Anosognosia is a condition in which a person with a disability is cognitively unaware of having it due to an underlying physical or psychological (e.g. PTSD, Stockholm syndrome, schizophrenia, bipolar disorder, dementia) condition.
Anosognosia can result from physiological damage to brain structures, typically to the parietal lobe or a diffuse lesion on the fronto-temporal-parietal area in the right hemisphere, and is thus a neuropsychiatric disorder. A deficit of self-awareness, it was first named by the neurologist Joseph Babinski in 1914. Phenomenologically, anosognosia has similarities to denial, which is a psychological defence mechanism; attempts have been made at a unified explanation. Anosognosia is sometimes accompanied by asomatognosia, a form of neglect in which patients deny ownership of body parts such as their limbs. The term is from Ancient Greek ἀ- a-, ‘without’, νόσος nosos, ‘disease’ and γνῶσις gnōsis, ‘knowledge’. It is also considered a disorder that makes the treatment of the patient more difficult, since it may affect negatively the therapeutic relationship.
Causes
Relatively little has been discovered about the cause of the condition since its initial identification. Recent empirical studies tend to consider anosognosia a multi-componential syndrome or multi-faceted phenomenon. That is it can be manifested by failure to be aware of a number of specific deficits, including motor (hemiplegia), sensory (hemianaesthesia, hemianopia), spatial (unilateral neglect), memory (dementia), and language (receptive aphasia) due to impairment of anatomo-functionally discrete monitoring systems.
Anosognosia is relatively common following different causes of brain injury, such as stroke and traumatic brain injury; for example, anosognosia for hemiparesis (weakness of one side of the body) with onset of acute stroke is estimated at between 10% and 18%. However, it can appear to occur in conjunction with virtually any neurological impairment. It is more frequent in the acute than in the chronic phase and more prominent for assessment in the cases with right hemispheric lesions than with the left. Anosognosia is not related to global mental confusion, cognitive flexibility, other major intellectual disturbances, or mere sensory/perceptual deficits.
The condition does not seem to be directly related to sensory loss but is thought to be caused by damage to higher level neurocognitive processes that are involved in integrating sensory information with processes that support spatial or bodily representations (including the somatosensory system). Anosognosia is thought to be related to unilateral neglect, a condition often found after damage to the non-dominant (usually the right) hemisphere of the cerebral cortex in which people seem unable to attend to, or sometimes comprehend, anything on a certain side of their body (usually the left).
Anosognosia can be selective in that an affected person with multiple impairments may seem unaware of only one handicap, while appearing to be fully aware of any others. This is consistent with the idea that the source of the problem relates to spatial representation of the body. For example, anosognosia for hemiplegia may occur with or without intact awareness of visuo-spatial unilateral neglect. This phenomenon of double dissociation can be an indicator of domain-specific disorders of awareness modules, meaning that in anosognosia, brain damage can selectively impact the self-monitoring process of one specific physical or cognitive function rather than a spatial location of the body.
There are also studies showing that the manoeuvre of vestibular stimulation could temporarily improve both the syndrome of spatial unilateral neglect and of anosognosia for left hemiplegia. Combining the findings of hemispheric asymmetry to the right, association with spatial unilateral neglect, and the temporal improvement on both syndromes, it is suggested there can be a spatial component underlying the mechanism of anosognosia for motor weakness and that neural processes could be modulated similarly. There were some cases of anosognosia for right hemiplegia after left hemisphere damage, but the frequency of this type of anosognosia has not been estimated.
Anosognosia may occur as part of receptive aphasia, a language disorder that causes poor comprehension of speech and the production of fluent but incomprehensible sentences. A patient with receptive aphasia cannot correct his own phonetics errors and shows “anger and disappointment with the person with whom s/he is speaking because that person fails to understand her/him”. This may be a result of brain damage to the posterior portion of the superior temporal gyrus, believed to contain representations of word sounds. With those representations significantly distorted, patients with receptive aphasia are unable to monitor their mistakes. Other patients with receptive aphasia are fully aware of their condition and speech inhibitions, but cannot monitor their condition, which is not the same as anosognosia and therefore cannot explain the occurrence of neologistic jargon.
Psychiatry
Although largely used to describe unawareness of impairment after brain injury or stroke, the term “anosognosia” is occasionally used to describe the lack of insight shown by some people with anorexia nervosa. They do not seem to recognise that they have a mental illness. There is evidence that anosognosia related to schizophrenia may be the result of frontal lobe damage. E. Fuller Torrey, a psychiatrist and schizophrenia researcher, has stated that among those with schizophrenia and bipolar disorder, anosognosia is the most prevalent reason for not taking medications.
Diagnosis
Clinically, anosognosia is often assessed by giving patients an anosognosia questionnaire in order to assess their metacognitive knowledge of deficits. However, neither of the existing questionnaires applied in the clinics are designed thoroughly for evaluating the multidimensional nature of this clinical phenomenon; nor are the responses obtained via offline questionnaire capable of revealing the discrepancy of awareness observed from their online task performance. The discrepancy is noticed when patients showed no awareness of their deficits from the offline responses to the questionnaire but demonstrated reluctance or verbal circumlocution when asked to perform an online task. For example, patients with anosognosia for hemiplegia may find excuses not to perform a bimanual task even though they do not admit it is because of their paralysed arms.
A similar situation can happen to patients with anosognosia for cognitive deficits after traumatic brain injury when monitoring their errors during the tasks regarding their memory and attention (online emergent awareness) and when predicting their performance right before the same tasks (online anticipatory awareness). It can also occur among patients with dementia and anosognosia for memory deficit when prompted with dementia-related words, showing possible pre-attentive processing and implicit knowledge of their memory problems. Patients with anosognosia may also overestimate their performance when asked in first-person formed questions but not from a third-person perspective when the questions referring to others.
When assessing the causes of anosognosia within stroke patients, CT scans have been used to assess where the greatest amount of damage is found within the various areas of the brain. Stroke patients with mild and severe levels of anosognosia (determined by response to an anosognosia questionnaire) have been linked to lesions within the temporoparietal and thalamic regions, when compared to those who experience moderate anosognosia, or none at all. In contrast, after a stroke, people with moderate anosognosia have a higher frequency of lesions involving the basal ganglia, compared to those with mild or severe anosognosia.
Treatment
In regard to anosognosia for neurological patients, no long-term treatments exist. As with unilateral neglect, caloric reflex testing (squirting ice cold water into the left ear) is known to temporarily ameliorate unawareness of impairment. It is not entirely clear how this works, although it is thought that the unconscious shift of attention or focus caused by the intense stimulation of the vestibular system temporarily influences awareness. Most cases of anosognosia appear to simply disappear over time, while other cases can last indefinitely. Normally, long-term cases are treated with cognitive therapy to train patients to adjust for their inoperable limbs (though it is believed that these patients still are not “aware” of their disability). Another commonly used method is the use of feedback – comparing clients’ self-predicted performance with their actual performance on a task in an attempt to improve insight.
Neurorehabilitation is difficult because, as anosognosia impairs the patient’s desire to seek medical aid, it may also impair their ability to seek rehabilitation. A lack of awareness of the deficit makes cooperative, mindful work with a therapist difficult. In the acute phase, very little can be done to improve their awareness, but during this time, it is important for the therapist to build a therapeutic alliance with patients by entering their phenomenological field and reducing their frustration and confusion. Since severity changes over time, no single method of treatment or rehabilitation has emerged or will likely emerge.
