hypomanic episodes do not go to the full extremes of mania (i.e. do not usually cause severe social or occupational impairment, and are without psychosis). 3. This can make bipolar II more difficult to diagnose, since the hypomanic episodes may simply appear as periods of successful high productivity and are reported less frequently than a distressing, crippling depression.
Cyclothymia
A history of hypomanic episodes with periods of depression that do not meet criteria for major depressive episodes.
When relevant, specifiers for peripartum onset and with rapid cycling should be used with any subtype. Individuals who have subthreshold symptoms that cause clinically significant distress or impairment, but do not meet full criteria for one of the three subtypes may be diagnosed with other specified or unspecified bipolar disorder. Other specified bipolar disorder is used when a clinician chooses to explain why the full criteria were not met (e.g. hypomania without a prior major depressive episode). If the condition is thought to have a non-psychiatric medical cause, the diagnosis of bipolar and related disorder due to another medical condition is made, while substance/medication-induced bipolar and related disorder is used if a medication is thought to have triggered the condition.
Rapid Cycling
Most people who meet criteria for bipolar disorder experience a number of episodes, on average 0.4 to 0.7 per year, lasting three to six months. Rapid cycling, however, is a course specifier that may be applied to any bipolar subtype. It is defined as having four or more mood disturbance episodes within a one-year span. Rapid cycling is usually temporary but is common amongst people with bipolar disorder and affects between 25.8%-45.3% of them at some point in their life. These episodes are separated from each other by a remission (partial or full) for at least two months or a switch in mood polarity (i.e. from a depressive episode to a manic episode or vice versa). The definition of rapid cycling most frequently cited in the literature (including the DSM-V and ICD-11) is that of Dunner and Fieve: at least four major depressive, manic, hypomanic or mixed episodes during a 12-month period. The literature examining the pharmacological treatment of rapid cycling is sparse and there is no clear consensus with respect to its optimal pharmacological management. People with the rapid cycling or ultradian subtypes of bipolar disorder tend to be more difficult to treat and less responsive to medications than other people with bipolar disorder.
Children
Refer to Bipolar Disorder in Children.
In the 1920s, Kraepelin noted that manic episodes are rare before puberty. In general, bipolar disorder in children was not recognised in the first half of the twentieth century. This issue diminished with an increased following of the DSM criteria in the last part of the twentieth century. The diagnosis of childhood bipolar disorder, while formerly controversial, has gained greater acceptance among childhood and adolescent psychiatrists. American children and adolescents diagnosed with bipolar disorder in community hospitals increased 4-fold reaching rates of up to 40% in 10 years around the beginning of the 21st century, while in outpatient clinics it doubled reaching 6%. Studies using DSM criteria show that up to 1% of youth may have bipolar disorder. The DSM-5 has established a diagnosis – disruptive mood dysregulation disorder – that covers children with long-term, persistent irritability that had at times been misdiagnosed as having bipolar disorder, distinct from irritability in bipolar disorder that is restricted to discrete mood episodes.
Elderly
Bipolar disorder is uncommon in older patients, with a measured lifetime prevalence of 1% in over 60s and a 12-month prevalence of 0.1 to 0.5% in people over 65. Despite this, it is overrepresented in psychiatric admissions, making up 4 to 8% of inpatient admission to aged care psychiatry units, and the incidence of mood disorders is increasing overall with the aging population. Depressive episodes more commonly present with sleep disturbance, fatigue, hopelessness about the future, slowed thinking, and poor concentration and memory; the last three symptoms are seen in what is known as pseudodementia. Clinical features also differ between those with late-onset bipolar disorder and those who developed it early in life; the former group present with milder manic episodes, more prominent cognitive changes and have a background of worse psychosocial functioning, while the latter present more commonly with mixed affective episodes, and have a stronger family history of illness. Older people with bipolar disorder suffer cognitive changes, particularly in executive functions such as abstract thinking and switching cognitive sets, as well as concentrating for long periods and decision-making.
Prevention
Attempts at prevention of bipolar disorder have focused on stress (such as childhood adversity or highly conflictual families) which, although not a diagnostically specific causal agent for bipolar, does place genetically and biologically vulnerable individuals at risk for a more severe course of illness. Longitudinal studies have indicated that full-blown manic stages are often preceded by a variety of prodromal clinical features, providing support for the occurrence of an at-risk state of the disorder when an early intervention might prevent its further development and/or improve its outcome.
Management
The aim of management is to treat acute episodes safely with medication and work with the patient in long-term maintenance to prevent further episodes and optimise function using a combination of pharmacological and psychotherapeutic techniques. Hospitalisation may be required especially with the manic episodes present in bipolar I. This can be voluntary or (local legislation permitting) involuntary. Long-term inpatient stays are now less common due to deinstitutionalisation, although these can still occur. Following (or in lieu of) a hospital admission, support services available can include drop-in centres, visits from members of a community mental health team or an Assertive Community Treatment team, supported employment, patient-led support groups, and intensive outpatient programmes (IOP). These are sometimes referred to as partial-inpatient programmes.
Psychosocial
Psychotherapy aims to assist a person with bipolar disorder in accepting and understanding their diagnosis, coping with various types of stress, improving their interpersonal relationships, and recognising prodromal symptoms before full-blown recurrence. Cognitive behavioural therapy, family-focused therapy, and psychoeducation have the most evidence for efficacy in regard to relapse prevention, while interpersonal and social rhythm therapy and cognitive-behavioural therapy appear the most effective in regard to residual depressive symptoms. Most studies have been based only on bipolar I, however, and treatment during the acute phase can be a particular challenge. Some clinicians emphasize the need to talk with individuals experiencing mania, to develop a therapeutic alliance in support of recovery.
Medication
Medications may differ depending on what episode is being treated. The medication with the best overall evidence is lithium, which is an effective treatment for acute manic episodes, preventing relapses, and bipolar depression. Lithium reduces the risk of suicide, self-harm, and death in people with bipolar disorder. Antipsychotics and mood stabilisers used together are quicker and more effective at treating mania than either class of drug used alone. Some analyses indicate antipsychotics alone are also more effective at treating acute mania. Mood stabilisers are used for long-term maintenance but have not demonstrated the ability to quickly treat acute bipolar depression. It is unclear if ketamine (a common general dissociative anaesthetic used in surgery) is useful in bipolar disorder.
Mood Stabilisers
Lithium and the anticonvulsants carbamazepine, lamotrigine, and valproic acid are classed as mood stabilisers due to their effect on the mood states in bipolar disorder. Lithium is preferred for long-term mood stabilisation, although it erodes kidney and thyroid function over extended periods. Valproate has become a commonly prescribed treatment and effectively treats manic episodes. Carbamazepine is less effective in preventing relapse than lithium or valproate. Lamotrigine has some efficacy in treating depression, and this benefit is greatest in more severe depression. It has also been shown to have some benefit in preventing bipolar disorder relapses, though there are concerns about the studies done, and is of no benefit in rapid cycling subtype of bipolar disorder. Valproate and carbamazepine are teratogenic and should be avoided as a treatment in women of childbearing age, but discontinuation of these medications during pregnancy is associated with a high risk of relapse. The effectiveness of topiramate is unknown. Carbamazepine effectively treats manic episodes, with some evidence it has greater benefit in rapid-cycling bipolar disorder, or those with more psychotic symptoms or more symptoms similar to that of schizoaffective disorder.