In regard to psychiatric patients, empirical studies verify that, for individuals with severe mental illnesses, lack of awareness of illness is significantly associated with both medication non-compliance and re-hospitalisation. Fifteen percent of individuals with severe mental illnesses who refuse to take medication voluntarily under any circumstances may require some form of coercion to remain compliant because of anosognosia. Coercive psychiatric treatment is a delicate and complex legal and ethical issue.
One study of voluntary and involuntary inpatients confirmed that committed patients require coercive treatment because they fail to recognise their need for care. The patients committed to the hospital had significantly lower measures of insight than the voluntary patients.
Anosognosia is also closely related to other cognitive dysfunctions that may impair the capacity of an individual to continuously participate in treatment. Other research has suggested that attitudes toward treatment can improve after involuntary treatment and that previously committed patients tend later to seek voluntary treatment.
This page is based on the copyrighted Wikipedia article <https://en.wikipedia.org/wiki/Anosognosia >; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
Schizophrenics Anonymous is a peer support group to help people who are affected by schizophrenia and related disorders including bipolar disorder, schizoaffective disorder, psychotic depression and psychosis.
Brief History
The programme was established in Detroit in 1985. The founder was Joanne Verbanic, who was diagnosed with schizophrenia in 1970. Shortly before forming SA, Verbanic publicly disclosed her diagnosis and discussed her illness on national television in an effort to challenge the stigma associated with the condition. She was a 2006 recipient of a Lilly Reintegration Award in recognition of her lifetime contributions to the mental health community, and she continued to be active as a spokesperson for persons with schizophrenia and other mental illness until her death on 07 May 2015.
By 2007, more than 150 local SA groups operated in 31 of the 50 United States, and in Australia, Brazil, Canada, Mexico, France, India and Venezuela.
Technical support for Schizophrenics Anonymous was provided by the National Schizophrenia Foundation (NSF) until 2007 when NSF ceased operations. In response to the loss of a national sponsor, a group of consumers, family members, and mental health providers came together to form a not-for-profit organisation, Schizophrenia and Related Disorders Alliance of America (SARDAA).
SARDAA promotes recovery for persons with schizophrenia and related brain disorders including bipolar disorder, schizoaffective disorder, depression with psychosis, and experience with psychosis. They envision a future in which every person with a schizophrenia-related brain disorder has the opportunity to recover from their disorders. The name Schizophrenics Anonymous was changed to Schizophrenia Alliance in 2015 and added Psychosis Support and Acceptance in 2018. They provide an online directory of SA groups, sponsor five weekly SA conference calls, and one Family and Friends conference call. At their annual conference, the group trains individuals and groups who have started or would like to start an SA group.
Although some SA groups are organised by mental health professionals, research has suggested that peer-led SA groups are more sustainable and longer lasting. Some groups are organised in psychiatric hospitals or jails and are not open to the public.
Programme Principles
The SA programme is based on the twelve-step model, but includes just six steps. The organisation describes the programme’s purpose of helping participants to learn about schizophrenia, “restore dignity and sense of purpose,” obtain “fellowship, positive support, and companionship,” improve their attitudes about their lives and their illnesses, and take “positive steps towards recovery.”
Joanne Verbanic wrote the original “Schizophrenics Anonymous” book, better known as “The Blue Book,” which describes the six steps to recovery. The steps require members to admit they need help, take responsibility for their choices and consequences, believe they have the inner strength to help themselves and others, forgive themselves and others, understand that false beliefs contribute to their problems and change those beliefs, and decide to turn their lives over to a higher power.
Research
One study about the risks of professional partnerships centres on the partnership between Schizophrenics Anonymous (SA) and the Mental Health Association of Michigan (MHAM) over a 14-year period. The study shows that the professional partnership resulted in increased access to SA Groups across Michigan and organisation expansion and development within SA. The professional influence also lead more SA Groups to be held in more traditional mental health treatment settings and led to more professional-led SA groups.
Self-help groups are more available to people who live independently. Researchers at Michigan State University studied whether SA would be successful in group homes. The results were positive: the groups had high attendance and participation and were well liked. However, staff members controlled who could lead and who could attend the meetings, and how the meetings should be run. The programs fell apart. The same obstacle occurred in SA groups started in prisons and monitored by employees.
This page is based on the copyrighted Wikipedia article <https://en.wikipedia.org/wiki/Schizophrenics_Anonymous>; it is used under the Creative Commons Attribution-ShareAlike 3.0 Unported License (CC-BY-SA). You may redistribute it, verbatim or modified, providing that you comply with the terms of the CC-BY-SA.
The Depression and Bipolar Support Alliance (DBSA), formerly the National Depressive and Manic Depressive Association (NDMDA), is a non-profit organisation providing support groups for people who live with depression or bipolar disorder as well as their friends and family.
DBSA’s scope, also includes outreach, education and advocacy regarding depression and bipolar disorder. DBSA employs a small staff and operates with the guidance of a Scientific Advisory Board.
DBSA sponsors online and “face to face” support groups. A nonrandomized study found participants in such groups reported their coping skills, medication compliance, and acceptance of their illness correlated with participation. Member hospitalization decreased by 49% (from 82% to 33%). Following an initial meeting, members were found to be 6.8 times more likely to attend subsequent meetings if accompanied by a member the first time.
DBSA is a not-for-profit 501(c)(3) organisation and receives over 21 million hits per year on their combined websites. Each month, DBSA distributes nearly 20,000 educational materials free of charge to anyone requesting information about mood disorders. DBSA reaches nearly five million people through their educational materials and programs, exhibit materials, and media activities.
The Depression and Bipolar Support Alliance (DBSA) Greater Houston is a 501(c)(3) non-profit organisation located in Houston, Texas.
DBSA provides free and confidential support groups for individuals living with, or family and friends affected by, depression or bipolar disorder. Each support group is led by a facilitator trained by the organisation. Select groups target specific populations including veterans, adolescents, and parents of adolescents, young adults, senior citizens, LGBT Community, homeless individuals and Spanish-speaking individuals.
Established in 1979, the Depressive and Manic Disorder Association (DMDA) of Greater Houston sponsored up to five weekly support groups for those with depressive or manic depressive disorders. In 2003, DMDA Greater Houston changed its name to DBSA Greater Houston and formed its own 501(c) (3) corporation. Currently, DBSA Greater Houston sponsors nearly 70 weekly support groups at 50 different locations throughout the Houston metropolitan area. The Houston organisation is the largest of the nation’s DBSA chapters, serving over 1,000 support group participants annually.
Affiliation
The Depression and Bipolar Support Alliance of Greater Houston is a chapter member of the National Depression and Bipolar Support Alliance organisation based in Chicago, Illinois. Additionally, the organisation has developed collaborations with a number of Houston area mental health and social service providers including the Texas Department of Corrections, the Harris County judicial system, the Michael DeBakey VA Hospital, Mental Health of America, National Alliance on Mental Illness and the AIDS Foundation of Houston. Every group provided by DBSA Greater Houston is a collaboration with another organisation in the community. For a list of collaborations, visit the organisations website.
Statistics
DBSA Greater Houston utilises 75 trained volunteer and professional facilitators to provide nearly 70 weekly support groups. According to an independently conducted demographics study in 2008, 64% of DBSA Greater Houston participants were female, 36% were male; 77% were diagnosed individuals while 23% were family members; 66% reported a diagnosis and/or symptoms of depression, 69% were diagnosed with bipolar disorder; 88% were prescribed psychotropic medications and 65% were in professional therapy.
The Depression and Bipolar Support Alliance of Greater Houston conducts an annual satisfaction survey for participants. In 2013, the results continued to show a high rating of satisfaction with a score of 4.28 out of a possible 5, which represents excellence. Also, it was found that the longer a person attends group, the more satisfied they are with the experience and the more skills they learn to manage their disorder.
In 2006 DBSA Greater received the Chapter of the Year award from the national Depression and Bipolar Support Alliance.
Recent Developments
On 24 September 2013, the Depression and Bipolar Support Alliance of Greater Houston hosted its second annual Help, Hope, and Healing Luncheon with speakers Jessie Close and actress, Glenn Close. Jessie lives with Bipolar Disorder and Glenn talked about the perspective of the family and gave 2 monologues.
The Depression and Bipolar Support Alliance of Greater Houston hosted its first annual Help, Hope, and Healing luncheon at the River Oaks Country Club on 24 September 2012 featuring Jane Pauley as the speaker. Jane Pauley is known for her work on Dateline NBC and the Today Show. Ms. Pauley lives with Bipolar Disorder.
In the fall of 2008, DBSA Greater Houston published an outcome study independently conducted by Dr. Ralph Culler, former Associate Dean of Research at the Hogg Foundation for Mental Health. The outcome study was designed to analyse the effectiveness of the DBSA Greater Houston support group model. The study provided tools for DBSA Greater Houston to:
Provide quantitative and qualitative evidence that its support group model is effective;
Prove DBSA Greater Houston’s accountability to individuals utilising its services; and
Learn how the benefits of DBSA occur.
This study provided evidenced-based results that the DBSA Greater Houston support group model was effective in a number of areas. The study used an outcome questionnaire which asked a broad range of questions regarding demographics, medical data, outcome assessments and satisfaction with the support group experience. On average 89% of group participants experienced an improvement in their quality of life as a direct benefit of their participation in the DBSA groups. 93% of participants reported high or very high satisfaction with their DBSA support group experience.
Grandiose delusions (GD) – also known as delusions of grandeur or expansive delusions – are a subtype of delusion that occur in patients suffering from a wide range of psychiatric diseases, including two-thirds of patients in manic state of bipolar disorder, half of those with schizophrenia, patients with the grandiose subtype of delusional disorder, and a substantial portion of those with substance abuse disorders.
GDs are characterised by fantastical beliefs that one is famous, omnipotent, wealthy, or otherwise very powerful. The delusions are generally fantastic and typically have a religious, science fictional, or supernatural theme. There is a relative lack of research into GD, in contrast to persecutory delusions and auditory hallucinations. About 10% of healthy people experience grandiose thoughts but do not meet full criteria for a diagnosis of GD.
Signs and Symptoms
According to the DSM-IV-TR diagnostic criteria for delusional disorders, grandiose-type symptoms include exaggerated beliefs of:
Self-worth.
Power.
Knowledge.
Identity.
Exceptional relationship to a deity or famous person.
For example, a patient who has fictitious beliefs about his or her power or authority may believe himself or herself to be a ruling monarch who deserves to be treated like royalty. There are substantial differences in the degree of grandiosity linked with grandiose delusions in different patients. Some patients believe they are God, the Queen of the United Kingdom, a president’s son, a famous rock star, and some other examples. Others are not as expansive and think they are skilled athletes or great inventors.
Expansive delusions may be maintained by auditory hallucinations, which advise the patient that they are significant, or confabulations, when, for example, the patient gives a thorough description of their coronation or marriage to the king. Grandiose and expansive delusions may also be part of fantastic hallucinosis in which all forms of hallucinations occur.
Positive Functions
Grandiose delusions frequently serve a very positive function by sustaining or increasing their self-esteem. As a result, it is essential to consider the consequences of removing the grandiose delusion on self-esteem when trying to modify the grandiose delusion in therapy. In many instances of grandiosity, it is suitable to go for a fractional rather than a total modification, which permits those elements of the delusion that are central for self-esteem to be preserved. For example, a person who believes they are a senior secret service agent gains a great sense of self-esteem and purpose from this belief, thus until this sense of self-esteem can be provided from elsewhere, it is best not to attempt modification.
Comorbidity
Schizophrenia
Schizophrenia is a mental disorder distinguished by a loss of contact with reality and the occurrence of psychotic behaviours, including hallucinations and delusions (unreal beliefs which endure even when there is contrary evidence). Delusions may include the false and constant idea that the person is being followed or poisoned, or that the person’s thoughts are being broadcast for others to listen to. Delusions in schizophrenia often develop as a response to the individual attempting to explain their hallucinations. Patients who experience recurrent auditory hallucinations can develop the delusion that other people are scheming against them and are dishonest when they say they do not hear the voices that the delusional person believes that he or she hears.
Specifically, grandiose delusions are frequently found in paranoid schizophrenia, in which a person has an extremely exaggerated sense of his or her significance, personality, knowledge, or authority. For example, the person may declare to own a major corporation and kindly offer to write a hospital staff member a check for $5 million if only help them escape from the hospital. Other common grandiose delusions in schizophrenia include religious delusions such as the belief that one is Jesus Christ.
Bipolar I disorder can lead to severe affective dysregulation, or mood states that sway from exceedingly low (depression) to exceptionally high (mania). In hypomania or mania, some bipolar patients can suffer grandiose delusions. In its most severe manifestation, days without sleep, auditory and other hallucinations, or uncontrollable racing thoughts can reinforce these delusions. In mania, this illness affects emotions and can also lead to impulsivity and disorganised thinking, which can be harnessed to increase their sense of grandiosity. Protecting this delusion can also lead to extreme irritability, paranoia, and fear. Sometimes their anxiety can be so over-blown that they believe others are jealous of them and, thus, undermine their “extraordinary abilities,” persecuting them or even scheming to seize what they already have.
The vast majority of bipolar patients rarely experience delusions. Typically, when experiencing or displaying a stage of heightened excitability called mania, they can experience joy, rage, and other intense emotions that can cycle out of control, along with thoughts or beliefs that are grandiose. Some of these grandiose thoughts can be expressed as strong beliefs that the patient is very rich or famous or has super-human abilities, or can even lead to severe suicidal ideations. In the most severe form, in what was formerly labelled as megalomania, the bipolar patient may hear voices that support these grandiose beliefs. In their delusions, they can believe that they are, for example, a king, a creative genius, or can even exterminate the world’s poverty because of their extreme generosity.
Cause(s)
There are two alternative causes for developing grandiose delusions:
Delusion-as-defence: Defence of the mind against lower self-esteem and depression.
Emotion-consistent: Result of exaggerated emotions.
Anatomical Aspects
Grandiose delusions may be related to lesions of the frontal lobe. Temporal lobe lesions have been mainly reported in patients with delusions of persecution and of guilt, while frontal and frontotemporal involvement have been described in patients with grandiose delusions, Cotard’s syndrome, and delusional misidentification syndrome.
Diagnosis
Patients with a wide range of mental disorders which disturb brain function experience different kinds of delusions, including grandiose delusions. Grandiose delusions usually occur in patients with syndromes associated with secondary mania, such as Huntington’s disease, Parkinson’s disease, and Wilson’s disease. Secondary mania has also been caused by substances such as L-DOPA and isoniazid which modify the monoaminergic neurotransmitter function. Vitamin B12 deficiency, uraemia, hyperthyroidism as well as the carcinoid syndrome have been found to cause secondary mania, and thus grandiose delusions.
In diagnosing delusions, the MacArthur-Maudsley Assessment of Delusions Schedule is used to assess the patient
Treatment
In patients suffering from schizophrenia, grandiose and religious delusions are found to be the least susceptible to cognitive behavioural interventions. Cognitive behavioural intervention is a form of psychological therapy, initially used for depression, but currently used for a variety of different mental disorders, in hope of providing relief from distress and disability. During therapy, grandiose delusions were linked to patients’ underlying beliefs by using inference chaining. Some examples of interventions performed to improve the patient’s state were focus on specific themes, clarification of patient’s neologisms, and thought linkage. During thought linkage, the patient is asked repeatedly by the therapist to explain their jumps in thought from one subject to a completely different one.