Antipsychotics
Antipsychotic medications are effective for short-term treatment of bipolar manic episodes and appear to be superior to lithium and anticonvulsants for this purpose. Atypical antipsychotics are also indicated for bipolar depression refractory to treatment with mood stabilisers. Olanzapine is effective in preventing relapses, although the supporting evidence is weaker than the evidence for lithium. A 2006 review found that haloperidol was an effective treatment for acute mania, limited data supported no difference in overall efficacy between haloperidol, olanzapine or risperidone, and that it could be less effective than aripiprazole.
Antidepressants
Antidepressants are not recommended for use alone in the treatment of bipolar disorder and do not provide any benefit over mood stabilisers. Atypical antipsychotic medications (e.g. aripiprazole) are preferred over antidepressants to augment the effects of mood stabilisers due to the lack of efficacy of antidepressants in bipolar disorder. Treatment of bipolar disorder using antidepressants carries a risk of affective switches; where a person switches from depression to manic or hypomanic phases. The risk of affective switches is higher in bipolar I depression; antidepressants are generally avoided in bipolar I disorder or only used with mood stabilisers when they are deemed necessary. There is also a risk of accelerating cycling between phases when antidepressants are used in bipolar disorder.
Other Drugs
Short courses of benzodiazepines are used in addition to other medications for calming effect until mood stabilising become effective. Electroconvulsive therapy (ECT) is an effective form of treatment for acute mood disturbances in those with bipolar disorder, especially when psychotic or catatonic features are displayed. ECT is also recommended for use in pregnant women with bipolar disorder.
Children
Treating bipolar disorder in children involves medication and psychotherapy. The literature and research on the effects of psychosocial therapy on bipolar spectrum disorders are scarce, making it difficult to determine the efficacy of various therapies. Mood stabilisers and atypical antipsychotics are commonly prescribed. Among the former, lithium is the only compound approved by the US Food and Drug Administration (FDA) for children. Psychological treatment combines normally education on the disease, group therapy, and cognitive behavioural therapy. Long-term medication is often needed.
Resistance to Treatment
The occurrence of poor response to treatment in has given support to the concept of resistance to treatment in bipolar disorder. Guidelines to the definition of such treatment resistance and evidence-based options for its management were reviewed in 2020.
Prognosis
A lifelong condition with periods of partial or full recovery in between recurrent episodes of relapse, bipolar disorder is considered to be a major health problem worldwide because of the increased rates of disability and premature mortality. It is also associated with co-occurring psychiatric and medical problems, higher rates of death from natural causes (e.g. cardiovascular disease), and high rates of initial under- or misdiagnosis, causing a delay in appropriate treatment and contributing to poorer prognoses. When compared to the general population, people with bipolar disorder also have higher rates of other serious medical comorbidities including diabetes mellitus, respiratory diseases, HIV, and Hepatitis C virus infection. After a diagnosis is made, it remains difficult to achieve complete remission of all symptoms with the currently available psychiatric medications and symptoms often become progressively more severe over time.
Compliance with medications is one of the most significant factors that can decrease the rate and severity of relapse and have a positive impact on overall prognosis. However, the types of medications used in treating BD commonly cause side effects and more than 75% of individuals with BD inconsistently take their medications for various reasons. Of the various types of the disorder, rapid cycling (four or more episodes in one year) is associated with the worst prognosis due to higher rates of self-harm and suicide. Individuals diagnosed with bipolar who have a family history of bipolar disorder are at a greater risk for more frequent manic/hypomanic episodes. Early onset and psychotic features are also associated with worse outcomes, as well as subtypes that are nonresponsive to lithium.
Early recognition and intervention also improve prognosis as the symptoms in earlier stages are less severe and more responsive to treatment. Onset after adolescence is connected to better prognoses for both genders, and being male is a protective factor against higher levels of depression. For women, better social functioning before developing bipolar disorder and being a parent are protective towards suicide attempts.
Functioning
Changes in cognitive processes and abilities are seen in mood disorders, with those of bipolar disorder being greater than those in major depressive disorder. These include reduced attentional and executive capabilities and impaired memory. People with bipolar disorder often experience a decline in cognitive functioning during (or possibly before) their first episode, after which a certain degree of cognitive dysfunction typically becomes permanent, with more severe impairment during acute phases and moderate impairment during periods of remission. As a result, two-thirds of people with BD continue to experience impaired psychosocial functioning in between episodes even when their mood symptoms are in full remission. A similar pattern is seen in both BD-I and BD-II, but people with BD-II experience a lesser degree of impairment.
When bipolar disorder occurs in children, it severely and adversely affects their psychosocial development. Children and adolescents with bipolar disorder have higher rates of significant difficulties with substance abuse, psychosis, academic difficulties, behavioural problems, social difficulties, and legal problems. Cognitive deficits typically increase over the course of the illness. Higher degrees of impairment correlate with the number of previous manic episodes and hospitalisations, and with the presence of psychotic symptoms. Early intervention can slow the progression of cognitive impairment, while treatment at later stages can help reduce distress and negative consequences related to cognitive dysfunction.
Despite the overly ambitious goals that are frequently part of manic episodes, symptoms of mania undermine the ability to achieve these goals and often interfere with an individual’s social and occupational functioning. One-third of people with BD remain unemployed for one year following a hospitalisation for mania. Depressive symptoms during and between episodes, which occur much more frequently for most people than hypomanic or manic symptoms over the course of illness, are associated with lower functional recovery in between episodes, including unemployment or underemployment for both BD-I and BD-II. However, the course of illness (duration, age of onset, number of hospitalisations, and the presence or not of rapid cycling) and cognitive performance are the best predictors of employment outcomes in individuals with bipolar disorder, followed by symptoms of depression and years of education.
Recovery and Recurrence
A naturalistic study in 2003 by Tohen and coworkers from the first admission for mania or mixed episode (representing the hospitalised and therefore most severe cases) found that 50% achieved syndromal recovery (no longer meeting criteria for the diagnosis) within six weeks and 98% within two years. Within two years, 72% achieved symptomatic recovery (no symptoms at all) and 43% achieved functional recovery (regaining of prior occupational and residential status). However, 40% went on to experience a new episode of mania or depression within 2 years of syndromal recovery, and 19% switched phases without recovery.
Symptoms preceding a relapse (prodromal), especially those related to mania, can be reliably identified by people with bipolar disorder. There have been intents to teach patients coping strategies when noticing such symptoms with encouraging results.
Suicide
Bipolar disorder can cause suicidal ideation that leads to suicide attempts. Individuals whose bipolar disorder begins with a depressive or mixed affective episode seem to have a poorer prognosis and an increased risk of suicide. One out of two people with bipolar disorder attempt suicide at least once during their lifetime and many attempts are successfully completed. The annual average suicide rate is 0.4%, which is 10-20 times that of the general population. The number of deaths from suicide in bipolar disorder is between 18 and 25 times higher than would be expected in similarly aged people without bipolar disorder. The lifetime risk of suicide has been estimated to be as high as 20% in those with bipolar disorder.
Risk factors for suicide attempts and death from suicide in people with bipolar disorder include older age, prior suicide attempts, a depressive or mixed index episode (first episode), a manic index episode with psychotic symptoms, hopelessness or psychomotor agitation present during the episodes, co-existing anxiety disorder, a first degree relative with a mood disorder or suicide, interpersonal conflicts, occupational problems, bereavement or social isolation.