Patients suffering from mental disorders that experience grandiose delusions have been found to have a lower risk of having suicidal thoughts and attempts.
Epidemiology
In researching over 1000 individuals of a vast range of backgrounds, Stompe and colleagues (2006) found that grandiosity remains as the second most common delusion after persecutory delusions. A variation in the occurrence of grandiosity delusions in schizophrenic patients across cultures has also been observed. In research done by Appelbaum et al. it has been found that GDs appeared more commonly in patients with bipolar disorder (59%) than in patients with schizophrenia (49%), followed by presence in substance misuse disorder patients (30%) and depressed patients (21%).
A relationship has been claimed between the age of onset of bipolar disorder and the occurrence of GDs. According to Carlson et al. (2000), grandiose delusions appeared in 74% of the patients who were 21 or younger at the time of the onset, while they occurred only in 40% of individuals 30 years or older at the time of the onset.
Prevalence
Research suggests that the severity of the delusions of grandeur is directly related to a higher self-esteem in individuals and inversely related to any individual’s severity of depression and negative self-evaluations. Lucas et al. (1962) found that there is no significant gender difference in the establishment of grandiose delusion. However, there is a claim that ‘the particular content of Grandiose delusions’ may be variable across both genders. Also, it has been noted that the presence of GDs in people with at least grammar or high school education was greater than lesser educated persons. Similarly, the presence of grandiose delusions in individuals who are the eldest is greater than in individuals who are the youngest of their siblings.
The Icarus Project was a media and activist endeavour broadly aligned to the anti-psychiatry movement and recovery approach, arguing that mental illness should be understood as an issue of social justice and that a person’s mental state can improve through greater social support and collective liberation.
It shares similarities with the academic fields of Psychopolitics and Mad Studies. The name is derived from Icarus, a hero in Greek mythology, and is metaphorically used to convey that the experiences of mental distress and other extreme mental states can lead to “potential[ly] flying dangerously close to the sun.”
Brief History
In 2002, musician Sascha Altman DuBrul wrote “Bipolar World”, an article published in the San Francisco Bay Guardian. The article described his experiences being diagnosed with bipolar disorder. Among the dozens of e-mails and other correspondence that he received after this publication was a letter from Ashley McNamara, now known as Jacks, an artist and writer who identified strongly with DuBrul’s experiences. DuBrul and McNamara corresponded for a few weeks before finally meeting in person and deciding to start The Icarus Project. Years later, musician-activist Bonfire Madigan Shive and counsellor/activist Will Hall became a key leader in The Icarus Project’s administration and development.
In the Journal of Medical Humanities, co-founder DuBrul wrote of The Icarus Project:
Though we did not fully understand it in the early days, we were walking in the footsteps of a large body of knowledge and thought from the 1960s, grouped under the category of Anti-Psychiatry.
He also noted the group and its members were inspired by a range of social trends and schools of thought including anarchism, permaculture/sustainable ecology, LGBTQ rights, harm reduction, global justice movement, the Beat Generation, counterculture, and punk rock. He writes, “Our response to the label ‘bipolar’ was not a ‘normal’ response, which is why the Icarus Project brought a new perspective to psychic diversity. To create this perspective, we drew inspiration from many social movements and subcultural communities that came before us. So even though our response was unusual, it did not arise in a vacuum. In creating the Icarus Project, we wove together the ideas and practices in these movements to imagine a powerful new counter narrative to the dominant mental health narrative that went beyond a questioning of the language around ‘bipolar’ and critiqued the system itself.”
The first step, they decided, was creating a website where people who identified with “bipolar and other ‘mental illness’ [could] find real community and contribute to it.” DuBrul states that by 2003, “The Icarus Project website was up and running, and a virtual community began to evolve around the discussion forums.” He notes that user-generated content online enabled The Icarus Project’s growth: “We were attracting interesting people, creating discussion forums with names like ‘Alternate Dimensions or Psychotic Delusions’ and ‘Experiencing Madness and Extreme States.’ There was no place else where people who used psych meds and people who did not, people who identified with diagnostic categories and people who did not, could all talk with each other and share stories. Because of the outreach in the anarchist and activist community, there was a high percentage of creative people with a radical political analysis. And with the (seeming) anonymity of the Internet, people felt comfortable being honest and sharing intimate stories about their lives. Our website served as a refuge for a diverse group of people who were learning the ways in which new narratives could be woven about their lives.”
Mission
The Icarus Project’s stated aims are to provide a “support network and education project by and for people who experience the world in ways that are often diagnosed as mental illness.” The national Icarus Collective staff is set up to support local groups instead of creating the smaller organisations themselves. The responsibilities of the local group are to gather people locally for support, education, activism, and access to alternatives to mainstream medical diagnosis and treatment. The Project advocates self-determination and caution when approaching psychiatric care. It encourages harm reduction, alternatives to the prevailing medical model that is accepted by the vast majority of mental health professionals, and self-determination in treatment and diagnosis. Key members of The Icarus Project state that they “envision a world with more options to navigate mental health issues: options that support self-determination, centre people who are most impacted by mental health-based oppression, and most critically, uplift social transformation as central to individual wellbeing.”
In 2005, Journalist Jennifer Itzenson noted that the Icarus Project accepts those with a wide range of perspectives on mental health issues, but also describes “an edge of militancy within the group,” particularly among those who reject medication. Itzenson also writes that while medical professionals applaud groups like the Icarus Project for providing a sense of support and community, and combating social stigmas related to bipolar and other mental health issues, the group’s questioning of the medical paradigm is “misguided” and that rejecting medication is a “potentially fatal choice” for those with bipolar disorder. A Newsweek article provides the following perspective on The Icarus Project’s stance towards medication: “While some critics might view Icaristas as irresponsible, their skepticism about drugs isn’t entirely unfounded. Lately, a number of antipsychotic drugs have been found to cause some troubling side effects.”
Writer Mark Lukach describes in an article for Pacific Standard his experience asking co-founder Sascha Altman DuBrul about the role of psychiatric medication as a part of his wife’s recovery from a bipolar diagnosis. Lukach articulates The Icarus Project’s approach to self-determination in psychiatric treatment. Lukach wrote:
“As for medication, DuBrul said that he believed that the answer to the question of whether or not to use pharmaceuticals needed to be far more nuanced than yes or no. The best response might be maybe, sometimes, or only certain medications. For instance, DuBrul shared that he takes lithium every night because he’s confident that, after four hospitalizations and over a decade with the label bipolar, the medication is a positive part of his care. Not the whole solution, but a piece.”
Anthropologist Erica Hua Fletcher describes Icarus Project member’s diverse ways of discussing altered mental states in the Journal of Medical Humanities. Fletcher writes:
While many Icarus contributors have found relief through the use of psycho-pharmaceutical interventions and other bio-psychiatric technologies, they also have experienced the limitations of medical paradigms and language to recognize the fullness of their lives. Because of this, they frequently adopt alternative words and phrases beyond bio-psychiatric terms to describe their mental states such as “neurodivergent processing,” “diasporas of distressing symptoms,” “sensory/cognitive/emotional trauma,” or “cognitive-emotional terror.” “Bipolar disorder” is interchangeable with highs and lows; “psychosis” can be seen as a reckoning; and nonconsensus realities can describe extreme experiences, which psychiatrists could label as symptoms of “schizophrenia” (such as hearing voices others do not hear or seeing objects others do not see). Such alternative words and phrases do not diminish the utility of bio- psychiatric terminology nor do they directly undermine medical treatment options, yet they allow for a range of descriptors and call for attention to individual needs and desires. They call us to listen to personal stories, to forces at work within communities, and to reevaluate the languages that enframe mental illness as such.” She goes on to state, “Alternative language beyond the biomedical paradigm of mental illness fosters a diversity of paradigms. Moreover, it can create a reflective space for those with mental suffering (and for their healthcare providers) to see themselves outside of a medical identity, reevaluate their self-care regimens, advocate for the care they would like to receive, and connect to others who may have similar concerns about ascribing to solely psycho-pharmaceutical interventions.”
As of early 2018, Icarus Project staff describe their expertise in social activism, herbalism, and labour organising; none is a licensed medical or mental health professional. Icarus Project advisory board members describe themselves as educators, artists, activists, writers, healers, community organisers, and other creative types and some identify as Latinx, queer, trans, people of colour or mixed race, and trauma survivors; none is a licensed medical or mental health professional. Leadership currently offers publications on self-care and community care, workshops and training for peers, training and talks for providers, peer support spaces, webinars, and other events.
Structure/Funding
The Icarus Project is currently under the fiscal sponsorship of FJC, a non-profit 501(c)3 umbrella organization arm of an investment firm, based in New York City. The Icarus Project currently gets the bulk of its money from foundation grants, including the Ittleson Foundation, but it also has many individual donors.
The Icarus Project Network
Places where local chapters met included Anchorage, Alaska; Asheville, North Carolina; Atlanta, Georgia; Boston, Massachusetts; Conway, Arkansas; Chicago, Illinois; Los Angeles, California (Wildflowers’ Movement); Minneapolis, Minnesota; Madison, Wisconsin; New York City, New York; Northampton, Massachusetts (Freedom Centre); Philadelphia, Pennsylvania; Portland, Oregon; San Francisco (Bay Area), California; Columbus, Ohio; Gainesville, Florida.
Media Mentions
The Icarus Project has been mentioned in passing in The New York Times as a resource for those who “don’t want to ‘get better'”, by Frontline 20/20, and many local media outlets.
Publications
Educational materials published by The Icarus Project have been published in Spanish, German, French, Italian, Japanese, Greek, and Bosnian/Croatian. Some of these publications are listed below:
In March 2004, The Icarus Project released Navigating the Space Between Brilliance and Madness; A Reader and Roadmap of Bipolar Worlds. The book is currently in its 6th printing.
In July 2006, The Icarus Project released the first draft of Friends Make the Best Medicine: A Guide to Creating Community Mental Health Support Networks.
In 2008, The Icarus Project released Through the Labyrinth; A Harm Reduction Guide to Coming Off Psychiatric Drugs, and in 2009 this publication was translated into Spanish and German and made available for free download on the Icarus Project website.
In 2012, The Icarus Project released Mindful Occupation: Rising Up without Burning Out.
In 2015, The Icarus Project released Madness and Oppression: Personal Paths to Transformation and Collective Liberation.
Filmography
Films about Icarus Project members are listed below:
Ken Paul Rosenthal (2010). Crooked Beauty. 30 min. Poetic documentary featuring Jacks McNamara. In Mad Dance Mental Health Film Trilogy.
Ken Paul Rosenthal (2018). Whisper Rapture. 36 min. A doc-opera featuring Bonfire Madigan Shive.
The concept has its origins as far back as the year 1889, when the German psychiatrist Emil Kraepelin first used the term of “periodic mania” to refer to people with recurrent manic episodes and no depression. One year later, Carl Wernicke proposed that mania and depression should be viewed as separate disorders. As the time went on, unipolar mania became an invalid diagnosis due to its variations across different patients. Currently patients with symptoms of mania, even in the absence of any depressive symptoms, would get the bipolar 1 diagnosis.
Symptoms
Symptoms of unipolar mania are similar to those of bipolar mania. They can include:
Excessive involvement in activities with a high likelihood of painful consequences.(e.g. extravagant shopping, improbable commercial schemes, hypersexuality).
The episode generally have a stronger tendency to present with psychosis or/and need psychiatric assistance.
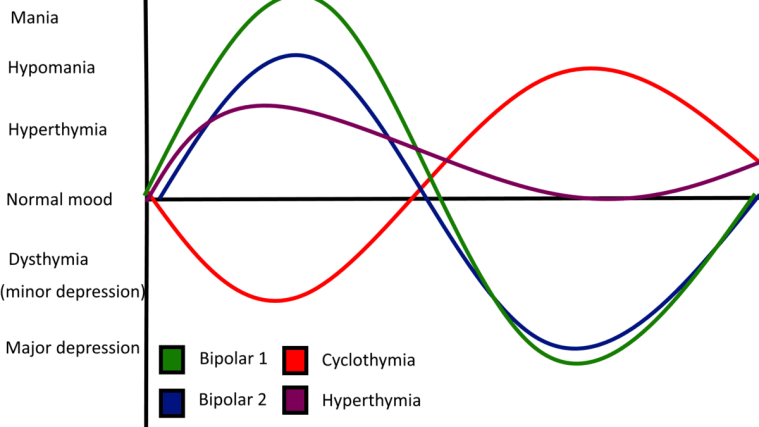
Hyperthymic temperament, or hyperthymia, from Ancient Greek ὑπέρ (“over”, meaning here excessive) + θυμός (“spirited”), is a proposed personality type characterised by an exceptionally, or in some cases, abnormally positive mood and disposition.
Also known as Hyperthymic Personality-Type and Chronic Hypomania.
Graph showing showing hyperthymia in comparison to other bipolar spectrum disorders.
Background
It is generally defined by increased energy, vividness and enthusiasm for life activities, as opposed to dysthymia. Hyperthymia is similar to but more stable than hypomania.
Characteristics of the hyperthymic temperament include:
Increased energy and productivity.
Short sleep patterns.
Vividness, activity extroversion.
Self-assurance, self-confidence.
Strong will.
Extreme talkativeness.
Tendency to repeat oneself.
Risk-taking/sensation seeking.
Breaking social norms.
Very strong libido.
Love of attention.
Low threshold for boredom.
Generosity and tendency to overspend.
Emotion sensitivity.
Cheerfulness and joviality.
Unusual warmth.
Expansiveness.
Tirelessness.
Irrepressibility, irresistible, and infectious quality.
The clinical, psychiatric understanding of hyperthymia is evolving. Studies have shown that hyperthymic temperament promotes efficient performance of complex tasks under time pressure or extreme conditions. Despite this positive characterisation, hyperthymia can be complicated with depressive episodes manifesting as a softer form of bipolar illness, such as cyclothymia. Research also suggests a familial genetic connection of the temperament to bipolar I.
Aside from references in historical and more recent writings on the spectrum of mood disorders, further literature on the temperament is lacking. There is a lack of agreement on its definition, implications or whether it is pathological. It is not known where to place hyperthymia on the affective spectrum.
Hyperthymia manifesting intermittently or in an unusual way may mask hypomania or another psychiatric disorder. Hyperthymia can be most accurately diagnosed by a psychologist or psychiatrist with the help of a patient’s family and/or close friends.
The emphasis of the treatment of bipolar disorder is on effective management of the long-term course of the illness, which can involve treatment of emergent symptoms.
Treatment methods include pharmacological and psychological techniques.