Epidemiology
Bipolar disorder is the sixth leading cause of disability worldwide and has a lifetime prevalence of about 1 to 3% in the general population. However, a reanalysis of data from the National Epidemiological Catchment Area survey in the United States suggested that 0.8% of the population experience a manic episode at least once (the diagnostic threshold for bipolar I) and a further 0.5% have a hypomanic episode (the diagnostic threshold for bipolar II or cyclothymia). Including sub-threshold diagnostic criteria, such as one or two symptoms over a short time-period, an additional 5.1% of the population, adding up to a total of 6.4%, were classified as having a bipolar spectrum disorder. A more recent analysis of data from a second US National Comorbidity Survey found that 1% met lifetime prevalence criteria for bipolar I, 1.1% for bipolar II, and 2.4% for subthreshold symptoms. Estimates vary about how many children and young adults have bipolar disorder. These estimates range from 0.6 to 15% depending on differing settings, methods, and referral settings, raising suspicions of overdiagnosis. One meta-analysis of bipolar disorder in young people worldwide estimated that about 1.8% of people between the ages of seven and 21 have bipolar disorder. Similar to adults, bipolar disorder in children and adolescents is thought to occur at a similar frequency in boys and girls.
There are conceptual and methodological limitations and variations in the findings. Prevalence studies of bipolar disorder are typically carried out by lay interviewers who follow fully structured/fixed interview schemes; responses to single items from such interviews may suffer limited validity. In addition, diagnoses (and therefore estimates of prevalence) vary depending on whether a categorical or spectrum approach is used. This consideration has led to concerns about the potential for both under-diagnosis and overdiagnosis.
The incidence of bipolar disorder is similar in men and women as well as across different cultures and ethnic groups. A 2000 study by the World Health Organisation found that prevalence and incidence of bipolar disorder are very similar across the world. Age-standardised prevalence per 100,000 ranged from 421.0 in South Asia to 481.7 in Africa and Europe for men and from 450.3 in Africa and Europe to 491.6 in Oceania for women. However, severity may differ widely across the globe. Disability-adjusted life year rates, for example, appear to be higher in developing countries, where medical coverage may be poorer and medication less available. Within the United States, Asian Americans have significantly lower rates than their African American and European American counterparts. In 2017, the Global Burden of Disease Study estimated there were 4.5 million new cases and a total of 45.5 million cases globally.
Society and Culture
Cost
The United States spent approximately $202.1 billion on people diagnosed with bipolar I disorder (excluding other subtypes of bipolar disorder and undiagnosed people) in 2015. One analysis estimated that the United Kingdom spent approximately £5.2 billion on the disorder in 2007. In addition to the economic costs, bipolar disorder is a leading cause of disability and lost productivity worldwide. People with bipolar disorder are generally more disabled, have a lower level of functioning, longer duration of illness, and increased rates of work absenteeism and decreased productivity when compared to people experiencing other mental health disorders. The decrease in the productivity seen in those who care for people with bipolar disorder also significantly contributes to these costs.
Advocacy
There are widespread issues with social stigma, stereotypes, and prejudice against individuals with a diagnosis of bipolar disorder. In 2000, actress Carrie Fisher went public with her bipolar disorder diagnosis. She became one of the most well-recognized advocates for people with bipolar disorder in the public eye and fiercely advocated to eliminate the stigma surrounding mental illnesses, including bipolar disorder. Stephen Fried, who has written extensively on the topic, noted that Fisher helped to draw attention to the disorder’s chronicity, relapsing nature, and that bipolar disorder relapses do not indicate a lack of discipline or moral shortcomings. Since being diagnosed at age 37, actor Stephen Fry has pushed to raise awareness of the condition, with his 2006 documentary Stephen Fry: The Secret Life of the Manic Depressive. In an effort to ease the social stigma associated with bipolar disorder, the orchestra conductor Ronald Braunstein cofounded the ME/2 Orchestra with his wife Caroline Whiddon in 2011. Braunstein was diagnosed with bipolar disorder in 1985 and his concerts with the ME/2 Orchestra were conceived in order to create a welcoming performance environment for his musical colleagues, while also raising public awareness about mental illness.
Notable Cases
Numerous authors have written about bipolar disorder and many successful people have openly discussed their experience with it. Kay Redfield Jamison, a clinical psychologist and professor of psychiatry at the Johns Hopkins University School of Medicine, profiled her own bipolar disorder in her memoir An Unquiet Mind (1995). Several celebrities have also publicly shared that they have bipolar disorder; in addition to Carrie Fisher and Stephen Fry these include Catherine Zeta-Jones, Mariah Carey, Kanye West, Jane Pauley, Demi Lovato, and Selena Gomez.
Media Portrayals
Several dramatic works have portrayed characters with traits suggestive of the diagnosis which have been the subject of discussion by psychiatrists and film experts alike.
In Mr. Jones (1993), (Richard Gere) swings from a manic episode into a depressive phase and back again, spending time in a psychiatric hospital and displaying many of the features of the syndrome. In The Mosquito Coast (1986), Allie Fox (Harrison Ford) displays some features including recklessness, grandiosity, increased goal-directed activity and mood lability, as well as some paranoia. Psychiatrists have suggested that Willy Loman, the main character in Arthur Miller’s classic play Death of a Salesman, has bipolar disorder.
The 2009 drama 90210 featured a character, Silver, who was diagnosed with bipolar disorder. Stacey Slater, a character from the BBC soap EastEnders, has been diagnosed with the disorder. The storyline was developed as part of the BBC’s Headroom campaign.[198] The Channel 4 soap Brookside had earlier featured a story about bipolar disorder when the character Jimmy Corkhill was diagnosed with the condition. 2011 Showtime’s political thriller drama Homeland protagonist Carrie Mathison has bipolar disorder, which she has kept secret since her school days. The 2014 ABC medical drama, Black Box, featured a world-renowned neuroscientist with bipolar disorder. In the TV series Dave, the eponymous main character, played by Lil Dicky as a fictionalised version of himself, is an aspiring rapper. Lil Dicky’s real-life hype man GaTa also plays himself. In one episode, after being off his medication and having an episode, GaTa tearfully confesses to having bipolar disorder. GaTa has bipolar disorder in real life but, like his character in the show, he is able to manage it with medication.
Creativity
A link between mental illness and professional success or creativity has been suggested, including in accounts by Socrates, Seneca the Younger, and Cesare Lombroso. Despite prominence in popular culture, the link between creativity and bipolar has not been rigorously studied. This area of study also is likely affected by confirmation bias. Some evidence suggests that some heritable component of bipolar disorder overlaps with heritable components of creativity. Probands of people with bipolar disorder are more likely to be professionally successful, as well as to demonstrate temperamental traits similar to bipolar disorder. Furthermore, while studies of the frequency of bipolar disorder in creative population samples have been conflicting, full-blown bipolar disorder in creative samples is rare.
Research
Research directions for bipolar disorder in children include optimising treatments, increasing the knowledge of the genetic and neurobiological basis of the paediatric disorder and improving diagnostic criteria. Some treatment research suggests that psychosocial interventions that involve the family, psychoeducation, and skills building (through therapies such as CBT, DBT, and IPSRT) can benefit in addition to pharmocotherapy.
An intensive outpatient programme (IOP) is a kind of treatment service and support programme used primarily to treat eating disorders, bipolar disorder (including mania; and for Bipolar I and Bipolar II), unipolar depression, self harm and chemical dependency that does not rely on detoxification.
IOP operates on a small scale and does not require the intensive residential or partial day services typically offered by the larger, more comprehensive treatment facilities.
The typical IOP programme offers group therapy and generally facilitates 6-30 hours a week of programming for addiction treatment. IOP allows the individual to be able to participate in their daily affairs, such as work, and then participate in treatment at an appropriate facility in the morning or at the end of the day. With an IOP, classes, sessions, meetings, and workshops are scheduled throughout the day, and individuals are expected to adhere to the strict structure of the program. Online IOP has shown to be effective, as well.
The typical IOP programme encourages active participation in 12-step programmes in addition to IOP participation. IOP can be more effective than individual therapy for chemical dependency.
IOP is also used by some HMOs as transitional treatment for patients just released from treatment in a psychiatric ward.
The Mood Disorder Questionnaire (MDQ) is a self-report questionnaire designed to help detect bipolar disorder.
It focuses on symptoms of hypomania and mania, which are the mood states that separate bipolar disorders from other types of depression and mood disorder. It has 5 main questions, and the first question has 13 parts, for a total of 17 questions. The MDQ was originally tested with adults, but it also has been studied in adolescents ages 11 years and above. It takes approximately 5-10 minutes to complete. In 2006, a parent-report version was created to allow for assessment of bipolar symptoms in children or adolescents from a caregiver perspective, with the research looking at youths as young as 5 years old.
The MDQ has become one of the most widely studied and used questionnaires for bipolar disorder, and it has been translated into more than a dozen languages.
Development
The MDQ was developed as a screening tool for bipolar disorder, and assesses symptoms of mania and hypomania It was developed in the hopes that it would reduce the mis-diagnosis and delayed diagnosis of bipolar disorder. The first 13 items on the measure ask about any manic/hypomanic symptoms that may have occurred during one’s lifetime. These items are based on the DSM-IV criteria for bipolar disorder. Additional items then ask if these symptoms have happened during the same period of time (an “episode”), and how severely these symptoms affected functioning (assessing impairment).
In developing this tool, the MDQ was administered to a group of bipolar patients to assess feasibility and face validity, leading to revision of the items. Following this initial study, researchers have assessed psychometric properties of the MDQ, finding that the measure possesses adequate internal consistency. The measure has also demonstrated fair sensitivity in several studies, although sensitivity may be greater in inpatient versus community settings. First built for use in adults, it has been translated into many languages and tested in a range of different settings. Researchers also have studied whether parents could use this to provide useful information about their child or adolescent. Meta-analyses have found that the MDQ is one of the best self-report tools for assessing hypomania or mania in adults, and the parent report version is one of the three best options available for parents to use about their children.
Limitations
One limitation of the MDQ is that it has shown higher sensitivity when detecting bipolar I compared to other bipolar spectrum disorders. It is much less sensitive to bipolar II, often missing more than half of the cases with this diagnosis when using the recommended algorithm. Additionally, the sensitivity and specificity of the MDQ has been shown to differ by the use of a standard vs. modified cutoff (i.e. simplifies the cutoff to be based only on symptom endorsement, rather than impairment). Sensitivity and specificity of the MDQ also depend on study inclusion and exclusion criteria. Including more severe cases will increase the apparent sensitivity, because it is more likely that they will have high scores. Including healthy controls or people who are not seeking services will exaggerate the specificity of the test, as these individuals are unlikely to have manic symptoms and will score very low on the measure as a result.
Another major limitation of the MDQ is that it is not to be sensitive to treatment effects. It asks about lifetime history of symptoms, which is a strength for screening and detection, but a weakness for measuring the current severity of mood symptoms. The MDQ also uses a yes/no format for the symptoms, rather than asking about the severity of each. Other rating scales are more useful for measuring severity and treatment outcomes.
Additionally, self-report measures have some disadvantages, including bias that can stem from social desirability and demand characteristics.
The Bipolar Spectrum Diagnostic Scale (BSDS) is a psychiatric screening rating scale for bipolar disorder.
Background
It was developed by Ronald Pies, and was later refined and tested by S. Nassir Ghaemi and colleagues. The BSDS arose from Pies’s experience as a psychopharmacology consultant, where he was frequently called on to manage cases of “treatment-resistant depression”. Patients are typically diagnosed during their 20s. The lifetime prevalence of BD is approximately 1%, rising to 4% if a broader definition of bipolar spectrum disorder is used.
The English version of the scale consists of 19 question items and two sections. It differs from most scales in that it does not list separate items, but rather presents a short paragraph talking about experiences that people with bipolar spectrum disorders often have. The person checks off which phrases or experiences fit them. Bipolar spectrum disorder includes bipolar I and bipolar II, and other cases not meeting criteria for those disorders.
The scale was validated in its original version and demonstrated high diagnostic sensitivity, meaning that most people with confirmed bipolar diagnoses scored high on the BSDS. The BSDS may do better than other scales at detecting types of bipolar disorder that do not involve a full manic episode, such as bipolar II or cyclothymic disorder.
It is taken either by mouth or by injection into a muscle. The injectable version is long-acting and lasts for about two weeks.
Common side effects include movement problems, sleepiness, dizziness, trouble seeing, constipation, and increased weight. Serious side effects may include the potentially permanent movement disorder tardive dyskinesia, as well as neuroleptic malignant syndrome, an increased risk of suicide, and high blood sugar levels. In older people with psychosis as a result of dementia, it may increase the risk of dying. It is unknown if it is safe for use in pregnancy. Its mechanism of action is not entirely clear, but is believed to be related to its action as a dopamine and serotonin antagonist.
Study of risperidone began in the late 1980s and it was approved for sale in the United States in 1993. It is on the World Health Organisation’s List of Essential Medicines. It is available as a generic medication. In 2018, it was the 159th most commonly prescribed medication in the United States, with more than 3 million prescriptions.
Medical Uses
Risperidone is mainly used for the treatment of schizophrenia, bipolar disorder, and irritability associated with autism.
Schizophrenia
Risperidone is effective in treating psychogenic polydipsia and the acute exacerbations of schizophrenia.
Studies evaluating the utility of risperidone by mouth for maintenance therapy have reached varying conclusions. A 2012 systematic review concluded that evidence is strong that risperidone is more effective than all first-generation antipsychotics other than haloperidol, but that evidence directly supporting its superiority to placebo is equivocal. A 2011 review concluded that risperidone is more effective in relapse prevention than other first- and second-generation antipsychotics with the exception of olanzapine and clozapine. A 2016 Cochrane review suggests that risperidone reduces the overall symptoms of schizophrenia, but firm conclusions are difficult to make due to very low-quality evidence. Data and information are scarce, poorly reported, and probably biased in favour of risperidone, with about half of the included trials developed by drug companies. The article raises concerns regarding the serious side effects of risperidone, such as parkinsonism.
Long-acting injectable formulations of antipsychotic drugs provide improved compliance with therapy and reduce relapse rates relative to oral formulations. The efficacy of risperidone long-acting injection appears to be similar to that of long acting injectable forms of first generation antipsychotics.
Bipolar Disorder
Second-generation antipsychotics, including risperidone, are effective in the treatment of manic symptoms in acute manic or mixed exacerbations of bipolar disorder. In children and adolescents, risperidone may be more effective than lithium or divalproex, but has more metabolic side effects. As maintenance therapy, long-acting injectable risperidone is effective for the prevention of manic episodes but not depressive episodes. The long-acting injectable form of risperidone may be advantageous over long acting first generation antipsychotics, as it is better tolerated (fewer extrapyramidal effects) and because long acting injectable formulations of first generation antipsychotics may increase the risk of depression.