Principles
The primary treatment for bipolar disorder consists of medications called mood stabilisers, which are used to prevent or control episodes of mania or depression. Medications from several classes have mood stabilising activity. Many individuals may require a combination of medication to achieve full remission of symptoms. As it is impossible to predict which medication will work best for a particular individual, it may take some trial and error to find the best medication or combination for a specific patient. Psychotherapy also has a role in the treatment of bipolar disorder. The goal of treatment is not to cure the disorder but rather to control the symptoms and the course of the disorder. Generally speaking, maintenance treatment of bipolar disorder continues long after symptom control has been achieved.
Following diagnostic evaluation, the treating clinician must determine the optimal treatment setting in order to ensure the patient’s safety. Assessment of suicide risk is key, as the rate of suicide completion among those with bipolar disorder may be as high as 10-15%. Hospitalisation should be considered in patients whose judgement is significantly impaired by their illness, and those who have not responded to outpatient treatment; this may need to be done on an involuntary basis. Treatment setting should regularly be re-evaluated to ensure that it is optimal for the patient’s needs.
Mood Stabilisers
Lithium Salts
Lithium salts have been used for centuries as a first-line treatment for bipolar disorder. In ancient times, doctors would send their mentally ill patients to drink from “alkali springs” as a treatment. Although they were not aware of it, they were actually prescribing lithium, which was present in high concentration within the waters. The therapeutic effect of lithium salts appears to be entirely due to the lithium ion, Li+.
Its exact mechanism of action is uncertain, although there are several possibilities such as inhibition of inositol monophosphatase, modulation of G proteins or regulation of gene expression for growth factors and neuronal plasticity. There is strong evidence for its effectiveness in acute treatment and prevention of recurrence of mania. It can also be effective in bipolar depression, although the evidence is not as strong. It is also effective in reducing the risk of suicide in patients with mood disorders.
Potential side effects from lithium include gastrointestinal upset, tremor, sedation, excessive thirst, frequent urination, cognitive problems, impaired motor coordination, hair loss, and acne. Excessive levels of lithium can be harmful to the kidneys, and increase the risk of side effects in general. As a result, kidney function and blood levels of lithium are monitored in patients being treated with lithium. Therapeutic plasma levels of lithium range from 0.5 to 1.5 mEq/L, with levels of 0.8 or higher being desirable in acute mania.
Lithium levels should be above 0.6 mEq/L to reduce both manic and depressive episodes in patients. A recent review concludes that the standard lithium serum level should be 0.60-0.80 mmol/L with optional reduction to 0.40-0.60 mmol/L in case of good response but poor tolerance or an increase to 0.80-1.00 mmol/L in case of insufficient response and good tolerance.
Monitoring is generally more frequent when lithium is being initiated, and the frequency can be decreased once a patient is stabilised on a given dose. Thyroid hormones should also be monitored periodically, as lithium can increase the risk of hypothyroidism.
Anticonvulsants
A number of anti-convulsant drugs are used as mood stabilisers, and the suspected mechanism is related to the theory that mania can “kindle” further mania, similar to the kindling model of seizures. Valproic acid, or valproate, was one of the first anti-convulsants tested for use in bipolar disorder. It has proven to be effective for treating acute mania. The mania prevention and antidepressant effects of valproic acid have not been well demonstrated. Valproic acid is less effective than lithium at preventing and treating depressive episodes.
Carbamazepine was the first anti-convulsant shown to be effective for treating bipolar mania. It has not been extensively studied in bipolar depression. It is generally considered a second-line agent due to its side effect profile. Lamotrigine is considered a first-line agent for the treatment of bipolar depression. It is effective in preventing the recurrence of both mania and depression, but it has not proved useful in treating acute mania.
Zonisamide (trade name Zonegran), another anti-convulsant, also may show promise in treating bipolar depression. Various other anti-convulsants have been tested in bipolar disorder, but there is little evidence of their effectiveness. Other anti-convulsants effective in some cases and being studied closer include phenytoin, levetiracetam, pregabalin and valnoctamide.
Each anti-convulsant agent has a unique side-effect profile. Valproic acid can frequently cause sedation or gastrointestinal upset, which can be minimised by giving the related drug divalproex, which is available in an enteric-coated tablet. These side effects tend to disappear over time. According to studies conducted in Finland in patients with epilepsy, valproate may increase testosterone levels in teenage girls and produce polycystic ovary syndrome in women who began taking the medication before age 20. Increased testosterone can lead to polycystic ovary syndrome with irregular or absent menses, obesity, and abnormal growth of hair. Therefore, young female patients taking valproate should be monitored carefully by a physician. Excessive levels of valproate can lead to impaired liver function, and liver enzymes and serum valproate level, with a target of 50–125 µg/L, should be monitored periodically.
Side effects of carbamazepine include blurred vision, double vision, ataxia, weight gain, nausea, and fatigue, as well as some rare but serious side effects such as blood dyscrasias, pancreatitis, exfoliative dermatitis, and hepatic failure. Monitoring of liver enzymes, platelets, and blood cell counts are recommended.
Lamotrigine generally has minimal side effects, but the dose must be increased slowly to avoid rashes, including exfoliative dermatitis.
Atypical Antipsychotic Drugs
Antipsychotics work best in the manic phase of bipolar disorder. Second-generation or atypical antipsychotics (including aripiprazole, olanzapine, quetiapine, paliperidone, risperidone, and ziprasidone) have emerged as effective mood stabilisers. The evidence for this is fairly recent, as in 2003 the American Psychiatric Press noted that atypical anti-psychotics should be used as adjuncts to other anti-manic drugs because their mood stabilising properties had not been well established. The mechanism is not well known, but may be related to effects on glutamate activity. Several studies have shown atypical antipsychotics to be effective both as single-agent and adjunctive treatments. Antidepressant effectiveness varies, which may be related to different serotonergic and dopaminergic receptor binding profiles. Quetiapine and the combination of olanzapine and fluoxetine have both demonstrated effectiveness in bipolar depression.
In light of recent evidence, olanzapine (Zyprexa) has been US Food and Drug Administration (FDA) approved as an effective monotherapy for the maintenance of bipolar disorder. A head-to-head randomised control trial (RCT) in 2005 has also shown olanzapine monotherapy to be just as effective and safe as lithium in prophylaxis.
The atypical antipsychotics differ somewhat in side effect profiles, but most have some risk of sedation, weight gain, and extrapyramidal symptoms (including tremor, stiffness, and restlessness). They may also increase the risk of metabolic syndrome, so metabolic monitoring should be performed regularly, including checks of serum cholesterol, triglycerides, and glucose, weight, blood pressure, and waist circumference. Taking antipsychotics for long periods or at high doses can also cause tardive dyskinesia – a sometimes incurable neurological disorder resulting in involuntary, repetitive body movements. The risk of tardive dyskinesia appears to be lower in second-generation antipsychotics than in first-generation antipsychotics but as with first-generation drugs, increases with time spent on medications and in older patients.
New Treatments
A variety of other agents have been tried in bipolar disorder, including benzodiazepines, calcium channel blockers, L-methylfolate, and thyroid hormone. Modafinil (Provigil) and Pramipexole (Mirapex) have been suggested for treating cognitive dysfunction associated with bipolar depression, but evidence supporting their use is quite limited. In addition riluzole, a glutamatergic drug used in ALS has been studied as an adjunct or monotherapy treatment in bipolar depression, with mixed and inconsistent results. The selective oestrogen receptor modulator medication tamoxifen has shown rapid and robust efficacy treating acute mania in bipolar patients. This action is likely due not to tamoxifen’s oestrogen-modulating properties, but due to its secondary action as an inhibitor of protein Kinase C.
Cognitive Effects of Mood Stabilisers
Bipolar patients taking antipsychotics have lower scores on tests of memory and full-scale IQ than patients taking other mood stabilisers. Use of both typical and atypical antipsychotics is associated with risk of cognitive impairment, but the risk is higher for antipsychotics with more sedating effects.
Among bipolar patients taking anticonvulsants, those on lamotrigine have a better cognitive profile than those on carbamazepine, valproate, topiramate, and zonisamide.
Although decreased verbal memory and slowed psychomotor speed are common side effects of lithium use these side effects usually disappear after discontinuation of lithium. Lithium may be protective of cognitive function in the long term since it promotes neurogenesis in the hippocampus and increases grey matter volume in the prefrontal cortex.
Antidepressants
Antidepressants should only be used with caution in bipolar disorder, as they may not be effective and may even induce mania. They should not be used alone, but may be considered as an adjunct to lithium.
A recent large-scale study found that severe depression in patients with bipolar disorder responds no better to a combination of antidepressant medications and mood stabilisers than it does to mood stabilisers alone and that antidepressant use does not hasten the emergence of manic symptoms in patients with bipolar disorder.
The concurrent use of an antidepressant and a mood stabiliser, instead of mood stabiliser monotherapy, may lower the risk of further bipolar depressive episodes in patients whose most recent depressive episode has been resolved. However, some studies have also found that antidepressants pose a risk of inducing hypomania or mania, sometimes in individuals with no prior history of mania. Saint John’s Wort, although a naturally occurring compound, is thought to function in a fashion similar to man-made antidepressants, and so unsurprisingly, there are reports that suggest that it can also induce mania. For these reasons, some psychiatrists are hesitant to prescribe antidepressants for the treatment of bipolar disorder unless mood stabilisers have failed to have an effect, however, others feel that antidepressants still have an important role to play in treatment of bipolar disorder.
Side effects vary greatly among different classes of antidepressants.
Antidepressants are helpful in preventing suicides in people suffering from bipolar disorder when they go in for the depressive phase.
NMDA-Receptor Antagonists
In a double-blind, placebo-controlled, proof-of-concept study, researchers administered an N-methyl-d-aspartate-receptor antagonist (ketamine) to 18 patients already on treatment with lithium (10 patients) or valproate (8 patients) for bipolar depression. From 40 minutes following intravenous injection of ketamine hydrochloride (0.5 mg/kg), the researchers observed significant improvements in depressive symptoms, as measured by standard tools, that were maintained for up to 3 days, an effect not observed in subjects who received the placebo. Five subjects dropped out of the ketamine study; of these, four were taking valproate and one was being treated with lithium. One patient showed signs of hypomania following ketamine administration and two experienced low mood. This study demonstrates a rapid-onset antidepressant effect of ketamine in a small group of patients with bipolar depression. The authors acknowledged the study’s limitations, including the dissociative disturbances in patients receiving ketamine that could have compromised the study blinding, and they emphasised the need for further research.
A more recent double-blind, placebo-controlled study by the same group found that ketamine treatment resulted in a similarly rapid alleviation of suicidal ideation in 15 patients with bipolar depression.
Ketamine is used as a dissociative anaesthetic, and is a Class C substance in the United Kingdom; as such, it should only be used under the direction of a health professional.
Dopamine Agonists
In a single controlled study of twenty one patients, the dopamine D3 receptor agonist pramipexole was found to be highly effective in the treatment of bipolar depression. Treatment was initiated at 0.125 mg t.i.d. and increased at a rate of 0.125 mg t.i.d. to a limit of 4.5 mg qd until the patients’ condition satisfactorily responded to the medication or they could not abide the side effects. The final average dosage was 1.7 mg ± .90 mg qd. The incidence of hypomania in the treatment group was no greater than in the control group.
Psychotherapy
Certain types of psychotherapy, used in combination with medication, may provide some benefit in the treatment of bipolar disorders. Psychoeducation has been shown to be effective in improving patients’ compliance with their lithium treatment. Evidence of the efficacy of family therapy is not adequate to support unrestricted recommendation of its use. There is “fair support” for the utility of cognitive therapy. Evidence for the efficacy of other psychotherapies is absent or weak, often not being performed under randomised and controlled conditions. Well-designed studies have found interpersonal and social rhythm therapy to be effective.
Although medication and psychotherapy cannot cure the illness, therapy can often be valuable in helping to address the effects of disruptive manic or depressive episodes that have hurt a patient’s career, relationships or self-esteem. Therapy is available not only from psychiatrists but from social workers, psychologists and other licensed counsellors.
Jungian Therapy
Jungian authors have likened the mania and depression of bipolar disorder to the Jungian archetypes ‘puer’ and ‘senex’. The puer archetype is defined by the behaviours of spontaneity, impulsiveness, enthusiasm or mania and is symbolised by characters such as Peter Pan or the Greek god Hermes. The senex archetype is defined by behaviours of order, systematic thought, caution, and depression and is symbolised by characters such as the Roman god Saturn or the Greek god Kronos. Jungians conceptualise the puer and senex as a coexistent bipolarity appearing in human behaviour and imagination, but in neurotic manifestations appears as extreme oscillations and as unipolar manifestations. In the case of the split puer-senex bipolarity the therapeutic task is to bring the puer and senex back into correlation by working with the patient’s mental imagery.”
Lifestyle Changes
Sufficient Sleep
If sleeping is disturbed, the symptoms can occur. Sleep disruption may actually exacerbate the mental illness state. Those who do not get enough sleep at night, sleep late and wake up late, or go to sleep with some disturbance (e.g. music or charging devices) have a greater chance of having the symptoms and, in addition, depression. It is highly advised to not sleep too late and to get enough high quality sleep.
Self-Management and Self-Awareness
Understanding the symptoms, when they occur and ways to control them using appropriate medications and psychotherapy has given many people diagnosed with bipolar disorder a chance at a better life. Prodrome symptom detection has been shown to be used effectively to anticipate onset of manic episodes and requires high degree of understanding of one’s illness. Because the offset of the symptoms is often gradual, recognising even subtle mood changes and activity levels is important in avoiding a relapse. Maintaining a mood chart is a specific method used by patients and doctors to identify mood, environmental and activity triggers.
Stress Reduction
Forms of stress may include having too much to do, too much complexity and conflicting demands among others. There are also stresses that come from the absence of elements such as human contact, a sense of achievement, constructive creative outlets, and occasions or circumstances that will naturally elicit positive emotions. Stress reduction will involve reducing things that cause anxiety and increasing those that generate happiness. It is not enough to just reduce the anxiety.
Co-Morbid Substance Use Disorder
Co-occurring substance misuse disorders, which are extremely common in bipolar patients can cause a significant worsening of bipolar symptomatology and can cause the emergence of affective symptoms. The treatment options and recommendations for substance use disorders is wide but may include certain pharmacological and nonpharmacological treatment options.
Other Treatments
Omega-3 Fatty Acids
Omega-3 fatty acids may also be used as a treatment for bipolar disorder, particularly as a supplement to medication. An initial clinical trial by Stoll et al. (1999) produced positive results. However, since 1999 attempts to confirm this finding of beneficial effects of omega-3 fatty acids in several larger double-blind clinical trials have produced inconclusive results. It was hypothesized that the therapeutic ingredient in omega-3 fatty acid preparations is eicosapentaenoic acid (EPA) and that supplements should be high in this compound to be beneficial. A 2008 Cochrane systematic review found limited evidence to support the use of Omega-3 fatty acids to improve depression but not mania as an adjunct treatment for bipolar disorder.
Omega-3 fatty acids may be found in fish, fish oils, algae, and to a lesser degree in other foods such as flaxseed, flaxseed oil and walnuts. Although the benefits of Omega-3 fatty acids remain debated, they are readily available at drugstores and supermarkets, relatively inexpensive, and have few known side effects (All of these oils, however, have the capacity to exacerbate GERD (gastroesophageal reflux disease) – food sources may be a good alternative in such cases).