Autism
Compared to placebo, risperidone treatment reduces certain problematic behaviours in autistic children, including aggression toward others, self-injury, challenging behaviour, and rapid mood changes. The evidence for its efficacy appears to be greater than that for alternative pharmacological treatments. Weight gain is an important adverse effect. Some authors recommend limiting the use of risperidone and aripiprazole to those with the most challenging behavioural disturbances in order to minimise the risk of drug-induced adverse effects. Evidence for the efficacy of risperidone in autistic adolescents and young adults is less persuasive.
Other Uses
Risperidone has shown promise in treating therapy-resistant obsessive-compulsive disorder, when serotonin reuptake inhibitors are not sufficient.
While antipsychotic medications such as risperidone have a slight benefit in people with dementia, they have been linked to higher incidences of death and stroke. Because of this increased risk of death, treatment of dementia-related psychosis with risperidone is not US Drug and Food Administration (FDA) approved.
Forms
Available forms of risperidone include tablet, oral dissolving tablet, oral solution, and powder and solvent for suspension for injection.
Adverse Effects
Common side effects include movement problems, sleepiness, dizziness, trouble seeing, constipation, and increased weight. About 9 to 20% of people gained more than 7% of the baseline weight depending on the dose. Serious side effects may include the potentially permanent movement disorder tardive dyskinesia, as well as neuroleptic malignant syndrome, an increased risk of suicide, and high blood sugar levels. In older people with psychosis as a result of dementia, it may increase the risk of dying.
While atypical antipsychotics appear to have a lower rate of movement problems as compared to typical antipsychotics, risperidone has a high risk of movement problems among the atypicals. Atypical antipsychotics however are associated with a greater amount of weight gain.
Drug Interactions
Carbamazepine and other enzyme inducers may reduce plasma levels of risperidone.
If a person is taking both carbamazepine and risperidone, the dose of risperidone will likely need to be increased.
The new dose should not be more than twice the patient’s original dose.
CYP2D6 inhibitors, such as SSRI medications, may increase plasma levels of risperidone and those medications.
Since risperidone can cause hypotension, its use should be monitored closely when a patient is also taking antihypertensive medicines to avoid severe low blood pressure.
Risperidone and its metabolite paliperidone are reduced in efficacy by P-glycoprotein inducers such as St John’s wort.
Discontinuation
The British National Formulary recommends a gradual withdrawal when discontinuing antipsychotic treatment to avoid acute withdrawal syndrome or rapid relapse. Some have argued the additional somatic and psychiatric symptoms associated with dopaminergic super-sensitivity, including dyskinesia and acute psychosis, are common features of withdrawal in individuals treated with neuroleptics. This has led some to suggest the withdrawal process might itself be schizomimetic, producing schizophrenia-like symptoms even in previously healthy patients, indicating a possible pharmacological origin of mental illness in a yet unknown percentage of patients currently and previously treated with antipsychotics. This question is unresolved, and remains a highly controversial issue among professionals in the medical and mental health communities, as well as the public.
Dementia
Older people with dementia-related psychosis are at a higher risk of death if they take risperidone compared to those who do not. Most deaths are related to heart problems or infections.
Pharmacology
Pharmacodynamics
Risperidone has been classified as a “qualitatively atypical” antipsychotic agent with a relatively low incidence of extrapyramidal side effects (when given at low doses) that has more pronounced serotonin antagonism than dopamine antagonism. Risperidone contains the functional groups of benzisoxazole and piperidine as part of its molecular structure. Although not a butyrophenone, it was developed with the structures of benperidol and ketanserin as a basis. It has actions at several 5-HT (serotonin) receptor subtypes. These are 5-HT2C, linked to weight gain, 5-HT2A, linked to its antipsychotic action and relief of some of the extrapyramidal side effects experienced with the typical neuroleptics.[46]
It was recently found that D-amino acid oxidase, the enzyme that catalyses the breakdown of D-amino acids (e.g. D-alanine and D-serine – the neurotransmitters) is inhibited by risperidone.
Risperidone acts on the following receptors:
Receptors
Description
Dopamine
This drug is an antagonist of the D1 (D1, and D5) as well as the D2 family (D2, D3 and D4) receptors, with 70-fold selectivity for the D2 family. This drug has “tight binding” properties, which means it has a long half-life and like other antipsychotics, risperidone blocks the mesolimbic pathway, the prefrontal cortex limbic pathway, and the tuberoinfundibular pathway in the central nervous system. Risperidone may induce extrapyramidal side effects, akathisia and tremors, associated with diminished dopaminergic activity in the striatum. It can also cause sexual side effects, galactorrhoea, infertility, gynecomastia and, with chronic use reduced bone mineral density leading to breaks, all of which are associated with increased prolactin secretion.
Serotonin
Its action at these receptors may be responsible for its lower extrapyramidal side effect liability (via the 5-HT2A/2C receptors) and improved negative symptom control compared to typical antipsychotics such as haloperidol for instance. Its antagonistic actions at the 5-HT2C receptor may account, in part, for its weight gain liability.
Alpha α1 Adrenergic
This action accounts for its orthostatic hypotensive effects and perhaps some of the sedating effects of risperidone.
Alpha α2 Adrenergic
Perhaps greater positive, negative, affective and cognitive symptom control.
Histamine H1
Effects on these receptors account for its sedation and reduction in vigilance. This may also lead to drowsiness and weight gain.
Voltage-Gated Sodium Channels
Because it accumulates in synaptic vesicles, Risperidone inhibits voltage-gated sodium channels at clinically used concentrations. Though this medication possesses similar effects to other typical and atypical antipsychotics, it does not possess an affinity for the muscarinic acetylcholine receptors. In many respects, this medication can be useful as an “acetylcholine release-promoter” similar to gastrointestinal drugs such as metoclopramide and cisapride.
Pharmacokinetics
Risperidone undergoes hepatic metabolism and renal excretion. Lower doses are recommended for patients with severe liver and kidney disease. The active metabolite of risperidone, paliperidone, is also used as an antipsychotic.
Society and Culture
Regulatory Status
Risperidone was approved by the FDA in 1993 for the treatment of schizophrenia. In 2003, the FDA approved risperidone for the short-term treatment of the mixed and manic states associated with bipolar disorder. In 2006, the FDA approved risperidone for the treatment of irritability in autistic children and adolescents. The FDA’s decision was based in part on a study of autistic people with severe and enduring problems of violent meltdowns, aggression, and self-injury; risperidone is not recommended for autistic people with mild aggression and explosive behaviour without an enduring pattern. On 22 August 2007, risperidone was approved as the only drug agent available for treatment of schizophrenia in youths, ages 13-17; it was also approved that same day for treatment of bipolar disorder in youths and children, ages 10-17, joining lithium.
Availability
Janssen’s patent on risperidone expired on 29 December 2003, opening the market for cheaper generic versions from other companies, and Janssen’s exclusive marketing rights expired on 29 June 2004 (the result of a paediatric extension). It is available under many brand names worldwide.
Risperidone is available as a tablet, an oral solution, and an ampule, which is a depot injection.
Lawsuits
On 11 April 2012, Johnson & Johnson (J&J) and its subsidiary Janssen Pharmaceuticals Inc. were fined $1.2 billion by Judge Timothy Davis Fox of the Sixth Division of the Sixth Judicial Circuit of the US state of Arkansas. The jury found the companies had downplayed multiple risks associated with risperidone (Risperdal). The verdict was later reversed by the Arkansas State Supreme court.
In August 2012, Johnson & Johnson agreed to pay $181 million to 36 US states in order to settle claims that it had promoted risperidone and paliperidone for off-label uses including for dementia, anger management, and anxiety.
In November 2013, J&J was fined $2.2 billion for illegally marketing risperidone for use in people with dementia.
In 2015, Steven Brill posted a 15-part investigative journalism piece on J&J in The Huffington Post, called “America’s most admired lawbreaker”, which was focused on J&J’s marketing of risperidone.
J&J has faced numerous civil lawsuits on behalf of children who were prescribed risperidone who grew breasts (a condition called gynecomastia); as of July 2016 there were about 1,500 cases in Pennsylvania state court in Philadelphia, and there had been a February 2015 verdict against J&J with $2.5 million awarded to a man from Alabama, a $1.75M verdict against J&J that November, and in 2016 a $70 million verdict against J&J. In October, 2019, a jury awarded a Pennsylvania man $8 billion in a verdict against J&J.
Names
Brand names include Risperdal, Risperdal Consta, Risperdal M-Tab, Risperdal Quicklets, and Risperlet.
Bipolarised: Rethinking Mental Illness is a 2014 documentary by director Rita Kotzia.
Challenges conventional wisdom about mental illness and drug therapy through the raw personal journey of a man diagnosed as bipolar.
Outline
This documentary is about one man’s personal journey to heal. Diagnosed with bipolar disorder, Ross’ psychiatrist told him he would live with the disorder for the rest of his life and that he would have to take lithium to control symptoms. To Ross, taking the drug daily felt like a chemical lobotomy, leaving him in a foggy, drug-induced haze. Ross ultimately decided to resolve his symptoms outside of conventional medicine. He progressively reduced his use of the psychotropic drug lithium, at an experimental clinic in Costa Rica. What ensued was a self-exploration into alternative treatments to treat his condition and a journey delving into the root cause of his mental breakdown. The film uses Ross’ personal experiences to tell a larger story about medication. It will reveal how we are labelling more and more people with mental illnesses and how, in tandem, we are prescribing more and more toxic psychotropic drugs to treat these illnesses. It weaves together a series of interviews with activists, psychiatrists and other psychiatric survivors who have challenged the status quo as well as recounts some of the alternative therapies Ross uses to maintain his mental, emotional and physical health.
Lamotrigine, sold as the brand name Lamictal among others, is an anticonvulsant medication used to treat epilepsy and to delay or prevent the recurrence of depressive episodes in bipolar disorder. For epilepsy, this includes focal seizures, tonic-clonic seizures, and seizures in Lennox-Gastaut syndrome. In bipolar disorder, lamotrigine has not been shown to reliably treat acute depression; but for patients with bipolar disorder who are not currently symptomatic, it appears to be effective in reducing the risk of future episodes of depression.
Common side effects include nausea, sleepiness, headache, vomiting, trouble with coordination, and rash. Serious side effects include lack of red blood cells, increased risk of suicide, Stevens-Johnson syndrome, and allergic reactions. Concerns exist that use during pregnancy or breastfeeding may result in harm. Lamotrigine is a phenyltriazine, making it chemically different from other anticonvulsants. Its mechanism of action is not clear, but it appears to inhibit release of excitatory neurotransmitters via voltage-sensitive sodium channels in neurons.
Lamotrigine was first marketed in the United Kingdom in 1991, and approved for use in the United States in 1994. It is on the World Health Organization’s List of Essential Medicines. In 2019, it was the 71st most commonly prescribed medication in the United States, with more than 10 million prescriptions.
Brief History
1991 – Lamotrigine is first used in the United Kingdom as an anticonvulsant medication.
December 1994 – Lamotrigine was first approved for use in the United States and, that for the treatment of partial seizures.
August 1998 – For use as adjunctive treatment of Lennox-Gastaut syndrome in paediatric and adult patients, new dosage form: chewable dispersible tablets.
December 1998 – For use as monotherapy for treatment of partial seizures in adult patients when converting from a single enzyme-inducing anticonvulsant drug.
January 2003 – For use as adjunctive therapy for partial seizures in paediatric patients as young as two years of age.
June 2003 – Approved for maintenance treatment of Bipolar II disorder; the first such medication since lithium.
January 2004 – For use as monotherapy for treatment of partial seizures in adult patients when converting from the anti-epileptic drug valproate (including valproic acid).
Medical Uses
Epilepsy
Lamotrigine is considered a first-line drug for primary generalized tonic-clonic seizures (includes simple partial, complex partial, and secondarily generalized seizures such as focal-onset tonic-clonic seizures). It is also used as an alternative or adjuvant medication for partial seizures, such as absence seizure, myoclonic seizure, and atonic seizures. A 2020 review on the use of Lamotrigine as an add-on therapy for drug resistant generalized tonic-clonic seizures was unable to come to conclusions to inform clinical practice. Although low-certainty evidence suggest that it reduces generalised tonic-clonic seizures by 50% the level of uncertainty indicates that the actual findings could be significantly different. Another 2020 Cochrane review examining the use of lamotrigine as an add-on therapy for drug-resistant focal epilepsy found it to be effective for reducing seizure frequency and was well tolerated.
Lennox-Gastaut Syndrome
Lamotrigine is one of a small number of FDA-approved therapies for the form of epilepsy known as Lennox-Gastaut syndrome. It reduces the frequency of LGS seizures, and is one of two medications known to decrease the severity of drop attacks. Combination with valproate is common, but this increases the risk of lamotrigine-induced rash, and necessitates reduced dosing due to the interaction of these drugs.
Bipolar Disorder
Lamotrigine is approved in the US for maintenance treatment of bipolar I disorder and bipolar II disorder. While the anticonvulsants carbamazepine and valproate are predominantly antimanics, lamotrigine has demonstrated efficacy only in preventing or reducing the risk of recurrent depressive episodes of bipolar disorder. The drug seems ineffective in the treatment of current rapid-cycling, acute mania, or acute depression in bipolar disorder.
Lamotrigine has not demonstrated clear efficacy in treating acute mood episodes, either mania or depression. It has not demonstrated effectiveness in treating acute mania, and there is controversy regarding the drug’s effectiveness in treating acute bipolar depression. A paper written in 2008 by Nassir et al. reviewed evidence from trials that were unpublished and not referenced in the 2002 APA guidelines, and it concludes that lamotrigine has “very limited, if any, efficacy in the treatment of acute bipolar depression”. A 2008 paper by Calabrese et al. examined much of the same data, and found that in five placebo-controlled studies, lamotrigine did not significantly differ from placebo in the treatment of bipolar depression. However, in a meta-analysis of these studies conducted in 2008, Geddes, Calabrese and Goodwin found that lamotrigine was effective in individuals with bipolar depression, with a number needed to treat (NNT) of 11, or 7 in severe depression.
A 2013 review about lamotrigine concluded that it is recommended in bipolar maintenance when depression is prominent and that more research is needed in regard to its role in the treatment of acute bipolar depression and unipolar depression. No information to recommend its use in other psychiatric disorders was found.
Schizophrenia
Lamotrigine, as a monotherapy, is not substantially effective against schizophrenia. However; various publications and textbooks have expressed that lamotrigine could be added to clozapine as augmentation therapy against partial or non-responding schizophrenic patients. Patients had statistically significant improvements in positive, negative and affective symptoms. Lamotrigine does not have a statistically significant effect with antipsychotics other than clozapine, such as: olanzapine, risperidone, haloperidol, zuclopenthixol, etc.