Exercise
Exercise has also been shown to have antidepressant effects.
Electroconvulsive Therapy
Electroconvulsive therapy (ECT) may have some effectiveness in mixed mania states, and good effectiveness in bipolar depression, particularly in the presence of psychosis. It may also be useful in the treatment of severe mania that is non-responsive to medications.
The most frequent side effects of ECT include memory impairment, headaches, and muscle aches. In some instances, ECT can produce significant and long-lasting cognitive impairment, including anterograde amnesia, and retrograde amnesia.
Ketogenic Diet
Because many of the medications that are effective in treating epilepsy are also effective as mood stabilizers, it has been suggested that the ketogenic diet – used for treating paediatric epilepsy – could have mood stabilising effects. Ketogenic diets are diets that are high in fat and low in carbohydrates, and force the body to use fat for energy instead of sugars from carbohydrates. This causes a metabolic response similar to that seen in the body during fasting. This idea has not been tested by clinical research, and until recently, was entirely hypothetical. Recently, however, two case studies have been described where ketogenic diets were used to treat bipolar II. In each case, the patients found that the ketogenic diet was more effective for treating their disorder than medication and were able to discontinue the use of medication. The key to efficacy appears to be ketosis (a metabolic state characterised by elevated levels of ketone bodies in the blood or urine), which can be achieved either with a classic high-fat ketogenic diet, or with a low-carbohydrate diet similar to the induction phase of the Atkins Diet. The mechanism of action is not well understood. It is unclear whether the benefits of the diet produce a lasting improvement in symptoms (as is sometimes the case in treatment for epilepsy) or whether the diet would need to be continued indefinitely to maintain symptom remission.
The Role of Cannabinoids
Acute cannabis intoxication transiently produces perceptual distortions, psychotic symptoms and reduction in cognitive abilities in healthy persons and in severe mental disorder, and may impair the ability to safely operate a motor vehicle.
Cannabis use is common in bipolar disorder, and is a risk factor for a more severe course of the disease by increasing frequency and duration of episodes. It is also reported to reduce age at onset.
Alternative Medicine
Several studies have suggested that omega-3 fatty acids may have beneficial effects on depressive symptoms, but not manic symptoms. However, only a few small studies of variable quality have been published and there is not enough evidence to draw any firm conclusions.
Secondary mania, also known as organic mania, is a variation of bipolar disorder that is caused by physical trauma or illness.
Bipolar disorder has a 1% prevalence rate in the United States and secondary mania is likely a small subset of that percentage. Secondary mania exhibits symptoms similar to that of mania in bipolar I and bipolar II disorders. This includes an elevated mood or affect, psychotic state, accelerated speech, increased motor activity, irritability, and flight ideas. A unique criterion for secondary mania is the lack of history of mental illness that causes mania, such as bipolar disorder. Unlike bipolar disorder, which has an average age of onset at 25 years, secondary mania has an average age of onset at 45 years. Little is known about secondary mania, as much of the research on it is case studies and retrospective accounts. However, it has been connected to several causes such as traumatic brain injury, HIV/AIDS, and stroke.
Closed-Head Injury
One of the primary documented causes of secondary mania is traumatic brain injury, also called closed-head injury. For example, Jorge and colleagues examined the effects of traumatic brain injury and its correlation with secondary mania. They collected participants that in the previous year had had traumatic brain injuries. They did 3, 6, and 12-month follow-ups with the patients where they took psychiatric interviews to measure impairment of daily life, intellectual, and social function. Within the 9% of patients that met the criteria for secondary mania, a correlation between secondary mania and temporal basal polar lesion was found. On average, the duration of secondary mania was 2 months. A second study found that out of 66 patients with a closed head injury, 9% experienced mania during the 12-month period after their injury.
In a case study a 24-year-old man complained of symptoms of mania. He had no prior mental health issues, no family history for mental health disorders, and no history of substance abuse. After a medical examination, he was diagnosed with mania and psychotic symptoms. Soon after he reported having a severe headache and after examination it was found he had a heterogeneous lesion covering most of his left thalamus. After the lesion was discovered, his diagnosis was revised to be “organic mood disorder (left cerebral AVM, Arteriovenous malformation, with secondary mania)”. Another study by Jorge and colleagues looked at the effects of traumatic brain injury and its correlation with secondary mania.
HIV/AIDS
Secondary mania has been associated with HIV/AIDS in a number of cases. According to Ellen and colleagues, secondary mania is reported in 1.2% of HIV-positive patients and 4.3% positive in those with AIDS. In one case study by Chou and colleagues, a 78-year-old man was admitted to the hospital for manic symptoms. “The symptoms included decreased sleep, elevated mood, increased energy, hyperactivity, racing thoughts, and eccentric behaviour”. The patient had no prior history of mental health problems in his family or his own medical records. He was temporarily diagnosed with bipolar one. It was later discovered that he suffered from HIV/AIDS and his diagnosis was altered to secondary mania.
Drugs
Many drugs have direct or indirect effects on neurotransmitters. Steroids are especially proficient at causing changes to the chemistry of neurotransmitters. In a study, 40 women were given steroids to help with their rheumatoid arthritis. Three subjects developed manic symptoms within the first week of taking the steroid. Two had never had a diagnosis of a mental illness, and one of the three women was noted to be “emotionally labile” and had had a suicide attempt but no hospitalisation. It was noted that the mania was not caused by an electrolyte imbalance, but the exact cause was uncertain.
According to Ogawa and Ueki, secondary mania has also been associated with caffeine consumption. A 43-year-old man, with no prior history of mental illness, reportedly switched to drinking 10 cups of coffee a day. After consuming this amount, he was reported to have manic symptoms such as elevated mood, talkativeness, hyperactivity, grandiosity, flight of ideas, and insomnia. This led to his admission into a hospital. After examination, they removed caffeine from the man’s diet, resulting in the cessation of manic symptoms. The doctors then concluded that either the caffeine had acted as a catalyst for bipolar disorder or that he had secondary mania. Unfortunately, little research is done on studying the interaction between mood disorders and caffeine.
Other
A case study by Liang and Yang was of a 75-year-old woman who was admitted to the hospital with fever, chills, headache, and vomiting. Upon doing a mental test, they discovered she had symptoms of mania. However, she had no prior history of mental illness. When speaking with the family they discovered that the symptoms had manifested two weeks prior. Eventually, she was diagnosed with enterococcal meningitis for her physical symptoms and secondary mania for her psychological symptoms. The study stated that the exact link between the secondary mania and the enterococcal meningitis is unknown.
Controversy
Since its first discovery over 30 years ago, secondary mania has been difficult to conceptualise. The primary arguments regarding its aetiology are:
Secondary mania is a form of toxic psychosis rather than actual mania; and
Secondary mania is really latent bipolar disorder that happened to coincide with an injury.
Toxic psychosis is a state which is caused by substance abuse; this could mean being in a confused state from the substance. The main argument against this theory is that mania in general has toxic origins and secondary mania is no different in this regard. However, analyses of secondary mania tend to exclude cases in which the person experienced high levels of confusion. Therefore, stating that it is a toxic state does not take away from the validity of its existence as long as the cases of secondary mania are narrowed to those without the confused state. The second argument is harder to dispute, as it is possible that secondary mania is late-onset bipolar disorder. The way this claim is disputed is through looking at the history of the patient. They check to see if there is a negative pre-morbid history, a lack of history of mental illness, age of onset, and the close proximity of the organic trauma to the mania.




You must be logged in to post a comment.