Other Uses
Off-label uses include the treatment of peripheral neuropathy, trigeminal neuralgia, cluster headaches, migraines, visual snow, and reducing neuropathic pain, although a systematic review conducted in 2013 concluded that well-designed clinical trials have shown no benefit for lamotrigine in neuropathic pain. Off-label psychiatric usage includes the treatment of treatment-resistant obsessive-compulsive disorder, depersonalisation disorder, hallucinogen persisting perception disorder, schizoaffective disorder, and borderline personality disorder.
It has not been shown to be useful in post-traumatic stress disorder.
Side Effects
Lamotrigine prescribing information has a black box warning about life-threatening skin reactions, including Stevens-Johnson syndrome (SJS), DRESS syndrome, and toxic epidermal necrolysis (TEN). The manufacturer states that nearly all cases appear in the first two to eight weeks of therapy. Patients should seek medical attention for any unexpected skin rash, as its presence is an indication of a possible serious or even deadly side effect of the drug. Not all rashes that occur while taking lamotrigine progress to SJS or TEN. Between 5 and 10% of patients will develop a rash, but only one in a thousand patients will develop a serious rash. Rash and other skin reactions are more common in children, so this medication is often reserved for adults. For patients whose lamotrigine has been stopped after development of a rash, rechallenge with lamotrigine is also a viable option. However, it is not applicable for very serious cases. The incidence of these eruptions increases in patients who are currently on, or recently discontinued a valproate-type anticonvulsant drug, as these medications interact in such a way that the clearance of both is decreased and the effective dose of lamotrigine is increased.
Side effects such as rash, fever, and fatigue are very serious, as they may indicate incipient SJS, TEN, DRESS syndrome, or aseptic meningitis. Other side effects include loss of balance or coordination, double vision, crossed eyes, pupil constriction, blurred vision, dizziness and lack of coordination, drowsiness, insomnia, anxiety, vivid dreams or nightmares, dry mouth, mouth ulcers, memory problems, mood changes, itchiness, runny nose, cough, nausea, indigestion, abdominal pain, weight loss, missed or painful menstrual periods, and vaginitis. The side-effects profile varies for different patient populations. Overall adverse effects in treatment are similar between men, women, geriatric, paediatric and racial groups.
Lamotrigine has been associated with a decrease in white blood cell count (leukopenia). Lamotrigine does not prolong QT/QTc in TQT studies in healthy subjects.
In people taking antipsychotics, cases of lamotrigine-precipitated neuroleptic malignant syndrome have been reported.
In 2018, the FDA required a new warning for the risk of hemophagocytic lymphohistiocytosis. This reaction can occur between days to weeks after starting the treatment.
Women
Women are more likely than men to have side effects. This is the opposite of most other anticonvulsants.
Some evidence shows interactions between lamotrigine and female hormones, which can be of particular concern for women on oestrogen-containing hormonal contraceptives. Ethinylestradiol, an ingredient of such contraceptives, has been shown to decrease serum levels of lamotrigine. Women starting an oestrogen-containing oral contraceptive may need to increase the dosage of lamotrigine to maintain its level of efficacy. Likewise, women may experience an increase in lamotrigine side effects upon discontinuation of birth control pills. This may include the “pill-free” week where lamotrigine serum levels have been shown to increase twofold.
Pregnancy and Breastfeeding
Many studies have found no association between lamotrigine exposure in utero and birth defects, while those that have found an association have found only slight associations with minor malformations such as cleft palates. Review studies have found that overall rates of congenital malformations in infants exposed to lamotrigine in utero are relatively low (1-4%), which is similar to the rate of malformations in the general population. It is known that lamotrigine is a weak inhibitor of human dihydrofolate reductase (DHFR) and other, more powerful, human DHFR inhibitors such as methotrexate are known to be teratogenic.
Lamotrigine is expressed in breast milk; the manufacturer does not recommend breastfeeding during treatment. However, recent studies suggest that lamotrigine is safe to use while breastfeeding. A frequently updated review of scientific literature rates lamotrigine as L3: moderately safe.
Other Types of Effects
Lamotrigine binds to melanin-containing tissues such as the iris of the eye or melanin-rich skin. The long-term consequences of this are unknown.
GlaxoSmithKline investigated lamotrigine for the treatment of ADHD with inconclusive results. No detrimental effects on cognitive function were observed; however, the only statistical improvement in core ADHD symptoms was an improvement on a Paced Auditory Serial Addition Test (PASAT) that measures auditory processing speed and calculation ability. Another study reported that lamotrigine might be a safe and effective treatment option for adult ADHD comorbid with bipolar and recurrent depression.
Lamotrigine is known to affect sleep. Studies with small numbers of patients (10-15) reported that lamotrigine increases the duration of REM sleep, decreases the number of phase shifts, and decreases the duration of slow-wave sleep, and that there was no effect on vigilance, daytime somnolence and cognitive function. However, a retrospective study of 109 patients’ medical records found that 6.7% of patients experienced an “alerting effect” resulting in intolerable insomnia, for which the treatment had to be discontinued.
Lamotrigine can induce a type of seizure known as a myoclonic jerk, which tends to happen soon after the use of the medication. When used in the treatment of myoclonic epilepsies such as juvenile myoclonic epilepsy, lower doses (and lower plasma levels) are usually needed, as even moderate doses of this drug can induce seizures, including tonic-clonic seizures, which can develop into status epilepticus, which is a medical emergency. It can also cause myoclonic status epilepticus.
In overdose, lamotrigine can cause uncontrolled seizures in most people. Reported results in overdoses involving up to 15 g include increased seizures, coma, and death.
Pharmacology
Mechanism of Action
Lamotrigine is a member of the sodium channel blocking class of antiepileptic drugs. This may suppress the release of glutamate and aspartate, two dominant excitatory neurotransmitters in the central nervous system. It is generally accepted to be a member of the sodium channel blocking class of antiepileptic drugs, but it could have additional actions, since it has a broader spectrum of action than other sodium channel antiepileptic drugs such as phenytoin and is effective in the treatment of the depressed phase of bipolar disorder, whereas other sodium channel-blocking antiepileptic drugs are not, possibly on account of its sigma receptor activity. In addition, lamotrigine shares few side effects with other, unrelated anticonvulsants known to inhibit sodium channels, which further emphasizes its unique properties.
It is a triazine derivate that inhibits voltage-sensitive sodium channels, leading to stabilisation of neuronal membranes. It also blocks L-, N-, and P-type calcium channels and weakly inhibits the serotonin 5-HT3 receptor. These actions are thought to inhibit release of glutamate at cortical projections in the ventral striatum limbic areas, and its neuroprotective and anti-glutamatergic effects have been pointed out as promising contributors to its mood stabilising activity. Observations that lamotrigine reduced γ-aminobutyric acid (GABA) A receptor-mediated neurotransmission in rat amygdala, suggest that a GABAergic mechanism may also be involved. It appears that lamotrigine does not increase GABA blood levels in humans.
Lamotrigine does not have pronounced effects on any of the usual neurotransmitter receptors that anticonvulsants affect (adrenergic, dopamine D1 and D2, muscarinic, GABA, histaminergic H1, serotonin 5-HT2, and N-methyl-D-aspartate). Inhibitory effects on 5-HT, norepinephrine, and dopamine transporters are weak. Lamotrigine is a weak inhibitor of dihydrofolate reductase, but whether this effect is sufficient to contribute to a mechanism of action or increases risk to the foetus during pregnancy is not known. Early studies of lamotrigine’s mechanism of action examined its effects on the release of endogenous amino acids from rat cerebral cortex slices in vitro. As is the case for antiepileptic drugs that act on voltage-dependent sodium channels, lamotrigine thereby inhibits the release of glutamate and aspartate, which is evoked by the sodium-channel activator veratrine, and was less effective in the inhibition of acetylcholine or GABA release. At high concentrations, it had no effect on spontaneous or potassium-evoked amino acid release.
These studies suggested that lamotrigine acts presynaptically on voltage-gated sodium channels to decrease glutamate release. Several electrophysiological studies have investigated the effects of lamotrigine on voltage-gated sodium channels. For example, lamotrigine blocked sustained repetitive firing in cultured mouse spinal cord neurons in a concentration-dependent manner, at concentrations that are therapeutically relevant in the treatment of human seizures. In cultured hippocampal neurons, lamotrigine reduced sodium currents in a voltage-dependent manner, and at depolarised potentials showed a small frequency-dependent inhibition. These and a variety of other results indicate that the antiepileptic effect of lamotrigine, like those of phenytoin and carbamazepine, is at least in part due to use- and voltage-dependent modulation of fast voltage-dependent sodium currents. However, lamotrigine has a broader clinical spectrum of activity than phenytoin and carbamazepine and is recognised to be protective against generalised absence epilepsy and other generalised epilepsy syndromes, including primary generalised tonic-clonic seizures, juvenile myoclonic epilepsy, and Lennox-Gastaut syndrome.
The basis for this broader spectrum of activity of lamotrigine is unknown, but could relate to actions of the drug on voltage-gated calcium channels. Lamotrigine blocks T-type calcium channels weakly, if at all. However, it does inhibit native and recombinant high voltage–gated calcium channels (N- and P/Q/R-types) at therapeutic concentrations. Whether this activity on calcium channels accounts for lamotrigine’s broader clinical spectrum of activity in comparison with phenytoin and carbamazepine remains to be determined.
It antagonises these receptors with the following IC50 values:
5-HT3, IC50 = 18 μM
σ receptors, IC50 = 145 μM
Pharmacokinetics
The pharmacokinetics of lamotrigine follow first-order kinetics, with a half-life of 29 hours and volume of distribution of 1.36 L/kg. Lamotrigine is rapidly and completely absorbed after oral administration. Its absolute bioavailability is 98% and its plasma Cmax occurs from 1.4 to 4.8 hours. Available data indicate that its bioavailability is not affected by food. Estimate of the mean apparent volume of distribution of lamotrigine following oral administration ranges from 0.9 to 1.3 L/kg. This is independent of dose and is similar following single and multiple doses in both patients with epilepsy and in healthy volunteers.
Lamotrigine is inactivated by glucuronidation in the liver. Lamotrigine is metabolised predominantly by glucuronic acid conjugation. Its major metabolite is an inactive 2-n-glucuronide conjugate.
Lamotrigine has fewer drug interactions than many anticonvulsant drugs, although pharmacokinetic interactions with carbamazepine, phenytoin and other hepatic enzyme inducing medications may shorten half-life. Dose adjustments should be made on clinical response, but monitoring may be of benefit in assessing compliance.
The capacity of available tests to detect potentially adverse consequences of melanin binding is unknown. Clinical trials excluded subtle effects and optimal duration of treatment. There are no specific recommendations for periodic ophthalmological monitoring. Lamotrigine binds to the eye and melanin-containing tissues which can accumulate over time and may cause toxicity. Prescribers should be aware of the possibility of long-term ophthalmologic effects and base treatment on clinical response. Patient compliance should be periodically reassessed with lab and medical testing of liver and kidney function to monitor progress or side effects.
Society and Culture
Brand Names
Lamotrigine was originally brought to market by GlaxoSmithKline, trademarked as Lamictal; it is also available in generic form under many brand names worldwide.


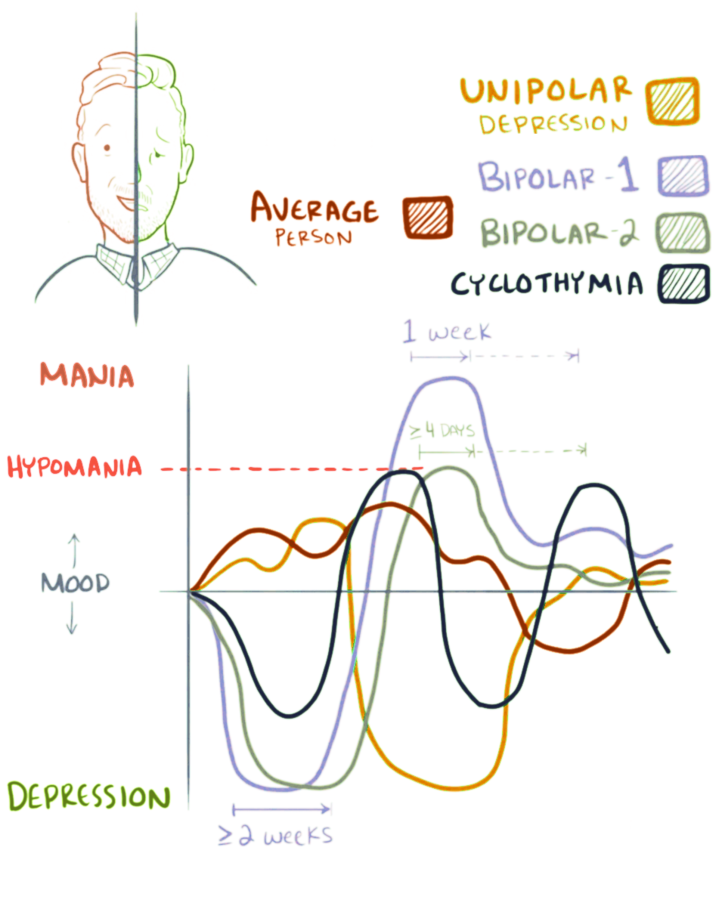
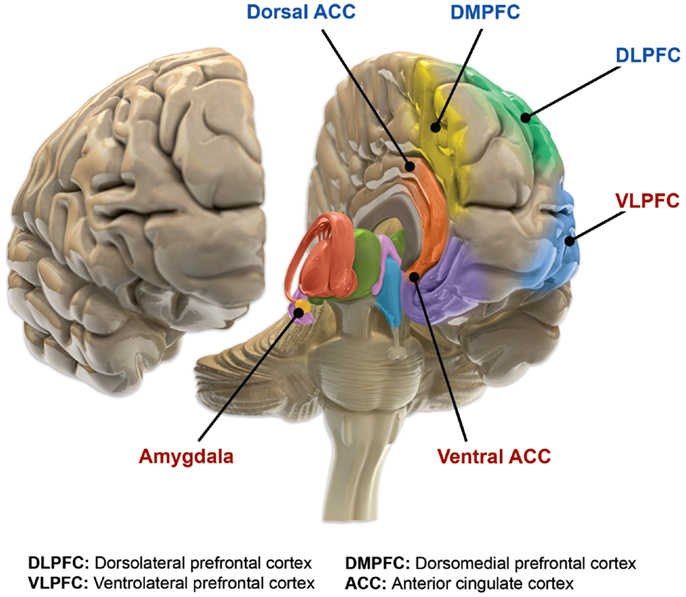





You must be logged in to post a comment.